 |
Case Report
Treatment of extensive endobronchial granulation tissue with cryotherapy and coagulation after foreign body aspiration: A case report
1 MD, Resident in Pulmonary Medicine, Department of Pulmonary Medicine, UZ Leuven, Leuven, Belgium
2 MD, Pulmonologist, Department of Pulmonary Medicine, AZ Turnhout, Turnhout, Belgium
Address correspondence to:
Lyndon Sprenghers
Herestraat 49, 3000 Leuven,
Belgium
Message to Corresponding Author
Article ID: 101531Z01LP2026
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Sprenghers L, Driesen P. Treatment of extensive endobronchial granulation tissue with cryotherapy and coagulation after foreign body aspiration: A case report. Int J Case Rep Images 2026;17(1):18–22.ABSTRACT
Introduction: Aspiration of foreign bodies is relatively uncommon in adults but may cause significant morbidity because of the formation of granulation tissue. This granulation tissue can cause complications, for example, airway obstruction, hemoptysis, and post-obstructive infections.
Case Report: We present the case of a 63-year-old man with dyspnoea and hemoptysis. Computed tomography (CT) thorax showed a foreign body in the bronchus intermedius. Upon removal of the foreign body, extensive granulation tissue was found, causing bronchial obstruction. The granulation tissue was successfully treated with cryotherapy and coagulation. After cryotherapy, the patient was admitted because of a post-obstructive pneumonia caused by airway obstruction due to necrotic tissue. This necrotic tissue was removed during repeat bronchoscopy.
Conclusion: Granulation tissue should only be removed when bronchial obstruction occurs. A stepwise approach is advised after removal of a foreign body when residual granulation tissue is present. Our case highlights this stepwise approach of conservative management with active follow-up. When bronchial obstruction is present, the granulation tissue should be removed. Interventional techniques such as cryotherapy or coagulation are effective. Cryotherapy causes necrotic tissue that will heal over time. However, this necrotic tissue can cause airway obstruction which can lead to post-obstructive pneumonia. This is a known delayed complication of cryotherapy and needs immediate re-intervention to clear the airways. Our case highlights the potential delayed complication of cryotherapy as well.
Keywords: Bronchoscopy, Coagulation, Cryotherapy, Foreign body aspiration
Introduction
Aspiration of foreign bodies is more frequent in children than it is in adults. In adults, it is relatively uncommon but may cause significant morbidity. Granulation tissue forms around retained foreign bodies, particularly when they are present for extended periods. This granulation tissue can cause complications, for example, airway obstruction, hemoptysis, and retro-obstructive infections. While immediate removal of foreign bodies is advised, removal of granulation tissue is not always necessary. Intervention is indicated in patients with symptomatic obstruction. It is important to recognise that therapeutic bronchoscopy itself may lead to post-procedural complications, for example, airway obstruction by necrotic debris or post-obstructive pneumonia. These complications require immediate reassessment.
This case report illustrates the importance of a stepwise management strategy (Table 1). Granulation tissue is best left untreated, unless bronchial obstruction occurs. Repeat bronchoscopy should be performed when infection develops after intervention.
Case Report
We present the case of a 63-year-old man who presented to our outpatient clinic. His past medical history included arterial hypertension, COPD GOLD II/B, unprovoked pulmonary embolism treated with rivaroxaban, and prostate adenocarcinoma with bone and lymphatic metastases. For the prostate adenocarcinoma, he was initially treated with surgical castration and docetaxel. Because of progressive disease with the development of lung metastases, he was started on abiraterone. The patient was an active smoker.
