 |
Case Series
Iniencephaly: Prenatal diagnosis and management—Case report
1 Department of Obstetrics and Gynecology, Yekatit 12 Hospital Medical College, Addis Ababa, Ethiopia
Address correspondence to:
Tewodros Getahun Asfaw
Department of Obstetrics and Gynecology, Yekatit 12 Hospital Medical College, Addis Ababa,
Ethiopia
Message to Corresponding Author
Article ID: 101527Z01TA2025
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Asfaw TG, Dina BK, Wube YT. Iniencephaly: Prenatal diagnosis and management—Case report. Int J Case Rep Images 2025;16(2):79–83.ABSTRACT
Introduction: Iniencephaly is a rare and complex neural tube defect characterized by significant deformities in the cervical and thoracic spine, resulting in an extremely retroflexed head. Although environmental and genetic factors have been proposed as potential causes, the precise etiology and pathogenesis are not well understood. Prenatal diagnosis of iniencephaly through ultrasound is rare, but it can often be confirmed with a second-trimester ultrasound. Due to its almost universally fatal prognosis, pregnancy termination is often considered when this condition is diagnosed before the fetus reaches age of viability.
Case Report: We present two cases of prenatal iniencephaly diagnosis, which, to the best of our knowledge, represent the second documented instances of iniencephaly diagnosis in Ethiopia, where the condition was first identified during Fetal Anatomic Scanning.
Conclusion: Iniencephaly is a severe and devastating condition that demands early prenatal diagnosis and counseling. Timely anatomic scanning enables an accurate diagnosis and provides families with the essential information to make informed decisions. In this case, early diagnosis facilitated appropriate management, including pregnancy termination, and was followed by a smooth post-expulsion period.
Keywords: Ethiopia, Iniencephaly, Neural tube defect, Prenatal diagnosis
Introduction
Iniencephaly is a rare and complex neural tube defect characterized by significant deformities in the cervical and thoracic spine, resulting in an extremely retroflexed head. The condition also causes the absence of a visible neck, with the skin extending continuously from the back of the scalp to the skin on the back, and from the face to the chest [1]. The neck is absent due to the partial or complete absence of the occipital squama, along with defects, abnormal fusion, and splitting of the cervical and thoracic vertebrae, as well as issues with the closure of the vertebral arches. The lordosis in the cervicothoracic region causes the face to tilt upwards (stargazing head), while the trunk is typically deformed and shortened [2],[3],[4].
CASE SERIES
Case 1
This is a 24-year-old primigravid woman who was referred from a nearby health center at a gestational age of 23 weeks with a suspicion of nuchal edema for further investigation at Abebech Gobena Referral Hospital in Addis Ababa, Ethiopia. All her baseline investigations were normal, and she had no known medical conditions or drug use.
