 |
Case Report
Primary pulmonary meningioma or large meningothelial-like nodule? A clinicopathological dilemma
1 St. Joseph’s Healthcare Hamilton Charlton Campus, Hamilton, Ontario, Canada
2 Division of Thoracic Surgery, Department of Surgery, McMaster University, Hamilton, Ontario, Canada
3 Department of Medical Imaging, McMaster University, Hamilton, Ontario, Canada
4 Department of Pathology and Molecular Medicine, McMaster University, Hamilton, Ontario, Canada
Address correspondence to:
Moaz Alowami
St. Joseph’s Healthcare Hamilton Charlton Campus, Hamilton, Ontario
Canada
Message to Corresponding Author
Article ID: 101526Z01MA2025
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Alowami M, Agzarian J, Haider E, Bonert M, Naqvi A. Primary pulmonary meningioma or large meningothelial-like nodule? A clinicopathological dilemma. Int J Case Rep Images 2025;16(2):73–78.ABSTRACT
Introduction: Primary pulmonary meningiomas (PPMs) are rare ectopic tumors that potentially arise from displaced embryonic arachnoid cells that are isolated outside the dura mater. Its presence outside of the central nervous system poses inherent challenges. We report a case of a primary pulmonary meningioma discovered after a 12-year follow-up for a presumed benign lung lesion.
Case Report: A 47-year-old male with a 17-year history of severe, undiagnosed right-sided subxiphoid and periumbilical pain was monitored for a right middle lobe lung mass that grew from 2.2 cm to 3.4 cm over 12 years. Initially, the transthoracic needle biopsy suggested a solitary fibrous tumor. Video-assisted thoracoscopic wedge resection with concomitant biopsy displayed the characteristic histomorphology, including whorling and psammomatous calcification. Positive immunohistochemical staining for epithelial membrane antigen (EMA) and progesterone receptor (PR) supported the diagnosis of clinically confirmed PPM.
Conclusion: This interesting case illustrates that primary pulmonary meningiomas can mimic other tumors and may be associated with atypical symptoms like chronic pain. In this 12-year monitored case, surgery relieved the patient’s debilitating 17-year-long chronic pain. Additionally, a novel nomenclature system was developed to help distinguish between PPMs and large meningothelial-like nodules.
Keywords: Pathology, Pulmonary meningioma, Pulmonary meningothelial-like nodules
Introduction
Ectopic primary meningiomas are rare neoplasms typically diagnosed in the head and neck region. Primary pulmonary meningiomas are specifically very rare, with few reported cases in the literature. In contrast to available published literature, this case reports a longitudinal monitoring period of 12 years and a definitive management via video-assisted thoracoscopic wedge resection of the right middle lobe. This case reports a unique insidious clinical presentation with a longstanding, undiagnosed right-sided subxiphoid, and periumbilical pain.
Primary pulmonary meningioma (PPM) is a rare ectopic tumor that potentially arises from displaced embryonic arachnoid cells that are isolated outside the dura mater [1],[2],[3]. Primary pulmonary meningioma is a formidable diagnostic challenge. It manifests as an incidental asymptomatic solitary pulmonary nodule with an epidemiological propensity for middle-aged or older female adults [4]. Radiological modalities such as computed tomography (CT) and positron emission tomography (PET) present ambiguity when detecting PPMs [5]. This ambiguity results from radiological findings that are non-specific and mimic malignancy. Histopathological biopsy is warranted in these cases for granular confirmation. Histological hallmark features of PPM include cellular whorls, psammoma bodies, and positive immunohistochemical staining for EMA and SSTR2A [6]. The vast majority of PPMs are benign (WHO Grade I) and curative with complete surgical resection, leading to an excellent prognosis [7].
Ectopic primary meningiomas are rare neoplasms typically diagnosed in the head and neck region. Primary pulmonary meningiomas are specifically very rare, with few reported cases in the literature. In contrast to available published literature, this case reports a longitudinal monitoring period of 12 years and a definitive management via video-assisted thoracoscopic wedge resection of the right middle lobe. This case reports a unique insidious clinical presentation with a longstanding, undiagnosed right-sided subxiphoid, and periumbilical pain.
Primary pulmonary meningioma (PPM) is a rare ectopic tumor that potentially arises from displaced embryonic arachnoid cells that are isolated outside the dura mater [1],[2],[3]. Primary pulmonary meningioma is a formidable diagnostic challenge. It manifests as an incidental asymptomatic solitary pulmonary nodule with an epidemiological propensity for middle-aged or older female adults [4]. Radiological modalities such as computed tomography (CT) and positron emission tomography (PET) present ambiguity when detecting PPMs [5]. This ambiguity results from radiological findings that are non-specific and mimic malignancy. Histopathological biopsy is warranted in these cases for granular confirmation. Histological hallmark features of PPM include cellular whorls, psammoma bodies, and positive immunohistochemical staining for EMA and SSTR2A [6]. The vast majority of PPMs are benign (WHO Grade I) and curative with complete surgical resection, leading to an excellent prognosis [7].
Case Report
A 47-year-old male presented with a longstanding history of right-sided subxiphoid and periumbilical pain, who had been monitored for approximately 12 years for a benign lung tumor in the right middle lobe. In 2006, a computed tomography (CT) scan of the chest showed a 2.2 cm mass in the medial segment of the right middle lobe. His past medical history is significant for a remote motor vehicle accident as a child, where he suffered substantial bruising of the ribs as well as a pulmonary contusion. He frequently suffers from migraines and has a longstanding history of chronic right upper quadrant abdominal and subxiphoid pain for at least the last 17 years. He had undergone several investigations for this prolonged radiating pain, including CT scans, abdominal ultrasound, and a hepatobiliary (HIDA) scan. All tests were inconclusive and unable to diagnose the origin of his pain. The patient is currently not working secondary to functional limitations associated with his chronic pain. He has smoked 10 cigarettes per day for the last 25 years. His social history also supplemented non-quantifiable asbestos exposure in the past.
