 |
Clinical Image
Apparent appendicitis in Amyand hernia with unexpected pathology
1 Resident, Department of Internal Medicine, Washington University School of Medicine, Saint Louis, Missouri, USA
2 Resident, Department of Radiology, Washington University School of Medicine, Barnes-Jewish Hospital, Saint Louis, Missouri, USA
3 Scientific Writer, Department of Medical Oncology, Washington University School of Medicine, Saint Louis, Missouri, USA
4 Professor, Department of Medical Oncology, Washington University School of Medicine, Saint Louis, Missouri, USA
Address correspondence to:
Nancy L Bartlett
Washington University School of Medicine, 660 South Euclid, Box 8056, St. Louis, Missouri 63110,
USA
Message to Corresponding Author
Article ID: 101030Z01DG2019
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Russler-Germain DA, Fraum TJ, Watkins MP, Bartlett NL. Apparent appendicitis in Amyand hernia with unexpected pathology. Int J Case Rep Images 2019;10:101030Z01DG2019.ABSTRACT
No Abstract
Keywords: Amyand hernia, Appendicitis, Lymphoma
Case Report
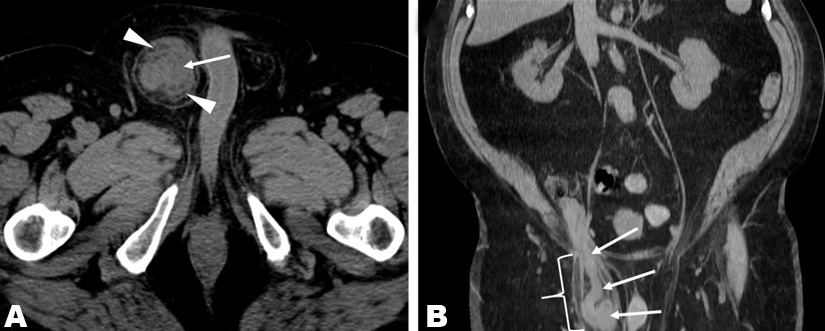
A 70-year-old man with a history of peripheral T-cell lymphoma in complete remission since 2012, presented with a three-week history of a tender ‘knot’ in his right inguinal/suprapubic region. He denied fevers, nausea, vomiting, and constipation. Physical examination was remarkable only for a 4x5 cm firm mass in the right suprapubic region. Complete blood counts and a comprehensive metabolic panel were normal except for a chronically elevated creatinine (1.9 mg/dL) and mildly elevated lactate dehydrogenase (279 units/L). Transaxial (Figure 1A) and coronal (Figure 1B) computed tomography (CT) images, obtained without intravenous contrast, revealed marked appendiceal thickening (arrows) and periappendiceal fat-stranding (arrowheads), suspicious for acute appendicitis. As shown in Figure 1B, the appendix was located within an indirect inguinal hernia sac (bracket), an entity known as an Amyand hernia. There was no evidence of appendiceal perforation. One day later, the patient underwent a laparoscopic appendectomy and open primary right inguinal hernia repair with a post-operative diagnosis of “acute, perforated appendicitis incarcerated within an indirect right inguinal hernia.” In addition to acute- on-chronic inflammation in the hernia sac, pathology revealed diffuse large B-cell lymphoma of the appendix. Subsequent staging by fluorodeoxyglucose (FDG)- PET/CT revealed multiple FDG-avid liver lesions consistent with stage IV lymphoma. The patient subsequently achieved a complete response with R-CHOP chemotherapy.
Discussion
Amyand hernia was first described by the surgeon Claudius Amyand in 1735. It refers to the protrusion of a vermiform appendix in an inguinal hernia sac and occurs in <1% of all inguinal hernias. Appendicitis in an Amyand hernia accounts for <0.1% of all cases of appendicitis [1],[2],[3]. Amyand hernias occur more frequently in male patients, and have a bimodal age distribution with peak incidences in neonates and in patients over 70 years of age [4],[5],[6]. Reports of Amyand hernia predominantly describe preoperative diagnoses made by ultrasound or CT, otherwise diagnosis of Amyand hernias tend to occur intraoperatively [7],[8],[9]. While almost always an indirect hernia, the phenomenon of a direct Amyand hernia has been also described [10]. A four-category classification system has been proposed by Losanoff and Basson to guide staging and management of Amyand hernias [11]. It bases surgical recommendations on the presence or absence of a normal appendix (Stage 1), localized acute appendicitis (Stage 2), peritonitis (Stage 3), or other abdominal pathology (Stage 4). Stage 4 Amyand hernia is a small subgroup of an already rare condition, typically encompassing cases with abscess formation, or alternatively with coexistence of a malignancy, typically a primary appendiceal tumor [12],[13]. The patient described in our case report fits this category with his unexpected diagnosis of diffuse large B-cell lymphoma (DLBCL) of the appendix. The most common site of extranodal involvement of non-Hodgkin lymphoma (NHL) is the gastrointestinal (GI) tract, representing 10–15% of all NHL cases, and ~1/3 of all NHL with any extranodal involvement [14]. Involvement of the appendix is rare, as the most commonly involved sites in the GI tract are the stomach, small intestine, pharynx, colon, and esophagus [14],[15].
