 |
Case Report
Primary breast lymphoma in a male
1 Higher Specialist General Surgery Trainee, Department of General and Vascular Surgery, Mater Dei Hospital, St. Paul’s Bay, Malta
2 Specialist Breast and General Surgeon, Department of General and Vascular Surgery, Mater Dei Hospital, St. Paul’s Bay, Malta
3 Consultant Breast and General Surgeon, Department of General and Vascular Surgery, Mater Dei Hospital, St. Paul’s Bay, Malta
Address correspondence to:
Marc Grech
9, Triq id-Duluri, St. Paul’s Bay,
Malta
Message to Corresponding Author
Article ID: 101538Z01MG2026
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Grech M, Ilgun AS, Agius J. Primary breast lymphoma in a male. Int J Case Rep Images 2026;17(1):47–51.ABSTRACT
Introduction: Primary breast lymphoma (PBL) accounts for less than 0.5% of total breast cancers and 1–2% of extranodal non-Hodgkin lymphomas. It mainly affects women, with male presentations being exceedingly rare and underrepresented in the literature. Primary breast lymphoma presents similarly to primary breast carcinoma, posing diagnostic challenges and risks of delaying treatment. This case emphasizes the importance of maintaining a high index of suspicion when assessing male breast lumps.
Case Report: A 68-year-old gentleman presented to his general practitioner with a new left breast lump, present for several weeks, associated with ipsilateral axillary lymphadenopathy. He was referred to the breast clinic, where examination revealed a palpable, solid lesion in the left lower outer quadrant with localized discomfort but no skin or nipple changes. The initial clinical suspicion was that of primary breast carcinoma. Triple assessment demonstrated a lobulated breast lesion measuring 16 × 8 × 14 mm with axillary lymphadenopathy. Sampling of the axillary node showed reactive changes. Core biopsy of the breast lesion revealed grade 3A classic follicular lymphoma. Following multidisciplinary team discussion, the patient was referred to a hematologist. Due to multiple comorbidities, treatment options were carefully considered. He received one cycle of bendamustine and rituximab but subsequently experienced clinical deterioration and elected for palliative care.
Conclusion: Primary breast lymphoma in males is rare and can resemble breast carcinoma at presentation. A high index of suspicion and adherence to triple assessment are essential for accurate diagnosis. A proper multidisciplinary approach should be devised based on patient compliance and clinical condition.
Keywords: Breast cancer, Extranodal lymphoma, Male breast lump, Primary breast lymphoma
Introduction
Lymphomas describe a group of malignancies originating from proliferating lymphatic cells at different stages of maturation. They are broadly classified as Hodgkin’s (10%) or non-Hodgkin’s lymphoma (90%) with the non-Hodgkin’s group further subdivided into B-cell, T-cell, and Natural Killer (NK) cell types. Lymphoma most commonly occurs within lymph nodes with cervical lymphadenopathy being the most commonly reported nodal site of involvement (36.8%) [1]. Patients often present with a palpable lump with associated fever, night sweats, and weight loss. Diagnosis is made by obtaining a tissue biopsy and management often combines chemotherapy, radiotherapy, and antibody-drug conjugates [2].
Breast lymphomas can be classified as primary or secondary breast lymphoma, where primary breast lymphoma indicates a new diagnosis with no previous evidence of lymphoma at diagnosis. Breast cancer in males is a rare entity, accounting for less than 1% of all breast cancer diagnosis [3]. In turn, Primary Breast Lymphoma (PBL) accounts for 0.4% of breast malignancies and 2% of extranodal lymphomas [4]. Few cases of PBL in males have been reported in the literature, there is therefore no data or guidelines available on the subject.
Case Report
A 68-year-old gentleman, residing in a southern Mediterranean country, noted a left breast lump on self-examination, which was confirmed after GP review. He was subsequently referred to the breast clinic and further noted associated left sided axillary lymphadenopathy. The lump had been present for a few weeks prior to seeking medical advice. He has a significant past medical history including history of myocardial ischemia, diabetes, peripheral neuropathy and glaucoma. He is independent at home, however required assistance when leaving the house.
