 |
Case Report
Profound necrotizing fasciitis of the neck and chest wall secondary to simple tooth extraction necessitating surgical tracheostomy and reconstruction
1 Consultant Oral and Maxillofacial Surgery/Head and Neck Surgeon, Royal Cornwall Hospital, Cornwall, UK
2 DCT 1 Oral and Maxillofacial Surgery, James Cook Hospital, Middlesbrough, UK
Address correspondence to:
Karim Kassam
Consultant Oral and Maxillofacial Surgery/Head and Neck Surgeon, James Cook Hospital, Middlesbrough,
UK
Message to Corresponding Author
Article ID: 101530Z01KK2026
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Kassam K, Galia R. Profound necrotizing fasciitis of the neck and chest wall secondary to simple tooth extraction necessitating surgical tracheostomy and reconstruction. Int J Case Rep Images 2026;17(1):12–17.ABSTRACT
Introduction: Cervical necrotizing fasciitis (CNF) is a rare, but serious condition that can develop as a result of an odontogenic infection spreading into the deep fascial planes of the neck. The infection is associated with significant morbidity and mortality due to septic shock and consequent multiple organ failure. Early diagnosis is of paramount importance with immediate surgical management and appropriate antimicrobial therapy being key in obtaining a good outcome. Patients require aggressive surgical resection necrotic tissues which can affect form and function in the head and neck. Surgeons dealing with cervical necrotizing fasciitis should be skilled in tracheostomy, have good knowledge of head and neck anatomy, able to deal with fasciitis around neck vessels, and the ability to reconstruction the neck as needed.
Case Report: A case of CNF affecting a 31-year-old male, who was treated with multiple rapid surgical debridements, intravenous antibiotics, and tracheostomy, is presented. Transfer to a neighboring unit was needed due to concern of potential spread to the mediastinum necessitating cardio-thoracic intervention. After further debridements, artificial skin grafting and reconstruction were carried, and the patient was successfully discharged from the hospital.
Conclusion: Cervical necrotizing fasciitis is a relatively uncommon, rapidly progressive, and often life-threatening soft tissue infection. Early diagnosis, aggressive antibiotic, and surgical treatment play a vital role in the management of the disease. In patients with resultant skin or soft tissue defects, advanced reconstructive techniques are needed to close resultant defects.
Keywords: Cervical, Fasciitis, Infection, Necrotizing, Odontogenic
Introduction
Globally, mortality for head and neck necrotizing fasciitis (NF) has been reported to be 13.36% which can rapidly increase to 41% with mediastinal involvement [1]. The mortality rate for head and neck NF overall in the UK reported cases appeared to be 18% [2]. At least 3 of these patients had a mediastinal extension which could contribute to a higher mortality rate [2]. The main origins of infections in the head and neck are either odontogenic or traumatic [2].
Cervical necrotizing fasciitis is a rare but severe complication of odontogenic infection [2],[3]. It has a mortality rate of 9.8% [3]. The infectious process is rapid, normally over a few days spreading along the periapical tooth tissue via the fascial planes which are not respected by the disease into the neck causing a secondary infection of the overlying and underlying skin, soft tissue, and muscle. The infection often involves a mixture of gram positive bacteria such as streptococcus species and staphylococcus species. Patients may appear acutely unwell, or have a recent history of dental or maxillofacial trauma or long standing dental neglect. Clinical examination often finds patient septic with signs of cyanosis of the skin and soft tissue of the neck with mottling, cellulitis, necrosis, and tension. Crepitus is often felt due to the presence of gas forming organisms with severe forms of CNF extending the anterior chest wall as with our case, mediastinum, and potentially the upper abdominal region, which is life-threatening [4]. Risk factors include poor immune function such as from diabetes, cancer, obesity, alcoholism, intravenous drug use, and peripheral artery disease. The aim of this work is to highlight to dental practitioners and primary care medical practitioners that untreated dental infection might trigger necrotizing fasciitis in immunocompromised patients although patients do not always have an underlying medical condition [2], but also the emergency services. Quick referral to specialist services is essential to commence early management and improve patient outcomes.
