 |
Case Report
Membranous nephropathy (MN) concurrent chronic inflammatory demyelinating polyneuropathy (CIDP) in a Bangladeshi male
1 Department of Rheumatology, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh
Address correspondence to:
Md Gias Uddin
Department of Rheumatology, Bangabandhu Sheikh Mujib Medical University, Dhaka,
Bangladesh
Message to Corresponding Author
Article ID: 101520Z01MU2025
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Gias Uddin M, Hassan MM, Sohel M, Azad MAK, Hussain KH, Choudhory MR. Membranous nephropathy (MN) concurrent chronic inflammatory demyelinating polyneuropathy (CIDP) in a Bangladeshi male. Int J Case Rep Images 2025;16(2):40–45.ABSTRACT
Introduction: Chronic inflammatory demyelinating polyneuropathy (CIDP) is an acquired autoimmune disorder of the peripheral nervous system, while membranous nephropathy (MN) is a glomerular disease that may develop from exogenous risks or autoimmune conditions. Their coexistence is extremely rare and poorly understood.
Case Report: We report a 55-year-old male from Bangladesh presenting with progressive symmetrical muscle weakness and both motor and sensory impairment in all four limbs. Nerve conduction studies demonstrated features consistent with inflammatory demyelinating polyneuropathy, and cerebrospinal fluid analysis revealed albuminocytological dissociation. The patient also developed nephrotic-range proteinuria; renal biopsy confirmed the diagnosis of membranous nephropathy. He was treated with pulse methylprednisolone and intravenous cyclophosphamide, resulting in improvement in both muscle strength and proteinuria, though sensory deficits persisted.
Conclusion: This rare case of concurrent CIDP and MN suggests a shared autoimmune mechanism involving nerves and kidneys. Early recognition and treatment are essential to prevent irreversible neurological and renal damage, especially in resource-limited settings.
Keywords: Autoimmune overlap syndrome, CIDP, Cyclophosphamide, Membranous nephropathy
Introduction
Chronic inflammatory demyelinating polyneuropathy (CIDP) is an acquired disorder resulting from immune dysfunction that affects the peripheral nervous system. It is a chronic progressive condition that causes symmetrical nerve involvement resulting in motor weakness and sensory disturbances. The immune system attacks the peripheral nerves and causes demyelination of the peripheral nerves [1]. Membranous nephropathy (MN) is an important cause of adult-onset nephrotic syndrome, which is histologically defined as diffuse thickening of the glomerular basement membrane in absence of cellular proliferation. Membranous nephropathy may result from some autoimmune conditions as well as chronic infections and malignancies [2]. The co-occurrence of CIDP and MN is rare. There is a hypothesis that coexistence of such conditions may result from the same autoimmune mechanism. Witte and Burke first described this association in 1987 [3]. Some other case reports and studies have proposed that contactin-1 (CNTN1) and neurofascin-155 (NF155) may be the common antigenic targets and it has a pathogenic role that results in injury to both peripheral nerves and podocytes [4],[5],[6]. The onset of the CIDP generally precedes the MN. Atypical presentation and uncommon associations at presentation sometimes makes the evaluation more critical. The treatment should be started as early as possible to avoid organ damage. But all the necessary diagnostic tools may not be available in some resource constraint countries like Bangladesh. To the best of our knowledge, this is the first reported case of CIDP associated with MN from Bangladesh.
Case Report
A 55-year-old male from Bangladesh presented with gradual, symmetrical weakness in all four limbs over a period of four months. The weakness started insidiously and was more pronounced in the lower limbs. Along with this, he developed tingling and numbness in the distal parts of both upper and lower limbs, which progressively worsened over the same four-month period. After about two months from the onset of symptoms, he observed visible wasting of the thenar and hypothenar muscles of both hands, which significantly impaired his ability to carry out daily activities. One month prior to presentation, he also developed bilateral leg swelling and reported scanty, frothy micturition. His muscle strength was assessed by using the Medical Research Council (MRC) scale. Lower limbs: 3/5 proximally and distally; Upper limbs: 4/5 proximally and distally. Examination of nervous system revealed impaired pain and temperature sensation up to the wrists in the upper limbs and up to the knees in the lower limbs. Vibration and position sense were reduced up to the anterior superior iliac spine. Laboratory investigations (Table 1) showed an elevated C-reactive protein (CRP) level and nephrotic-range proteinuria (5.75 g/day) without active urinary sediment. Serum albumin was low at 28 g/L (reference range: 35–55 g/L). He was not diabetic and his renal and liver functions were normal. His cerebrospinal fluid (CSF) analysis showed albuminocytological dissociation and his CSF protein was 110 mg/dL (Normal <45 mg/dL) with a normal cell count. He was negative for antinuclear antibody, cytoplasmic/perinuclear anti-neutrophil cytoplasmic antibody, hepatitis B surface antigen and anti-hepatitis C virus. Abdominal ultrasonography and computed tomography (CT) scan of chest were unremarkable.