A breast surgeon assessed him, noting a lump in the left lower, outer quadrant, approximately 15 mm in diameter. This was reported to be solid and lobulated with associated discomfort on palpation. The lesion was non-mobile, no skin changes were evident, and he denied any history of nipple changes or discharge. A minimal amount of weight loss was reported, which the patient attributed to a recent increase in diuretic dose. He denied a significant family history of breast cancer. In view of a strong suspicion of breast carcinoma with axillary lymph node metastasis, imaging of the breast lump and lymph nodes was organized, together with biopsies to complete the triple assessment.
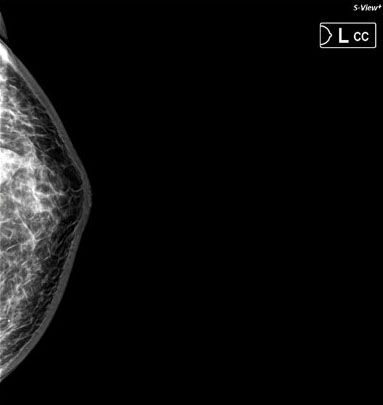
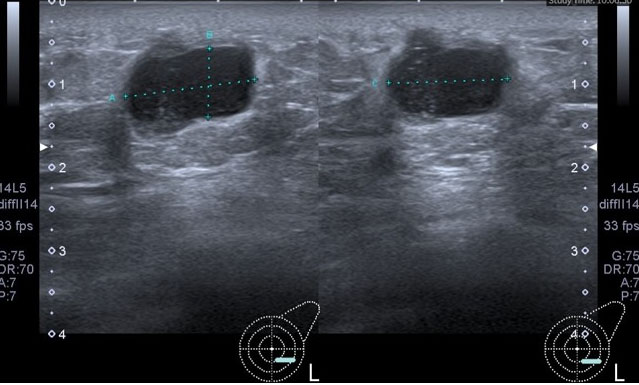
Mammography showed a lobulated, high-density opacity with circumscribed margins in the left lower outer quadrant and associated left axillary lymphadenopathy (Figure 1 and Figure 2). Ultrasound showed a lobulated hypoechoic, hypervascular lesion measuring 16 × 8 × 14 mm. No microcalcifications were reported (Figure 3). A fine-needle aspiration (FNA) of the largest axillary lymph node was performed, yielding a reactive lymph node aspirate. Histology of the breast reported a diffuse neoplastic lymphoid infiltrate with distinctly follicular architecture. The neoplastic follicles were non-polarized, lacked tangible body macrophages and were comprised predominantly of centroblasts, with scattered intervening centrocytes. No areas of diffuse growth or parenchymal necrosis was evident in the cores. Immunohistochemistry revealed strong CD20 expression in the centroblastic population, confirming B-Cell phenotype. A cyclin D1 stain was negative. The Ki67 proliferation fraction in the blast population was 65%. The overall findings were those of a Grade 3A Classic Follicular Lymphoma, according to the WHO classification system for follicular lymphoma.
The case was discussed at the Multiple Disciplinary Team meeting, following which he was referred to the hematology specialist for further investigation and treatment of the lymphoma. His blood picture showed a slightly low white cell count of 3.76 × 109/L, low lymphocytes of 0.94 × 109/L and a hemoglobin of 10.3 g/dL. Other markers were within normal limits. Surgical treatment for breast lymphoma has been shown to offer no survival benefit or protection from recurrence, and therefore referral to the local hematology unit was undertaken. The patient was worked up, and in view of his cardiomyopathy and peripheral neuropathy, was deemed high risk for chemotherapy treatment. Bone marrow biopsy and a computed tomography (CT) of the neck and trunk, together with positron emission tomography-computed tomography (PET-CT) were organized. Computed tomography neck and trunk showed axillary adenopathy while PET scan was suboptimal in view of widespread muscular glucose uptake. The patient refused a repeat PET scan, resulting in some doubt in the staging of the patient. The hematologist emphasized the immediate need for treatment in such cases; however, given the patient’s significant comorbidities, the possibility of a watch-and-wait approach was discussed with the patient and his family.
