 |
Case Report
Superior mesentery artery aneurysm with thrombosis and proximal stenosis in a case with Ehlers–Danlos syndrome
1 Dr, Department of Radiology, Erzurum Regional Training and Research Hospital, Erzurum, Turkey
2 Associate Professor, Faculty of Medicine, Department of Radiology, Ataturk University, Erzurum, Turkey
Address correspondence to:
Mehmet Eren Ozturk
H. Avni Ulas M. Haznedar C. Sagsoz Apt. A blok. No:12, 25240, Erzurum,
Turkey
Message to Corresponding Author
Article ID: 101535Z01MO2026
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Ozturk ME, Yalcin A. Superior mesentery artery aneurysm with thrombosis and proximal stenosis in a case with Ehlers–Danlos syndrome. Int J Case Rep Images 2026;17(1):35–37.ABSTRACT
Introduction: Visceral arterial aneurysms are very rare in the pediatric patient population and might be associated with connective tissue disorders.
Case Report: In this report, we present a 14-year-old male case with a superior mesenteric artery aneurysm with Ehlers–Danlos syndrome detected with computed tomography (CT) angiography. The patient had a history of scoliosis surgery associated with Ehlers–Danlos syndrome. A superior mesenteric artery aneurysm was detected along with a distal partial thrombosis and proximal stenosis. The patient was deceased 24 hours after admission to emergency room (ER) due to a generalized intestinal infarct.
Conclusion: Visceral arterial aneurysms are very rare and associated complications might be fatal in the child population. Computed tomography (CT) angiography imaging provides a fast and accurate diagnosis and can delineate additional prognostic findings.
Keywords: Computed tomography, Ehlers–Danlos, Intestinal ischemia, Superior mesenteric artery aneurysm stenosis, Thrombosis
Introduction
Arterial aneurysms of the major arteries are common in the adult population. However, aneurysms involving the visceral arteries are rare with an incidence of 0.01% [1],[2]. Superior mesenteric artery (SMA) related aneurysms constitute a small portion of the visceral aneurysms and have a mortality rate up to 35% [3]. Visceral arterial aneurysms are very rare in the pediatric patient population and might be associated with connective tissue disorders [4]. In this report, we present a peculiar case with SMA aneurysm, distal partial thrombosis and proximal stenosis in a 14 years old male detected by computed tomography angiography (CTA).
Case Report
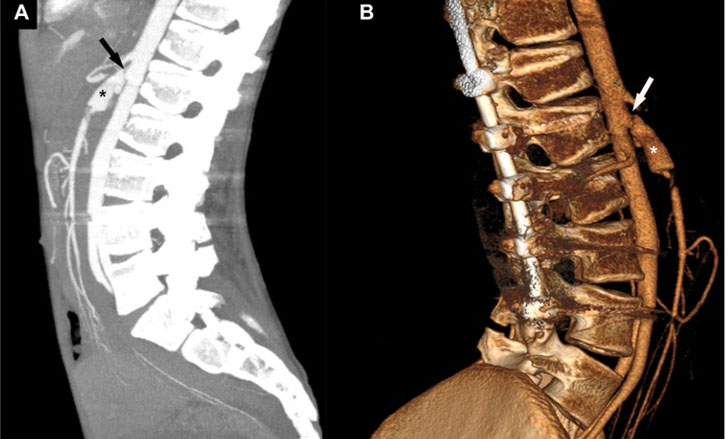
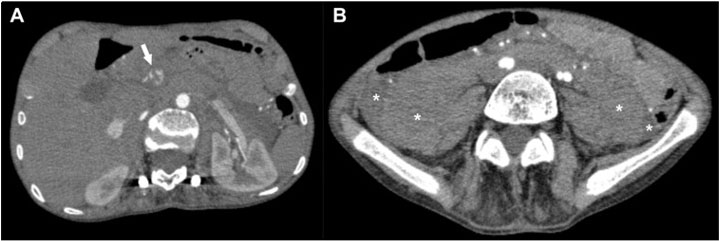
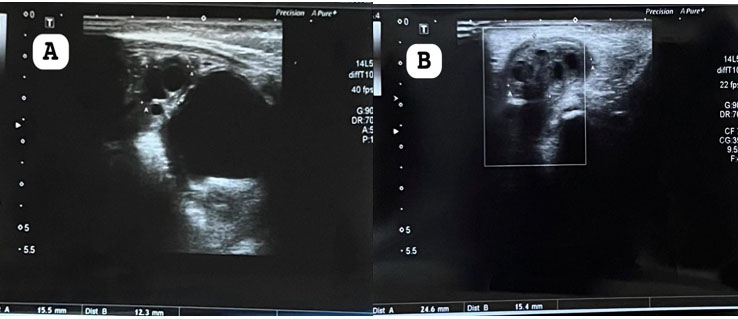
