 |
Case Report
Multimodality imaging of multiple cardiac myxomas
1 Limoges University Hospital, Limoges, France
Address correspondence to:
Djeinaba Kane
Limoges University Hospital, Limoges,
France
Message to Corresponding Author
Article ID: 101532Z01DK2026
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Kane D, Fikani A, Jouan J. Multimodality imaging of multiple cardiac myxomas. Int J Case Rep Images 2026;17(1):23–26.ABSTRACT
Myxoma is the most common primary cardiac tumor in adults, but remains rare. Most myxomas are located in the left atrium. The clinical expressions are non-specific and very variable. The treatment is essential from the diagnosis given its severe complications, in particular embolic. We present a case of a 48-year-old male patient who presented with two masses in left atrium and left ventricle compatible with a myxoma. The patient underwent complete resection of all the two tumors without incident and the post-operative course was uneventful.
Keywords: Cardiac tumor, Complications, Myxomas
Introduction
Myxoma is the most common primary cardiac tumor in adults, but remains rare. Most myxomas (75%) are located in the left atrium. The clinical expressions are non-specific and very variable according to the anatomical forms. Transthoracic echocardiography may easily do the diagnosis with in some cases no need of other explorations. The treatment is essential from the diagnosis given its severe complications, in particular embolic.
We present a case of a 48-year-old male patient with a medical history of abdominal myxoma who presented with two masses in left atrium and left ventricle, compatible with myxomas.
The patient underwent complete resection of all the tumors without incident and the post-operative course was uneventful.
Case Report
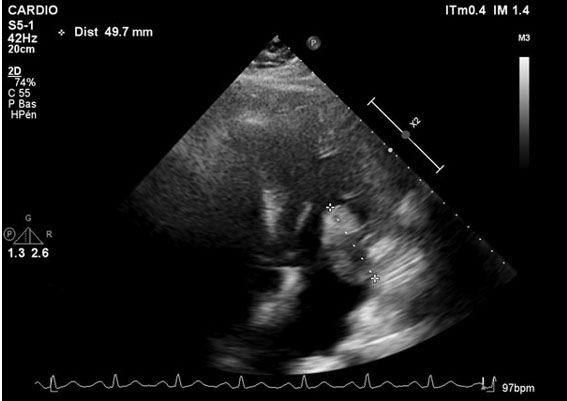
We describe the case of a 48-year-old patient with a past surgical history of right anterior abdominal wall myxoma resection, who currently presented with an asymptomatic heart murmur. His echocardiogram and transesophageal echocardiogram (TEE) revealed two polylobar mobile masses in the left cavities, the biggest one inserted on the lateral wall of the left atrium measuring 55 mm × 30 mm, prolabing in the mitral orifice during diastole (Figure 1). The other was 30 mm × 14 mm pedunculated and lied on the left ventricle lateral wall, at the level of the anterior papillary muscle (Figure 2).
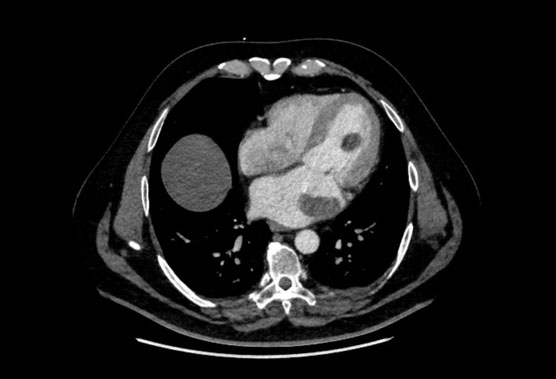
Cardiac computed tomography (CT) scan confirmed the echocardiographic findings, showing a bilobar hypodense left atrial mass, and another mass attached to the anterior papillary muscle (Figure 3).
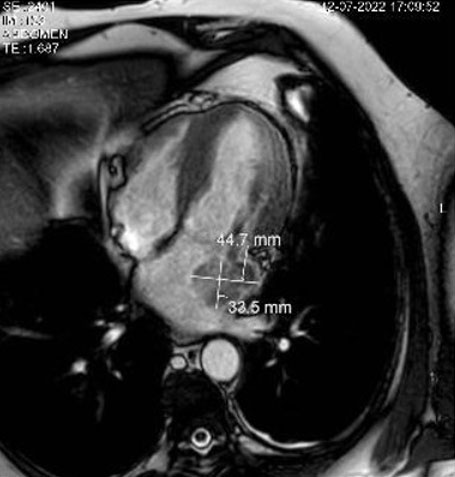
Magnetic resonance imaging (MRI) showed a heterogeneous aspect of both masses with T1 contrast enhancement (Figure 4 and Figure 5).