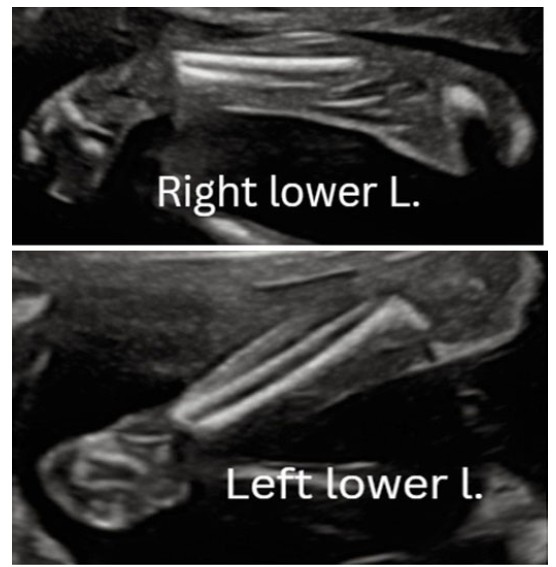
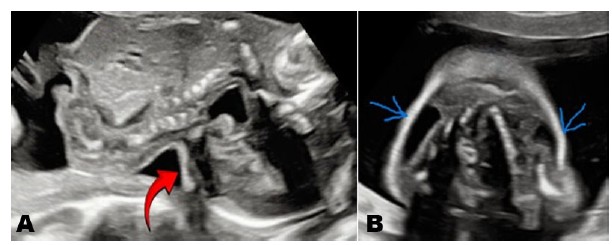
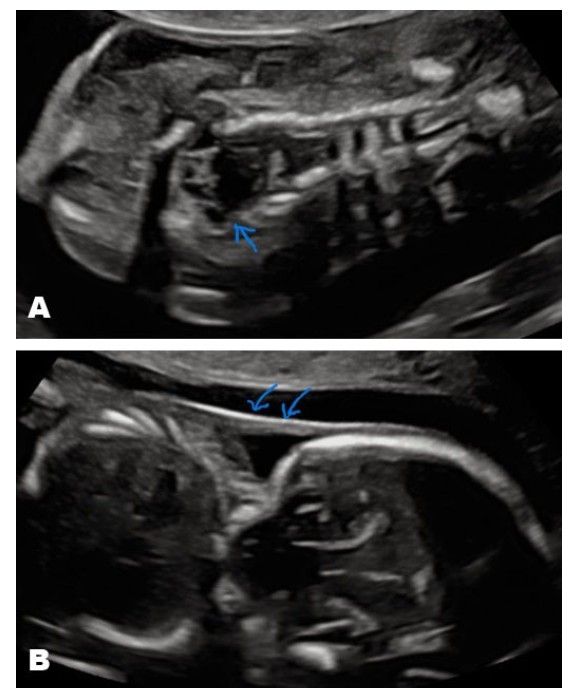
Upon fetal anatomic scanning at the Maternal Fetal Medicine unit, a singleton viable intrauterine pregnancy was identified with a fixed, hyperextended neck and a continuous scalp extending to the skin of the thorax, as shown in Figure 1A, Figure 1B, Figure 1C. Additionally, neck edema likely secondary to lymphatic obstruction was observed (as shown in Figure 2). Unilateral clubfoot was observed on the right lower limb, while the left lower limb appeared normal (as shown in Figure 3, right and left lower limbs, respectively).
The final diagnosis of iniencephaly was made, and the prognosis was discussed with the family. They opted pregnancy termination. Mifepristone and misoprostol were administered, and the mother expelled a 500 g male fresh stillborn (Figure 4). The post-expulsion period was uneventful. The mother was counseled on the risk of recurrence and advised to seek early preconceptional care. She was then discharged. A postmortem X-ray was not performed due to the unavailability of X-ray services at the hospital.
Case 2
A 24-year-old primigravid woman, with an unknown last menstrual period, had her gestational age calculated at eight weeks via crown-rump length (CRL). She was first referred to Abebech Gobena Referral Hospital at 8 weeks and 4 days, where a vanishing twin was noted. Her baseline investigations were uneventful. She continued follow-up care at the same hospital and was subsequently referred to the Maternal Fetal Medicine unit for a fetal anatomic scan at 20 weeks gestational age.
During the anatomic scan, the vanishing co-twin was not visible, and a singleton viable intrauterine fetus was identified. The fetus exhibited a fixed hyperextended neck with a stargazing facial appearance, along with a continuous scalp extending to the skin of the back. The axial view of the neck revealed bilateral neck edema, likely caused by lymphatic obstruction (Figure 5).
Additionally, the spine appeared unusually short with vertebral splaying, particularly in the cervicothoracic region, although it was covered by overlying skin as shown in Figure 6A and Figure 6B respectively.
The final diagnosis was iniencephaly. After counseling on the prognosis, the mother opted for pregnancy termination. Following the initiation of mifepristone and misoprostol, she delivered a 450 g freshly died male stillborn (Figure 7). The post-expulsion period was smooth, with no complications. The autopsy was not performed because the family chose not to pursue further investigation of the stillborn baby due to cultural and religious beliefs.




Discussion
Iniencephaly is an abnormality in cervical vertebrae associated with cervicothoracic spinal retroflexion and neural tube defect [5]. The incidence of iniencephaly is approximately 1 in 100,000 to 1 in 1000 births, with a notable female predominance (90%) observed [6],[7],[8],[9],[10]. This contrasts with our case, as both of the stillborns were male.