Case Report
A 31-year-old male presented in the Emergency Department with painful left submandibular swelling and dysphagia for four days. He was prescribed Metronidazole by his dentist. His medical history included well controlled asthma, a brain aneurysm surgically treated in 2015 with complication of loss of vision in right eye. He had a history of alcohol excess 30 units/day. Significant initial blood abnormalities were as follows:
- C-reactive protein—444 mg/L (normal 0–10 mg/L)
- Potassium—3.1 mmol/L (normal 3.5–5.3 mmol/L)
- Creatinine—235 umol/L (normal 49–90 umol/L)
- eGFR—mL/min 31 (normal >90 mL/min)
- ALT-558 U/L (normal 10–130 U/L)
- Lactate of 2.7 mmol/L (normal 0.5–2.2 mmol/L)
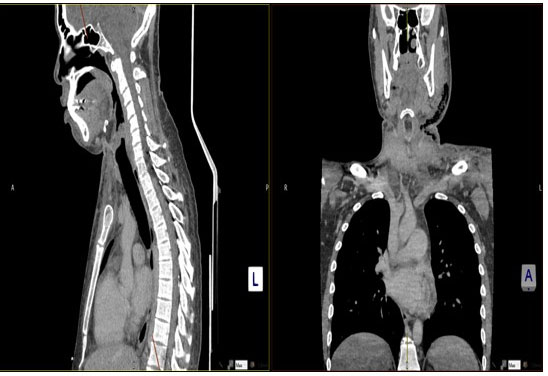
Clinical examination revealed diffuse left submandibular swelling extending toward neck with the mandibular border impalpable. The patient complained of pain. There were signs of cyanosis of the skin and soft tissue of the neck with mottling, cellulitis, necrosis, and tension. Crepitus was felt down to the clavicle. Intravenous antibiotics and fluids were administered. Orthopantogram radiograph suggested the suspected source of infection to be Lower Left Second Molar (Figure 1). His initial computed tomography (CT) of neck presented extensive subcutaneous gas and inflammatory change within the left neck arising from a dental infection extending within soft tissues into the lower left neck along with a small ill-defined subcutaneous collection lateral to the anterior left mandible (Figure 2). The most inferior locule of gas is seen approximately 1.4 cm above the left clavicle (Figure 3). Provisional diagnosis was Ludwig’s angina with a differential diagnosis of necrotizing fasciitis (NF) intravenous antibiotics were commenced as per the local microbiology guidelines for NF: flucloxacillin (2 g 4-hourly), metronizadole (500 mg 8-hourly), benzylpenicillin (2.4 g 6-hourly), and gentamicin (320 mg 24-hourly). Urgent incision and drainage with extraction of Lower Left Second Molar was arranged under general anesthesia along with surgical debridement (Figure 4). Four further surgical debridements in 1 week were subsequently required to arrest the progress of the disease (Figure 5). Post each debridement, betadine soaked gauze was placed in the neck secured with nonresorbable sutures (Figure 6). Tracheostomy was also done to maintain the airway as it was progressing towards the trachea and mediastinum. Pus was seen draining in the left neck (Figure 7). Post the fourth debridement, the area of necrosis had now spread over the anterior chest wall and below the clavicle (Figure 8). No end point was felt over the anterior chest wall and there was a concern of mediastinum breach and mediastinitis. At this point he was becoming septic. He was transferred to Plymouth University hospital at Day 9 from the Royal Cornwall for further management in case cardiothoracic surgical intervention was needed which was not available at our hospital. After further debridements, the patient was clinically stable and physiologically improving with down trending inflammatory markers and up trending albumin levels, making it appropriate for consideration of reconstruction. He needed staged reconstruction of left and anterior neck defect involving the skin and platysma down to deeper neuromuscular plane and muscle bellies.
Under the plastic surgery team further debridement was performed using the Versajet Hydrotechnique (Versajet 2 Hydrosurgery system) on the left side of the neck. The anterior neck that included a persistent tracheostomy stoma was reconstructed with rhomboid skin flap based inferiorly from the chest to achieve closure (Figure 9). A 15 × 10 cm granulating, clean, left neck wound (Figure 9), extending obliquely from the infra-auricular area down to the midline and base of the neck was inset with Integra (Integra LifeSciences) which is a synthetic acellular dermal regeneration template that provides a base for revascularization and neodermal formation. Integra is composed of a bilaminate membrane consisting of a bovine collagen based dermal analogue of glycosaminoglycans and chondroitin-6-sulfate, and a temporary epidermal substitute layer of silicone. This was secured with staples and a vacuum dressing with a silver based net gauze dressing underlying the vacuum dressing. The Integra product was fenestrated to minimize the risk of seroma. The patient was followed in the plastic dressing clinic for vacuum dressing changes, to ensure the Integra was adherent, and to monitor for seromas. This period was uneventful. Thirty days later a health bed was seen in order to graft the area (Figure 10). A split thickness skin graft from the thigh was harvested using a seven-thousandths of an inch setting. And placed onto the neck. The skin graft was secured with a silver-based dressing, sponge, and vacuum pump. The patient was followed up in the plastic dressing clinic for a skin graft check and was discharged a month later due to relocation to Australia. The skin graft was deemed to have a 98% take and was healthy (Figure 11). Advice was given regarding dressings. Subsequent telemedicine photographic updates demonstrated a well-healed and mature skin graft with good neck soft tissue pliability.