A 14-year-old patient presented to the emergency department complaining of sudden onset of cramping abdominal pain around the navel and deterioration in general condition 6 hours prior. He had a previous scoliosis operation at the age of 10 and diagnosis of Ehlers–Danlos type IV disease. On initial examination, the skin was moist and pale, blood pressure was hypotensive at 85/45 mmHg, pulse was 125 indicating tachycardia, and respiratory rate was 24 indicating tachypnea. Abdominal examination showed tenderness and rebound. Abdominal ultrasound showed collection of fluid in the peritoneal cavity and an abnormal dilated vessel anterior to the aorta. Doppler examination showed vascular color-coding consistent with vascular filling in the abnormal dilated vessel. The patient was referred to the CT unit for the detailed evaluation of abdominal circulation by contrast-enhanced CTA. On CT images, a proximal stenotic segment and aneurysm of the SMA was detected (Figure 1A and Figure 1B). A partial thrombus was detected distal to the dilated segment (Figure 2A). More caudal images showed intraperitoneal fluid and hypoperfusion of ileal and jejunal loops (Figure 2B). The patient underwent laparotomy in which subtotal intestinal ischemia was detected. The patient deceased in post-operative intensive care unit due to generalized intestinal infarct at 24 hours after admission to ER.
Discussion
Our case had proximally orientated SMA aneurysm and the distal thrombus which were concluded with fatal intestinal ischemia. Our case also had a stenotic segment proximal to the aneurysm. The formation of visceral aneurysms distal to the stenotic segment has been associated with high and low wall shear stress theories. These theories may explain the pathophysiology of the visceral aneurysm that formed distal to the stenotic segment in our case [5].
Pediatric non-aortic arterial aneurysms are extremely uncommon. Several factors such as infection, trauma, connective tissue diseases, noninfectious arteritis, or congenital vascular malformations are responsible for the development of aneurysm in the child population [6]. Aneurysms involving the visceral arteries are extremely rare in the pediatric population. These aneurysms can be due to fungal or bacterial infection, noninfectious inflammatory disease, or connective tissue disorders [7],[8]. Except for connective tissue related syndromes such as Ehlers–Danlos type IV disease, surgical repair is the main treatment option. However, in cases with Ehlers–Danlos syndromes, surgery is not preferable due to fragility of the vessels and ligation of the dilated vessel is advised [7],[9].
Our patient had a history of scoliosis operation and diagnosed with Ehlers–Danlos syndrome. Furthermore, the patient had a pre-aneurysmal stenotic segment and thrombosis in the distal segment of the aneurysm. Detection of thrombosis was important as it determined the fate of our patient. Thrombosis of the celiac axis was reported in another case who had type IV Ehlers–Danlos and underwent an operation of correction of scoliosis. In that case, authors associated the thrombosis with surgery [10].