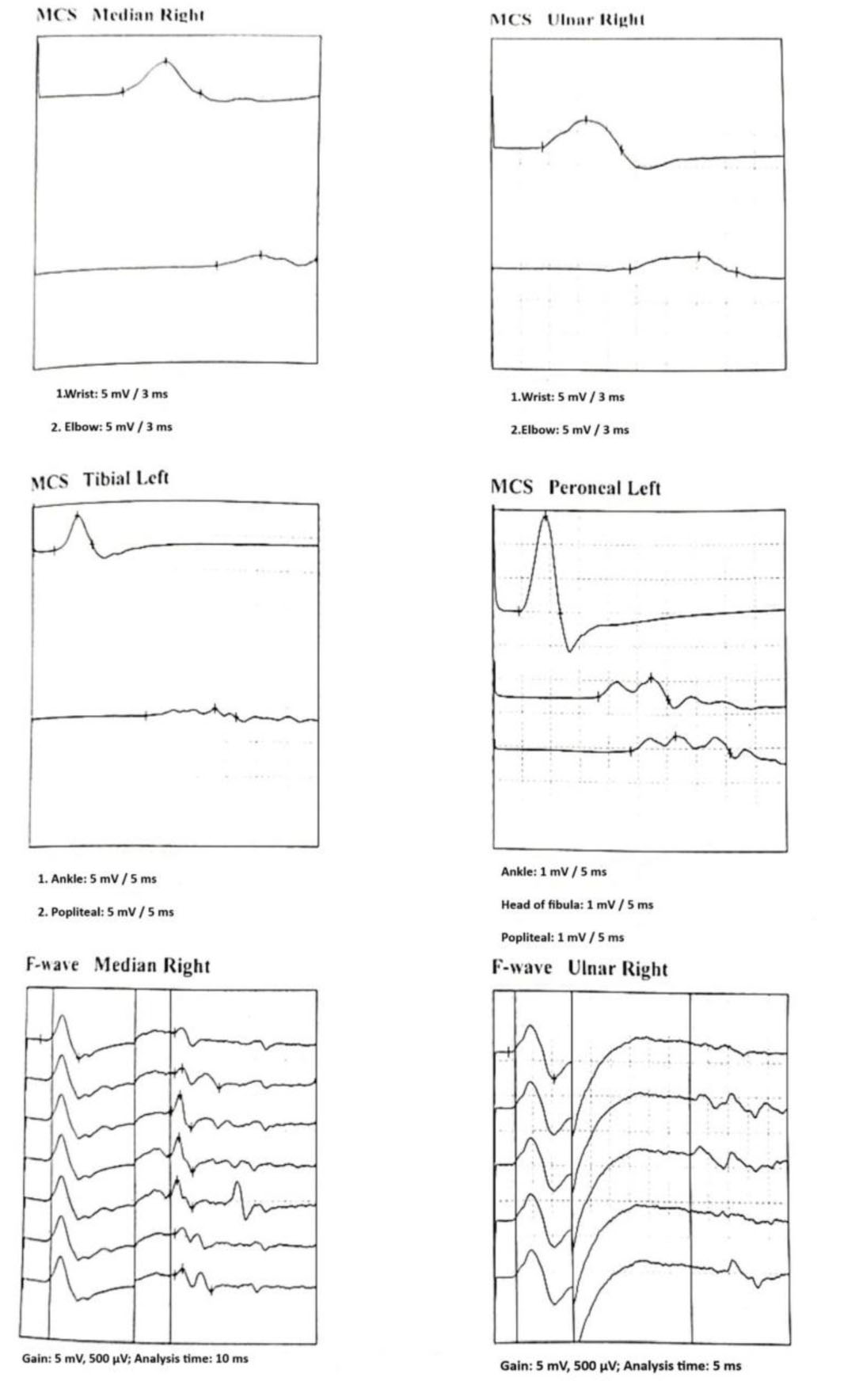
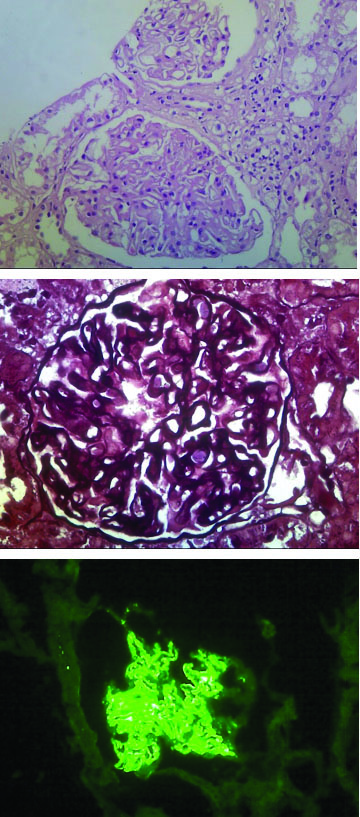
Nerve conduction studies (Figure 1) demonstrated a demyelinating polyneuropathy with the following findings: markedly reduced motor conduction velocities (right median nerve: 23.6 m/s; right ulnar nerve: 27.8 m/s) with prolonged distal motor latencies, decreased motor amplitudes across elbow segments suggesting conduction block, and substantially prolonged F-wave latencies (right median: 51.99 ms; right ulnar: 50.35 ms; left tibial: 78.6 ms—all above upper normal limits). Sensory nerve action potentials were absent in the right median, right ulnar, and left sural nerves. Renal biopsy revealed features consistent with membranous nephropathy. Light microscopy with silver stain (Figure 2A) and hematoxylin and eosin stain (Figure 2B) showed global thickening of the glomerular basement membrane. Immunofluorescence (Figure 2C) showed granular deposits of IgG along the glomerular basement membrane. A clinical diagnosis of CIDP with concurrent MN was made. Autoantibody testing could not be performed due to unavailability in Bangladesh. The patient received pulse methylprednisolone (1 g daily for three days), followed by oral prednisolone (1 mg/kg/day for one month, then gradually tapered), monthly intravenous cyclophosphamide (1 g/m2) was given. Both the muscle power and urinary protein excretion were improved after treatment with 6th cycle cyclophosphamide except sensory deficit.

Discussion
The coexistence of CIDP and MN, although relatively uncommon, but there are few reports in the literatures. It is probably the first case report from Bangladesh and the possibility of an autoimmune mechanism that affects both nerve and glomerulus need to be addressed during management. The clinical presentation showed a clear chronological sequence of neuromuscular and renal symptoms, with neuropathic features preceding nephrotic manifestations. This supports previous observations that CIDP may often precede MN, but it also emphasizes the need for clinicians to remain alert for renal involvement in patients with CIDP [3],[7]. Several studies have suggested that immune dysfunction or molecular mimicry may explain the coexistence of CIDP and MN. In previous reports, autoantibodies such as anti-contactin-1 (anti-CNTN1) and anti-neurofascin-155 (anti-NF155) have been implicated as potential pathogenic factors affecting both peripheral nerves and glomeruli [3],[4],[5],[6].