Discussion
Clinical features of NF involve early, intermediate, and late. Early features include tenderness to palpation (beyond apparent area of skin involvement), erythema, pain and calor (warmth), Intermediate features are blister or bull formation. Late features are crepitus of the skin, skin anesthesia and skin necrosis with dusky discoloration [5]. Diagnosis is made on clinical history, biochemical markers, and imaging together and not on their own. White blood cells and C-reactive protein (CRP) were not thought to be reliable indicators in a recent case series and review [4] although in our case the CRP was raised at 444 mg/L. Computed tomography scans remain the most popular imaging in these cases as expected and vary from soft tissue edema and inflammation, loss of clarity of the fat planes and gas locules or fluid collection [6],[7]. The presence of gas locules is the main predictor of NF [2] (Video 1, Video 2, Video 3).
Infection of second and third molars of the mandible are the most frequent etiologies of odontogenic cervical necrotising fasciitis. These teeth are deep into the mylohyoid insertion over the lingual side of the mandible. If untreated, infection that originates from these teeth can easily extend to the submandibular, and subsequently disseminated into surrounding spaces, including sublingual, submental, and parapharyngeal spaces. Ultimately infection can reaches the skull base, or caudally into the mediastinum and thoracic cavity. NF begins with progressive liquefaction of subcutaneous fat and connective tissue which is mediated by the collagenase and hyaluronidase produced by group A streptococci. This results in the separation of skin from the underlying soft tissue producing brownish edematous fluid, which is pathognomonic “dishwater pus.” It is followed by the disintegration of fascial planes, venous thrombosis, and inflammatory cell infiltration. This results in the spread of infection to deep cervical spaces with vascular compromise because of endarteritis obliterans of nutrient vessels. Widespread vascular compromise leads to skin necrosis and gangrene formation. The antibiotic therapy given intravenously, in the first instance is broad-spectrum, which is then modulated and customized as microbiology results are received after debridements.
Access video on other devices
Access video on other devices
Conclusion
Necrotizing fasciitis of the head and neck is a rare yet critical disease entity. The report highlights the importance of recognizing this severe infection in primary settings such as dental and medical practice where they first may attend or the emergency services. Early diagnosis and treatment is key to survival. Intensive medical and surgical care are crucial for treatment. A high index of suspicion is warranted for patients with diabetes or those taking immunosuppressive medications. Multiple surgical procedures are necessary and can result in massive defects. Even in severe cases, survival is likely when an aggressive treatment strategy is employed although the mortality rates are high. The treating physician should secure the airway if needed, aggressively debride repeatedly as antibiotics alone will not cure this disease and proceed with reconstruction after the infection is cleared.
REFERENCES
1.
Gunaratne DA, Tseros EA, Hasan Z, Kudpaje AS, Suruliraj A, Smith MC, et al. Cervical necrotizing fasciitis: Systematic review and analysis of 1235 reported cases from the literature. Head Neck 2018;40(9):2094–102. [CrossRef]
[Pubmed]

2.
Nazir H, Chieng CY, Rogers S, Nekrasisus R, Dodd M, Shah N. Outcomes of necrotizing fasciitis in the head and neck region in the United Kingdom – A case series and literature review. Advances in Oral and Maxillofacial Surgery 2022;6:100254.
3.
Gore MR. Odontogenic necrotizing fasciitis: A systematic review of the literature. BMC Ear Nose Throat Disord 2018;18:14. [CrossRef]
[Pubmed]
4.
Reed JM, Anand VK. Odontogenic cervical necrotizing fasciitis with intrathoracic extension. Otolaryngol Head Neck Surg 1992;107(4):596–600. [CrossRef]
[Pubmed]
5.
Wang YS, Wong CH, Tay YK. Staging of necrotizing fasciitis based on the evolving cutaneous features. Int J Dermatol 2007;46(10):1036–41. [CrossRef]
[Pubmed]
6.
Farrier JN, Kittur MA, Sugar AW. Necrotising fasciitis of the submandibular region; A complication of odontogenic origin. Br Dent J 2007;202(10):607–9. [CrossRef]
[Pubmed]
7.
Darat HN, Kanodia AK, Yong A, Ram B. A rare case of non-clostridial infection in a non-diabetic patient. BMJ Case Rep 2020;13(1):e233467. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Acknowledgments
Mr. Alexander Armstrong, Consultant Plastic Surgeon, University Hospitals Plymouth.
Author ContributionsKarim Kassam - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Roshni Galia - Acquisition of data, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2026 Karim Kassam et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}