The patient ultimately opted for treatment with chemotherapy, and he received a cycle of bendamustine 90 mg/m2 and rituximab 375 mg/m2. Despite treatment, he experienced a sharp deterioration in pain management and general condition and opted not to receive further treatment but to receive palliation and Hospice support.
He was referred to a psychologist to aid in processing his diagnosis and dealing with issues related to his end-of-life care. He was also reviewed by an anesthetist pain specialist to optimize pain management, and was prescribed 20 mg of Morphine Sulfate tablets twice daily, with a view to increase the dose as clinically indicated.
A Hospice foundation, providing patient-centered home palliative care, was involved in his care from the start. This involved regular home visits by nurses, general practitioners and specialists according to the patient’s needs. He passed away at home seven months after his initial diagnosis.

Discussion
The majority of male breast lumps are benign, with gynecomastia being the most common cause of breast enlargement in males. Gynecomastia can be confirmed or excluded through proper history taking including a detailed past medical history and drug history and imaging. Other benign causes may include lipomas and sebaceous cysts, and rarely fibroadenomas, breast cysts, and papillomas. Malignant breast lumps follow the female pattern and may include invasive ductal, mucinous and papillary cancers, Paget’s disease, sarcomas, metastasis, and primary or secondary lymphoma. In our patient, the history provided us with a strong suspicion of a sinister process, which was confirmed on subsequent histological reports [5],[6].
Primary breast lymphoma is a rare entity, accounting for less than 1–2% of all non-Hodgkin lymphomas and less than 0.5% of all malignant neoplasms of the breast. It is a rare variant of lymphoma which is of B-cell type in 50% of cases, but may also be follicular lymphoma, mucosa-associated lymphoid tissue lymphoma, or Burkitt lymphoma [5].
Primary breast lymphoma originates in the breast lymphoid tissue, occurring in the absence of a previously identified extramammary lymphoma or disseminated disease. In contrast, secondary breast lymphoma describes an extramammary lymphoma which has metastasized to the breast [7].
Primary breast lymphoma is diagnosed based on criteria proposed by Wiseman and Liao, which state that the primary site of lymphoma presentation should be the breast, the lymphoma should be in close association with the breast tissue, and the patient should have no history or evidence of disseminated disease within six months of diagnosis, while the simultaneous involvement of axillary lymph nodes is considered to be the part of the spectrum of PBL [8]. Our patient fulfilled the above criteria, presenting with a breast lump, and having no evidence of disseminated disease on investigation.
The overwhelming majority of patients with PBL are females; however, there are a few rare reports in males [9]. It is suggested that sex hormones may play an important role in pathogenesis. Additional support for this theory is the relatively high rate (5–20%) of bilateral disease at diagnosis [9]. The influence of sex hormones on lymphocytes has been extensively studied; however, detailed findings are beyond the scope of this review. Estrogen receptors (ERs) are selectively expressed on B lymphocytes, with differential expression of ERα and ERβ. ERβ expression has also been described in Hodgkin and Burkitt lymphoma cell lines as well as in lymphocytes within breast cancer tissue [10]. The activation of the ERβ pathway has an apoptotic and anti-proliferative effect on lymphocytes, but its precise role in lymphomagenesis remains uncertain [11].
Currently, chemo-immunotherapy with consolidation radiation therapy is considered the mainstay in the treatment of PBL, which has shown the most favorable results. Nevertheless, the choice of criteria for combination therapy is still controversial. Most authors advocate for combination chemotherapy for patients with high-grade tumors, axillary lymph node involvement, and central nervous system involvement in primary high-grade breast lymphomas [5]. Luo et al. showed that radiotherapy was not significantly associated with an improved 5-year overall survival and 5-year disease free survival. In this study, 12 patients received local radiotherapy with a dose range of 20–53 Gy (median 36.5 Gy) [5],[11].