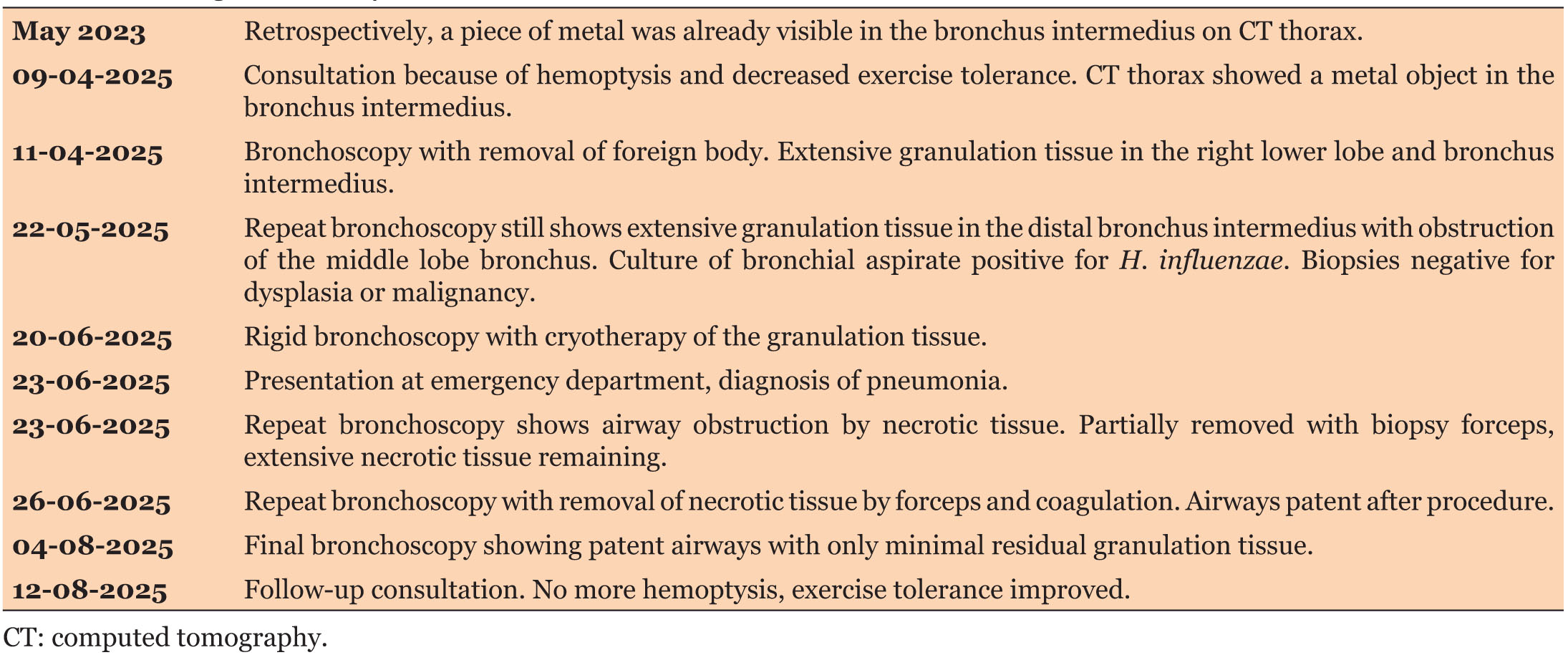
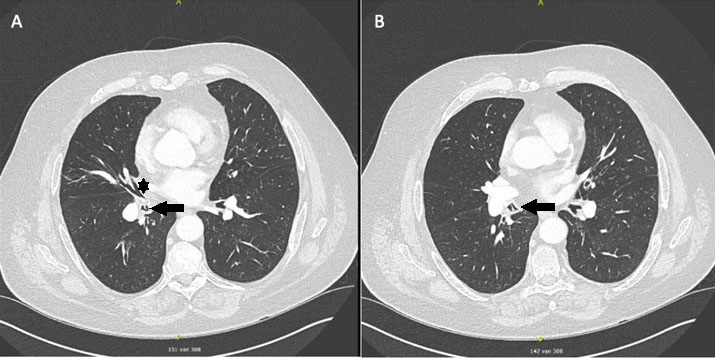
The man presented with hemoptysis and decreased exercise tolerance for the past several weeks. He denied fever, chills, or night sweats. He did not report any thoracic pain or any other complaints. Clinical examination was unremarkable. A computed tomography (CT) scan of the thorax showed no masses or consolidations; it showed a known subpleural nodule in the apex of the left upper lobe, a partial atelectasis of the middle lobe and a foreign body in the bronchus intermedius (Figure 1 and Figure 2).