In our case, antibody testing could not be performed due to unavailability in our country, which limits the ability to confirm this mechanism directly. However, several clinical observations support an immune-mediated pathogenesis: the temporal association of neuromuscular and renal symptoms, the presence of demyelinating features on NCS with CSF albuminocytological dissociation, and the characteristic renal biopsy findings of membranous nephropathy. Moreover, the patient demonstrated a favorable response to combined immunosuppressive therapy (corticosteroids plus cyclophosphamide), with significant motor improvement and reduction of proteinuria, further reinforcing the role of a shared immune mechanism even in the absence of antibody confirmation. The treatment of CIDP includes corticosteroids, intravenous immunoglobulin (IVIG), or plasma exchange. The rapid action and safety of IVIG makes it more superior than the others [8],[9],[10],[11]. Membranous nephropathy is also treated with the Ponticelli regimen or rituximab. When CIDP and MN occur together, treatment strategies vary. First-line options usually include IVIG or rituximab, which have shown good efficacy in several reports [12],[13]. However, in our patient, a combination of corticosteroids and monthly intravenous cyclophosphamide was chosen. The patient’s clinical profile and the financial constraints was the principal determinants in making the choice of therapies. The unavailability of antibody testing and the issue of delay in starting treatment may cause permanent renal and neurological damage made us to consider starting treatment immediately. Fertility preservation was not a great concern as he has already completed his family. This treatment outcome was very satisfactory and there were significant improvements both in motor function and reduced proteinuria. This demonstrates that this approach is effective in settings with limited resources.
The motor function was improved significantly after treatment but sensory symptoms did not. In previous studies this response pattern has been observed. One possibility for this outcome is that irreversible axonal damage may limit full recovery.