In view of the aggressive nature of PBL, high relapse rates are reported, particularly in the central nervous system and in the breast. Some authors therefore advocate for adding central nervous system prophylaxis to systemic treatment [5].
Conclusion
Primary breast lymphoma may closely mimic primary breast carcinoma on clinical and radiological assessment. This case highlights the importance of maintaining a broad differential diagnosis when evaluating male breast lumps. Prompt investigation is essential to establish an accurate histological diagnosis, as management differs significantly from that of primary breast carcinoma and does not routinely involve surgical treatment. A proper multidisciplinary approach should be devised based on patient compliance and clinical condition.
REFERENCES
1.
Laurent C, Do C, Gourraud PA, de Paiva GR, Valmary S, Brousset P. Prevalence of common non-Hodgkin lymphomas and subtypes of Hodgkin lymphoma by nodal site of involvement: A systematic retrospective review of 938 cases. Medicine (Baltimore) 2015;94(25):e987.
[Pubmed]

2.
Jamil A, Mukkamalla SKR. Lymphoma. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2026.
[Pubmed]
3.
Zheng G, Leone JP. Male breast cancer: An updated review of epidemiology, clinicopathology, and treatment. J Oncol 2022;2022:1734049. [CrossRef]
[Pubmed]
4.
Jennings WC, Baker RS, Murray SS, Howard CA, Parker DE, Peabody LF, et al. Primary breast lymphoma: The role of mastectomy and the importance of lymph node status. Ann Surg 2007;245(5):784–9. [CrossRef]
[Pubmed]
5.
Sakhri S, Aloui M, Bouhani M, Bouaziz H, Kamoun S, Slimene M, et al. Primary breast lymphoma: A case series and review of the literature. J Med Case Rep 2023;17(1):290. [CrossRef]
[Pubmed]
6.
Önder Ö, Azizova A, Durhan G, Elibol FD, Akp?nar MG, Demirkaz?k F. Imaging findings and classification of the common and uncommon male breast diseases. Insights Imaging 2020;11(1):27. [CrossRef]
[Pubmed]
7.
Raj SD, Shurafa M, Shah Z, Raj KM, Fishman MDC, Dialani VM. Primary and secondary breast lymphoma: Clinical, pathologic, and multimodality imaging review. Radiographics 2019;39(3):610–25. [CrossRef]
[Pubmed]
8.
James ER, Miranda RN, Turner SD. Primary lymphomas of the breast: A review. JPRAS Open 2022;32:127–43. [CrossRef]
[Pubmed]
9.
Aviv A, Tadmor T, Polliack A. Primary diffuse large B-cell lymphoma of the breast: Looking at pathogenesis, clinical issues and therapeutic options. Ann Oncol 2013;24(9):2236–44. [CrossRef]
[Pubmed]
10.
Shim GJ, Gherman D, Kim HJ, Omoto Y, Iwase H, Bouton D, et al. Differential expression of oestrogen receptors in human secondary lymphoid tissues. J Pathol 2006;208(3):408–14. [CrossRef]
[Pubmed]
11.
Luo H, Yi P, Wang W, Li K, Meng L, Li J, et al. Clinicopathological features, treatment, and prognosis in primary diffuse large B cell lymphoma of the breast: A retrospective study of 46 patients. Med Sci Monit 2019;25:8671–82. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Acknowledgments
Artificial Intelligence, Chat GPT version 5.4 was used in parts of the text solely to aid in grammar correction and in the improvement of sentence structure. All content was reviewed by the authors and the authors take full responsibility for the accuracy and scientific integrity of the paper.
Author ContributionsMarc Grech - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Ahmet Serkan Ilgun - Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
John Agius - Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2026 Marc Grech et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}