Contrast-enhanced CT angiography was extremely useful in this case, as it showed both the aneurysm and distal thrombus which allowed the surgeons to take necessary steps after definitive diagnosis. Doppler ultrasound imaging was used as a first step imaging method without radiation exposure. The diagnosis was made quickly and accurately in the emergency room, but the patient’s delay in presenting for treatment 6 hours later delayed the early diagnosis and revascularization that are crucial in mesenteric ischemia, leading to the patient's death due to intestinal necrosis [11].
Conclusion
Visceral arterial aneurysms are very rare and associated complications might be fatal in the child population. Computed tomography angiography imaging provides a fast and accurate diagnosis and can delineate additional prognostic findings.
REFERENCES
1.
Subbaraj L, Beleniski F, Courtier J, Vartanian S, Nijagal A. Congenital superior mesenteric artery aneurysm in a 6-week-old infant presenting with upper gastrointestinal bleeding. J Vasc Surg 2020;71(4):1391–4. [CrossRef]
[Pubmed]

2.
Huang YK, Hsieh HC, Tsai FC, Chang SH, Lu MS, Ko PJ. Visceral artery aneurysm: Risk factor analysis and therapeutic opinion. Eur J Vasc Endovasc Surg 2007;33(3):293–301. [CrossRef]
[Pubmed]
3.
Cumbie TA, Kedora JC, Pearl GJ, Shutze WP. A hybrid repair of a superior mesenteric artery pseudoaneurysm using open mesenteric bypass and endovascular exclusion. Proc (Bayl Univ Med Cent) 2015;28(3):355–7. [CrossRef]
[Pubmed]
4.
Chadha M, Ahuja C. Visceral artery aneurysms: Diagnosis and percutaneous management. Semin Intervent Radiol 2009;26(3):196–206. [CrossRef]
[Pubmed]
5.
Li S, Sun X, Chen M, Ma T, Liu X, Zheng Y. Patient-specific modeling of hemodynamic characteristics associated with the formation of visceral artery aneurysms at uncommon locations. Front Cardiovasc Med 2022;9:1008189. [CrossRef]
[Pubmed]
6.
Davis FM, Eliason JL, Ganesh SK, Blatt NB, Stanley JC, Coleman DM. Pediatric nonaortic arterial aneurysms. J Vasc Surg 2016;63(2):466–76.e1. [CrossRef]
[Pubmed]
7.
Ruddy JM, Dodson TF, Duwayri Y. Open repair of superior mesenteric artery mycotic aneurysm in an adolescent girl. Ann Vasc Surg 2014;28(4):1032.e21–4. [CrossRef]
[Pubmed]
8.
de Leeuw K, Goorhuis JF, Tielliu IFJ, Symoens S, Malfait F, de Paepe A, et al. Superior mesenteric artery aneurysm in a 9-year-old boy with classical Ehlers-Danlos syndrome. Am J Med Genet A 2012;158A(3):626–9. [CrossRef]
[Pubmed]
9.
Sheppard DG, Wilkinson AG. Syndrome of idiopathic childhood aneurysms: A case report and review of the literature. J Vasc Interv Radiol 2000;11(8):997–1004. [CrossRef]
[Pubmed]
10.
Debnath UK, Sharma H, Roberts D, Kumar N, Ahuja S. Coeliac axis thrombosis after surgical correction of spinal deformity in type VI Ehlers-Danlos syndrome: A case report and review of the literature. Spine (Phila Pa 1976) 2007;32(18):E528–31. [CrossRef]
[Pubmed]
11.
Teixeira S, Sá Pinto P, Silva I, Veiga C, Almeida R. Acute mesenteric ischemia: The importance of early diagnosis and aggressive revascularization. [Article in Portuguese]. Rev Port Cir Cardiotorac Vasc 2015;22(4):225–30.
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Mehmet Eren Ozturk - Conception of the work, Design of the work, Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Ahmet Yalcin - Conception of the work, Design of the work, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2026 Mehmet Eren Ozturk et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}