Managing chronic conditions require vigilance for rare but severe complications [14]. The occurrence of MN in a patient with CIDP highlights an aggressive systemic autoimmune process, emphasizing the importance of early recognition and intervention to prevent irreversible neurological and renal damage.
Conclusion
This is a rare case report of CIDP and MN that may present concomitantly and the same autoimmune mechanism can simultaneously attack nerves and kidneys. Early detection and treatment are crucial to prevent permanent damage. Experience in managing such disease with rapid diagnosis is essential. Electrophysiological studies and renal biopsy are the cornerstone in diagnosis. Antibody test if available is further helpful for establishing the same pathology.
REFERENCES
1.
Lewis RA. Chronic inflammatory demyelinating polyneuropathy. Curr Opin Neurol 2017;30(5):508–12. [CrossRef]
[Pubmed]

2.
Ponticelli C. Membranous nephropathy. J Clin Med 2025;14(3):761. [CrossRef]
[Pubmed]
3.
Witte AS, Burke JF. Membranous glomerulonephritis associated with chronic progressive demyelinating neuropathy. Neurology 1987;37(2):342–5. [CrossRef]
[Pubmed]
4.
Tang Y, Liu J, Gao F, Hao H, Jia Z, Zhang W, et al. CIDP/autoimmune nodopathies with nephropathy: A case series study. Ann Clin Transl Neurol 2023;10(5):706–18. [CrossRef]
[Pubmed]
5.
Bolz S, Totzeck A, Amann K, Stettner M, Kleinschnitz C, Hagenacker T. CIDP, myasthenia gravis, and membranous glomerulonephritis – Three autoimmune disorders in one patient: A case report. BMC Neurol 2018;18(1):113. [CrossRef]
[Pubmed]
6.
Le Quintrec M, Teisseyre M, Bec N, Delmont E, Szwarc I, Perrochia H, et al. Contactin-1 is a novel target antigen in membranous nephropathy associated with chronic inflammatory demyelinating polyneuropathy. Kidney Int 2021;100(6):1240–9. [CrossRef]
[Pubmed]
7.
Nazarali S, Mathey EK, Tang D, Margetts PJ, Baker SK. Chronic inflammatory demyelinating polyneuropathy and concurrent membranous nephropathy. Can J Neurol Sci 2020;47(4):585–7. [CrossRef]
[Pubmed]
8.
van Schaik IN, Eftimov F, van Doorn PA, Brusse E, van den Berg LH, van der Pol WL, et al. Pulsed highdose dexamethasone versus standard prednisolone treatment for chronic inflammatory demyelinating polyradiculoneuropathy (PREDICT study): A double-blind, randomised, controlled trial. Lancet Neurol 2010;9(3):245–53. [CrossRef]
[Pubmed]
9.
Eftimov F, Winer JB, Vermeulen M, de Haan R, van Schaik IN. Intravenous immunoglobulin for chronic inflammatory demyelinating polyradiculoneuropathy. Cochrane Database Syst Rev 2013;(12):CD001797. [CrossRef]
[Pubmed]
10.
Shah M, DeLaat A, Cavanaugh C. Treatment of membranous nephropathy: Perspectives on current and future therapies. Front Nephrol 2023;3:1110355. [CrossRef]
[Pubmed]
11.
Tarabzuni O. Chronic inflammatory demyelinating polyneuropathy and concurrent membranous nephropathy associated with anti-contactin-1 autoantibodies: A rare case report with a review of the literature. Cureus 2025;17(5):e83975. [CrossRef]
[Pubmed]
12.
Good JL, Chehrenama M, Mayer RF, Koski CL. Pulse cyclophosphamide therapy in chronic inflammatory demyelinating polyneuropathy. Neurology 1998;51(6):1735–8. [CrossRef]
[Pubmed]
13.
Fang Y, Ma X, Ren J, Wang H. Fishnet-like double active layer-loaded carbon fiber for electrical double-layer capacitors. Dalton Trans 2023;52(21):7208–18. [CrossRef]
[Pubmed]
14.
Kanani J, Sheikh MI. An autopsy presentation of spontaneous splenic rupture in chronic myeloid leukemia: A rare case report. J Med Surg Public Health 2024;3:100118. [CrossRef]
SUPPORTING INFORMATION
Author Contributions
Md Gias Uddin - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Md Masudul Hassan - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Mainuddin Sohel - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Mohammad Abul Kalam Azad - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Kassim Hagi Hussain - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Minhaj Rahim Choudhory - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2025 Md Gias Uddin et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}