Two types of iniencephaly are recognized based on the presence or absence of encephalocele: iniencephalus apertus, which involves the presence of encephalocele, and iniencephalus clausus, where encephalocele is absent [11],[12]. Iniencephaly can be diagnosed prenatally through ultrasound starting in the early second trimester. The diagnosis is typically straightforward due to the characteristic star-gazing appearance of the fetus [6].
The sonographic features of iniencephaly include: (1) A defect in the occipital bone, resulting in an enlarged foramen magnum; (2) Partial or complete absence of the cervical and thoracic vertebrae, with irregular fusion of the remaining vertebrae and incomplete closure of the vertebral arches and/or bodies; (3) A significantly shortened spinal column due to marked lordosis and hyperextension of the malformed cervicothoracic spine; and (4) An upward-turned face, with the mandible’s skin directly connected to the chest, caused by the absence of a neck [7],[13],[14]. Polyhydramnios is commonly associated with iniencephaly due to impaired fetal swallowing [10].
Iniencephaly is thought to occur due to the arrest of the embryo in physiological retroflexion during the third week of gestation or from a failure in the normal forward bending process that typically happens in the fourth week. This results in a fixed retroflexion of the head and severe lordosis of the cervicothoracic spine [15]. While there is no definitive evidence for the etiologic factors, it appears that nutritional, environmental, and genetic factors have been suggested as potential causes [16],[17].
It has been observed that in geographic areas with a higher prevalence of anencephaly, there is also an increased prevalence of iniencephaly [5]. The majority of cases of iniencephaly are sporadic and likely related to polygenic inheritance [18]. However, it has also been reported as a result of congenital syphilis, maternal diabetes, and exposure to teratogenic substances such as triparanol, streptonigrin, and vincaleukoblastine [18]. Additionally, chromosomal abnormalities, including trisomy 18, trisomy 13, and monosomy X, have also been associated with this anomaly [19].
Although most patients are either stillborn or pass away within a few hours after birth, only a few survivors have been documented in the literature to date. However, the prognosis for infants with iniencephaly remains extremely poor [16],[17],[20]. Due to its nearly universally fatal prognosis, termination of pregnancy is common when this condition is diagnosed before the fetus reaches the age of viability [3],[18].
Given that iniencephaly has a recurrence rate of 1% to 5%, the Centers for Disease Control and Prevention (CDC), Institute of Medicine, all recommend that women who have previously had a pregnancy affected by neural tube defects take 4000 mcg of folic acid daily, starting at least one month before pregnancy and continuing through the first three months of pregnancy [17],[18],[21].
Conclusion
Iniencephaly is a severe and devastating condition that demands early prenatal diagnosis and counseling. Timely anatomic scanning enables an accurate diagnosis and provides families with the essential information to make informed decisions. In this case, early diagnosis facilitated appropriate management, including pregnancy termination, and was followed by a smooth post-expulsion period.
REFERENCES
1.
Holmes LB, Toufaily MH, Westgate MN. Iniencephaly. Birth Defects Res 2018;110(2):128–33. [CrossRef]
[Pubmed]

2.
Lemire RJ, Beckwith JB, Shepard TH. Iniencephaly and anencephaly with spinal retroflexion. A comparative study of eight human specimens. Teratology 1972;6(1):27–36. [CrossRef]
[Pubmed]
3.
Joó JG, Beke A, Papp C, Szigeti Z, Csaba A, Papp Z. Major diagnostic and pathological features of iniencephaly based on twenty-four cases. Fetal Diagn Ther 2008;24(1):1–6. [CrossRef]
[Pubmed]
4.
Csabay L, Szabó I, Papp C, Tóth-Pál E, Papp Z. Central nervous system anomalies. Ann N Y Acad Sci 1998;847:21–45. [CrossRef]
[Pubmed]
5.
Danzer E, Rintoul NE, Adzick NS. Pathophysiology of neural tube defects. 5th ed. Fetal and neonatal physiology, 2-volume set. Elsevier Inc.; 2017. p. 1712–23.
6.