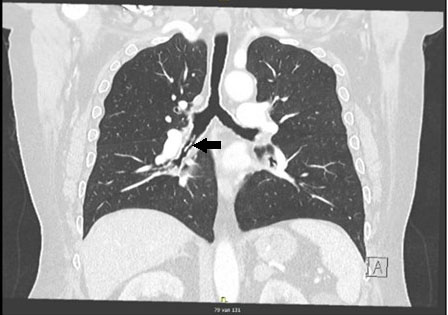
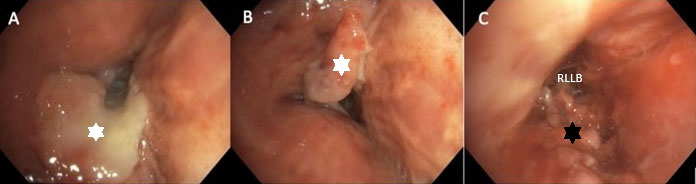
A flexible bronchoscopy was performed because of the hemoptysis and the foreign body, it showed dynamic collapse of the airways and a foreign body in the right lower lobe (Figure 3A). The foreign body was removed with a basket and appeared to be a piece of metal, presumably a part of a soda can (Figure 3B and Figure 3C). Inspection after removing the object showed extensive granulation tissue in the right lower lobe (Figure 3D and Figure 3E). Retrospectively, the piece of metal was also visible on an earlier CT scan from May 2023. A follow-up bronchoscopy was scheduled to confirm whether the granulation tissue would resolve.
Follow-up bronchoscopy six weeks later showed residual granulation tissue obstructing the middle lobe bronchus. Biopsy excluded malignancy. Bronchial aspirate culture showed Haemophilus influenzae, for which amoxicillin-clavulanic acid was started. Because of the obstruction of the middle lobe bronchus, we performed a rigid bronchoscopy with cryotherapy to remove the granulation tissue. Rigid bronchoscopy was performed under general anaesthesia with jet ventilation. We used contact cryoablation, where a freeze phase is followed by a passive thaw phase. We used around 10 cycles of cryoablation, each cycle followed by inspection with flexible bronchoscopy to check for complications and residual granulation tissue. Contact time was a couple of seconds. During cryotherapy, no precautions were taken to prevent airway fire, as there is no airway fire risk. There were no immediate post-procedural complications. A follow-up bronchoscopy was scheduled after six weeks.
Three days later, the patient presented to our emergency department because of fever and increased shortness of breath. Since a couple of days the man was experiencing general malaise, dyspnoea and a productive cough. He had a high fever up to 39.2 °C. Clinically, there was tachypnoea with an oxygen saturation of 89%, and there were crackles over the lower right lung. Biochemically, there was inflammation with CRP (C-reactive protein) of 51.6 mg/L. Arterial blood gas showed hypoxemia with respiratory alkalosis. Chest X-ray showed an infiltrate in the right lower lobe. The diagnosis of pneumonia was made, and the patient was started on amoxicillin-clavulanic acid. Because the pneumonia developed shortly after the rigid bronchoscopy with cryotherapy, a repeat bronchoscopy was performed.
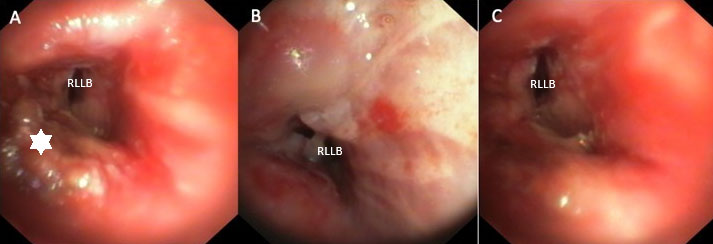
Bronchoscopy showed total occlusion of the bronchus intermedius by necrotic tissue (Figure 4A and Figure 4B). The necrotic tissue was partially removed with a biopsy forceps; upon removal, there was drainage of pus. Only partial opening of the bronchus intermedius was obtained with visualisation of two of the basal bronchial branches. Extensive necrotic tissue and granulation tissue remained, for which a flexible bronchoscopy with coagulation was performed (Figure 4C). With flexible bronchoscopy, all necrotic tissue was removed with forceps. The remaining granulation tissue was removed with coagulation, obtaining complete clearance and patent bronchi (Figure 5A, Figure 5B, Figure 5C). We used probe electrocautery to coagulate the tissue. To reduce the risk of airway fire, we used a grounding pad to the patient, a low FiO2 (<40%) and we coordinated with the anaesthesiologist to stop jet ventilation when coagulating. The patient recovered further with antibiotics and was discharged after three days.
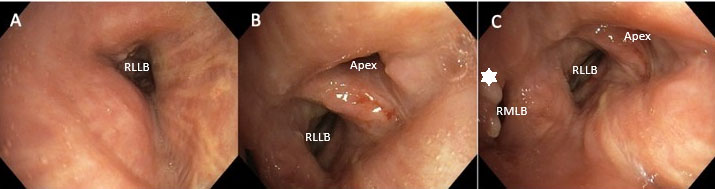
Follow-up bronchoscopy after six weeks showed a good post-procedural result; there was only little remaining granulation tissue (Figure 6A, Figure 6B, Figure 6C). The dyspnoea and hemoptysis resolved; there were no other complaints.