Surgery was performed via a right anterolateral video-assisted thoracotomy. The most voluminous tumor occupied one third of the atrial volume, was pedunculated, with a large and extremely fibrous implantation base. A second smaller intra-auricular calcified tumor was found after complete resection of the previous one. Its implantation base set on the posterior mitral annulus. The intraventricular tumor was developed on the anterior papillary muscle. Total excision of all tumors was performed. The post-operative course was uneventful.
The anatomopathological results confirmed that the three tumors were benign tumors with the characteristics of myxoma: a myxoid stroma with scattered stellate cells, there was no necrosis.
Follow-up was performed with a clinical examination and echocardiography, which revealed no recurrence. The patient remained asymptomatic.


Discussion
Primary cardiac tumors are extremely rare. Cardiac myxomas are rare tumors representing 0.5% to 1%, it is by far the most common benign primary tumors [1]. Left atrium represents 75% to 90% of myxomas locations, 15% to 20% of myxomas are right atrial location, implantation is mainly on the interatrial septum [1],[2]. The other locations of myxoma are very rare. In rare cases abdominal myxomas has been described, in particular myxoma of the small intestine [2]. Z. Zhang et al. described a case of giant retroperitoneal myxoma [3].
Multiple location of myxomas can let us think about of carney syndrome, and may us do a genetic looking [4].
Our patient has surgical history of the right abdominal wall myxoma 17 years ago and underwent surgical resection. Left ventricular myxoma is rare, and the both localization in left ventricle and left atrium myxoma at the same time has reported once by Xiang Ji et al. [5].
In our case the patient had two masses, one in the left ventricle and one in the left atrium.
The classic triad of symptoms, including obstructive, embolic, and constitutional symptoms is the common manifestation of a cardiac myxoma. It is a pathology which is characterized by a very large clinical polymorphism which can cause a diagnostic delay.
The clinical appearance of myxoma varies from non-specific to life-threatening complications, such as stroke, acute heart failure, or even sudden death [6].
A cerebrovascular complication such as a neurological deficit or sensory impairment as an onset symptom may prompt a suspicion of a cardiac myxoma much earlier.
Although most patients present with one or more elements of the clinical triad comprising impairment of general health, embolic events and syndromes of valvular obstruction or cardiac chambers, cases of totally asymptomatic myxomas have been reported. Our patient was completely asymptomatic. The positive diagnosis of myxoma is essentially based on echocardiography.
Surgically, the tumor resection must be complete, taking away the myxoma, its pedicle and its implantation base, and all with a minimum of manipulation in order to avoid any fragmentation and any risk of embolic migration. Early mortality is low, less than 5%. Late morbidity is dominated by the risk of tumor recurrence and the occurrence of distant metastases [7]. The frequency of these tumor recurrences is around 2% [1]. It is important to insist on a perfect surgical technique to prevent any risk of recurrence as well as on a regular follow up of any patient operated on for cardiac myxomas. Surgical resection has to be complete, to avoid any recurrence.
Conclusion
Cardiac myxomas are rare and the most common primary cardiac neoplasm with a various clinical symptoms. Cardiac myxomas with multiple locations are also very rare. The diagnosis of cardiac myxoma is mainly based on echocardiography. Its treatment is always surgical, with low morbidity and mortality. In the long term, the evolution is usually favorable; however, recurrence remains possible justifying regular follow-up.
REFERENCES
1.
Riberi A, Gariboldi V, Grisoli D, Collart F. Cardiac tumors. [Article in French]. Rev Pneumol Clin 2010;66(1):95–103. [CrossRef]
[Pubmed]

2.
Maghbool M, Samizadeh B. Small intestinal myxoma presented with bowel obstruction, a rare case report. Int J Surg Case Rep 2022;95:107180. [CrossRef]
[Pubmed]
3.
Zhang Z, Song L, Zhu X, Huang Z, Chen J, Zeng Q. Giant retroperitoneal myxoma: A case report and literature review. Int J Surg Case Rep 2021;84:106055. [CrossRef]
[Pubmed]
4.
McCluggage WG, Walsh MY, Thornton CM, McClelland HR, Irwin ST. Massive abdominal and pelvic myxoma in Carney’s syndrome. J Clin Pathol 2000;53(7):558–60. [CrossRef]
[Pubmed]
5.
Ji X, Zhang X. Left atrial myxoma with left ventricular myxoma diagnosed by ultrasound examination: A case report. Medicine (Baltimore) 2021;100(32):e26903. [CrossRef]
[Pubmed]
6.
Qin W, Wang L, Chen X, Liu P, Wang R. Left ventricular myxoma: A case report. J Biomed Res 2014;28(6):506–8. [CrossRef]
[Pubmed]
7.
Varsamis N, Tavlaridis T, Lostoridis E, Tziastoudi E, Salveridis N, Chatzipourgani C, et al. Myxoma of the small intestine complicated by ileo-ileal intussusception: Report of an extremely rare case. Int J Surg Case Rep 2013;4(7):609–12. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Djeinaba Kane - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Amine Fikani - Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Jerome Jouan - Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2026 Djeinaba Kane et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}