Conclusion
Computed tomography (CT) findings of acute appendicitis are nonspecific and that differential diagnoses should be considered when there is an atypical clinical presentation. In this case, the subacute presentation over three weeks and the absence of fever, leukocytosis, or gastrointestinal symptoms were unusual for acute appendicitis.
REFERENCES
1.
Ryan WJ. Hernia of the vermiform appendix. Ann Surg 1937;106:135–9.

2.
Thomas WE, Vowles KD, Williamson RC. Appendicitis in external herniae. Ann R Coll Surg Engl 1982;64(2):121–2.
[Pubmed]
3.
Michalinos A, Moris D, Vernadakis S. Amyand's hernia: A review. Am J Surg 2014;207(6):989–95. [CrossRef]
[Pubmed]
4.
Cankorkmaz L, Ozer H, Guney C, Atalar MH, Arslan MS, Koyluoglu G. Amyand's hernia in the children: A single center experience. Surgery 2010;147(1):140–3. [CrossRef]
[Pubmed]
5.
Meinke AK. Review article: Appendicitis in groin hernias. J Gastrointest Surg 2007;11(10):1368–72. [CrossRef]
[Pubmed]
6.
Srouji MN, Buck BE. Neonatal appendicitis: Ischemic infarction in incarcerated inguinal hernia. J Pediatr Surg 1978;13(2):177–9.
[Pubmed]
7.
Akfirat M, Kazez A, Serhatlioglu S. Preoperative sonographic diagnosis of sliding appendiceal inguinal hernia. J Clin Ultrasound 1999;27(3):156–8.
[Pubmed]
8.
Luchs JS, Halpern D, Katz DS. Amyand's hernia: Prospective CT diagnosis. J Comput Assist Tomogr 2000;24(6):884–6.
[Pubmed]
9.
Kueper MA, Kirschniak A, Ladurner R, Granderath FA, Konigsrainer A. Incarcerated recurrent inguinal hernia with covered and perforated appendicitis and periappendicular abscess: Case report and review of the literature. Hernia 2007;11(2):189–91. [CrossRef]
[Pubmed]
10.
D'Alia C, Lo Schiavo MG, Tonante A, et al. Amyand's hernia: Case report and review of the literature. Hernia 2003;7(2):89–91. [CrossRef]
[Pubmed]
11.
Losanoff JE, Basson MD. Amyand hernia: A classification to improve management. Hernia 2008;12(3):325–6. [CrossRef]
[Pubmed]
12.
Wu CL, Yu CC. Amyand's hernia with adenocarcinoid tumor. Hernia 2010;14(4):423–5. [CrossRef]
[Pubmed]
13.
Lee YT, Wu HS, Hung MC, Lin ST, Hwang YS, Huang MH. Ruptured appendiceal cystadenoma presenting as right inguinal hernia in a patient with left colon cancer: A case report and review of literature. BMC Gastroenterol 2006;6:32. [CrossRef]
[Pubmed]
14.
Paryani S, Hoppe RT, Burke JS, et al. Extralymphatic involvement in diffuse non-Hodgkin’s lymphoma. J Clin Oncol 1983;1(11):682–8. [CrossRef]
[Pubmed]
15.
Caristo G, Griseri G, Fornaro R, et al. Primary lymphoma of appendix presenting as acute appendicitis: A case report. Int J Surg Case Rep 2018;48:30–3. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
David A Russler-Germain - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Tyler J Fraum - Acquisition of data, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Marcus P Watkins - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Nancy L Bartlett - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2019 David A Russler-Germain et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


{kind=link}
{kind=link}
{kind=link}
{kind=link}