Discussion
Foreign body aspiration is a common cause of granulation tissue formation, particularly when the foreign body is present for extended periods. Foreign bodies should always be removed as quickly as possible [1],[2],[3]. Although granulation tissue can cause complications, it usually does not require immediate intervention. Conservative management can be sufficient, unless there is bronchial obstruction or airway stenosis, or hemoptysis. In those cases, interventional bronchoscopic techniques such as cryotherapy, laser, or coagulation can be used [4],[5].
In our patient, the granulation tissue obstructed the middle lobe bronchus. Therefore, we performed rigid bronchoscopy with cryotherapy. Cryotherapy has been proven to be a safe and effective technique for treating obstructive airway lesions. However, unlike laser therapy, recanalization does not occur instantly and tends to have a more delayed effect [4].
Complications may arise after bronchoscopic interventions [5]. Cryotherapy causes necrotic tissue, and this necrotic tissue can obstruct the airways. If the airways are obstructed by this necrotic tissue, post-obstructive pneumonia can develop. In these cases, repeat bronchoscopy is recommended to remove the necrotic tissue. In our case, the patient developed a post-obstructive pneumonia shortly after rigid bronchoscopy with cryotherapy. This required immediate re-intervention to remove the obstructing necrotic tissue. After clearance of the airway obstruction, and in combination with antibiotic therapy, a swift clinical improvement was seen. Risk factors for airway obstruction by necrotic debris are not completely known. Cryoablation causes tissue destruction and necrosis through multiple mechanisms, one of which is freezing of extracellular fluid, causing water shifts and cell dehydration. Tissue destruction is dependent of the water content of the target tissue, tissue with high water content such as mucosa is more sensitive to necrosis [6]. The fact that our patient had an extensive amount of granulation tissue can be seen as a risk factor for a higher amount of necrotic debris. The fast development of post-obstructive pneumonia can possibly be explained by the presence of H. influenzae in this COPD patient.
Our case illustrates that granulation tissue caused by foreign body aspiration should be left untreated unless it causes significant airway obstruction. When bronchoscopic interventions are used, one should be aware of potential post-procedural complications which necessitate re-intervention.
Conclusion
Granulation tissue after foreign body aspiration should not always be removed; conservative management is often sufficient. However, when bronchial obstruction occurs, the granulation tissue should be removed. Interventional techniques such as cryotherapy or coagulation are effective. Cryoablation has no immediate effect, it causes tissue necrosis over 48–72 h. As a result, necrotic debris can cause bronchial obstruction with development of post-obstructive pneumonia. A follow-up bronchoscopy should always be performed. In case of pneumonia after cryoablation, a low threshold for repeat bronchoscopy is recommended.
REFERENCES
1.
Hewlett JC, Rickman OB, Lentz RJ, Prakash UB, Maldonado F. Foreign body aspiration in adult airways: Therapeutic approach. J Thorac Dis 2017;9(9):3398–409. [CrossRef]
[Pubmed]

2.
Aykun G, Köseoğlu Hİ. Rapid and intense onset of granulation tissue formation following walnut aspiration: A case report. BMC Pulm Med 2025;25(1):96. [CrossRef]
[Pubmed]
3.
Bajaj D, Sachdeva A, Deepak D. Foreign body aspiration. J Thorac Dis 2021;13(8):5159–75. [CrossRef]
[Pubmed]
4.
Hetzel M, Hetzel J, Schumann C, Marx N, Babiak A. Cryorecanalization: A new approach for the immediate management of acute airway obstruction. J Thorac Cardiovasc Surg 2004;127(5):1427–31. [CrossRef]
[Pubmed]
5.
Mitchell PD, Kennedy MP. Bronchoscopic management of malignant airway obstruction. Adv Ther 2014;31(5):512–38. [CrossRef]
[Pubmed]
6.
Katzman D, Argento A. Advances in endobronchial ablative therapies. Shanghai Chest 2021;5:23. [CrossRef]
SUPPORTING INFORMATION
Author Contributions
Lyndon Sprenghers - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Peter Driesen - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2026 Lyndon Sprenghers et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}