Pungavkar SA, Sainani NI, Karnik AS, Mohanty PH, Lawande MA, Patkar DP, et al. Antenatal diagnosis of iniencephaly: Sonographic and MR correlation: A case report. Korean J Radiol 2007;8(4):351–5. [CrossRef]
[Pubmed]
7.
Chen CP. Prenatal diagnosis of iniencephaly. Taiwan J Obstet Gynecol 2007;46(3):199–208. [CrossRef]
[Pubmed]
8.
Alvis-Miranda HR, Bula-Anichiarico DA, Calderón-Miranda WG, Moscote-Salazar LR. Iniencephaly: Case report. J Pediatr Neurosci 2015;10(2):181–4. [CrossRef]
[Pubmed]
9.
Subzposh NA, Ekramullah, Haque F, Sabat S. Iniencephaly. Indian J Pediatr 2003;70(4):355–6. [CrossRef]
[Pubmed]
10.
Scherrer CC, Hammer F, Schinzel A, Briner J. Brain stem and cervical cord dysraphic lesions in iniencephaly. Pediatr Pathol 1992;12(3):469–76. [CrossRef]
[Pubmed]
11.
Esin S, Yirci B, Yalvaç S, Kandemir Ö. Prenatal diagnosis of iniencephaly: Clues and pitfalls. Gynecol Obstet Reprod Med 2012;18(3):148–50.
12.
Lewis H. Iniencephalus. Am J Obstet Gynecol 1897;35:11.
13.
Persutte WH, Lenke RR, Kurczynski TW, Woldenberg LEE. Case reports prenatal ultrasonographic of iniencephaly aperta diagnosis. J Diagnostic Med Sonogr 1991;208–12.
14.
Mórocz I, Szeifert GT, Molnár P, Tóth Z, Csécsei K, Papp Z. Prenatal diagnosis and pathoanatomy of iniencephaly. Clin Genet 1986;30(2):81–6. [CrossRef]
[Pubmed]
15.
Chavan SB. Iniencephaly : A rare anomaly. Natl J Clin Anat 2019;8(1):43–6.
16.
Bakhti S, Tighilt N, Khoudir W, Djennas M. Iniencephaly with long survival: A rare condition. Iran J Neurosurg 2016;2(3):19–21.
17.
Arega BN, Endalew SD, Hailu DM. A rare case of fetal neural tube defect; Iniencephaly clausus. AJP Rep 2024;14(4):e281–3. [CrossRef]
[Pubmed]
18.
Sahid S, Sepulveda W, Dezerega V, Gutierrez J, Rodriguez L, Corral E. Iniencephaly: Prenatal diagnosis and management. Prenat Diagn 2000;20(3):202–5.
[Pubmed]
19.
Kulkarni PR, Rao RV, Alur MB, Joshi SK. Iniencephaly clausus: A case report with review of literature. J Pediatr Neurosci 2011;6(2):121–3. [CrossRef]
[Pubmed]
20.
Agostini L, Massimi L, Tamburrini G, Frassanito P, Bianchi F. Iniencephaly and long-term survival: A possible association—Case report and review of the literature. Childs Nerv Syst 2023;39(8):2027–35. [CrossRef]
[Pubmed]
21.
CDC, Institute of Medicine and USPSTF. Folic Acid Recommendations 2023;3–6.
SUPPORTING INFORMATION
Acknowledgments
We would like to acknowledge and express our gratitude to all the management teams who were involved in overseeing the care of these mothers during their time at our hospital. Their dedication and teamwork played a vital role in ensuring the best possible care and support. Additionally, we would like to thank the mothers for their willingness to be presented as cases, their cooperation in providing the necessary data, and their commitment to attending regular follow-up appointments. The author used generative AI technology, specifically canva.com/ photo-editor/were used for editing figures and images. All content, including text and images, was reviewed and verified by the author to ensure factual accuracy and originality. The author takes full responsibility for the final manuscript.
Author ContributionsTewodros Getahun Asfaw - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Birhanu Kebede Dina - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Yared Tesfaye Wube - Conception of the work, Design of the work, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2025 Tewodros Getahun Asfaw et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}