The debilitating radiating pain initiated a follow-up CT scan performed in 2017, which showed that the lesion had increased in size to 3.4 cm. Radiographic characterization demonstrated a round, solid, well-circumscribed mass with smooth margins that abutted the pleural surfaces of the diaphragm as well as the anterior aspect of the lung (Figure 1). The mass was homogeneous without areas of calcification or fatty attenuation. Atelectasis of the lingula with scattered bilateral calcified granulomas was also present. Radiologically, the lesion was suspected to be of pleural or pulmonary origin. In conjunction with the interval growth of the lesion, a biopsy was recommended. A transthoracic needle biopsy of this right middle lobe lung mass was performed at an outside facility. The biopsy displayed spindle cells with focal staining for CD34. The findings were felt to be consistent with solitary fibrous tumor, and the patient was referred for thoracic surgery consultation. According to the documented growth and biopsy results, the management algorithm pivoted to a surgical resection using a sublobar technique. The patient was informed that surgical treatment would not be expected to provide any therapeutic benefit to his chronic pain.
The patient underwent a video-assisted thoracoscopic wedge resection of the right middle lobe. Histological margins were grossly clear, and there was no evidence of any pleural seeding/metastasis and no diaphragmatic involvement/invasion. The tumor appeared to arise from the anterior aspect of the medial segment of the right middle lobe. Surgery was uncomplicated. The patient was discharged on the third postoperative day. Postoperative resection of the tumor gradually reduced the severity and frequency of the pain. A magnetic resonance imaging (MRI) of the brain and spine showed no abnormality or tumor.
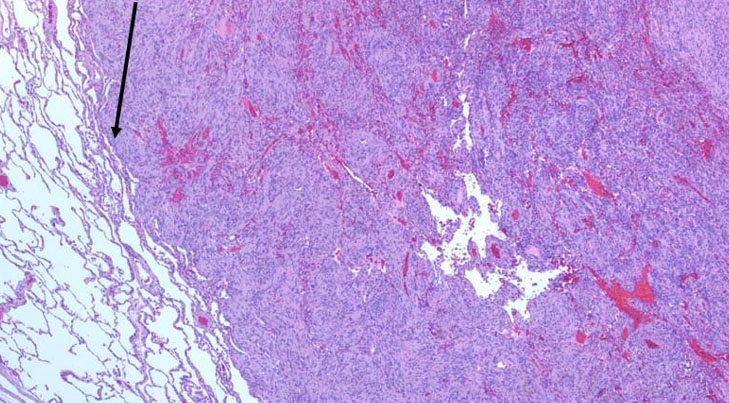
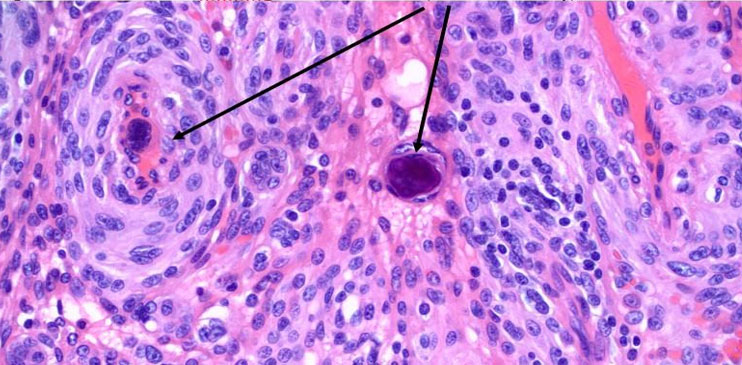
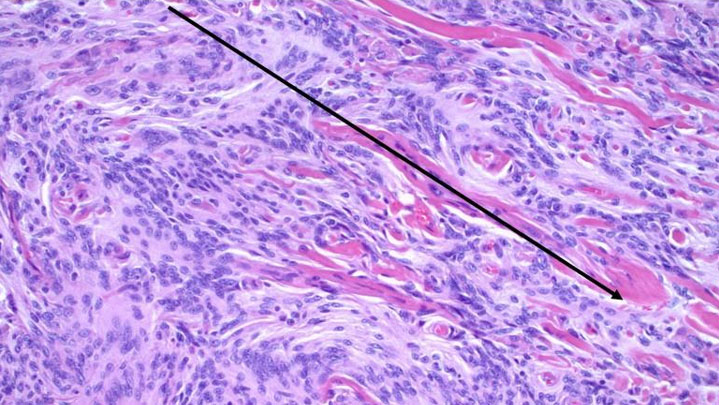
The wedge resection specimen demonstrated a 3.4 × .3.0 cm subpleural mass involving the pleura. The lesion was homogenous, gray-white, and did not show any necrosis or hemorrhage (Figure 2). Hematoxylin & Eosin (H&E) stained sections of the mass showed a spindle cell lesion with characteristic whorling (Figure 3). The nuclei showed mild atypia with the absence of necrosis and mitosis. The cells had indistinct cell borders. A focal area of thick collagen deposition was seen (Figure 4). The tumor showed a mild sprinkling of lymphocytes. Focal hemorrhage and hemosiderin-containing macrophages were present. Several foci of concentric calcification resembling psammoma bodies were present.
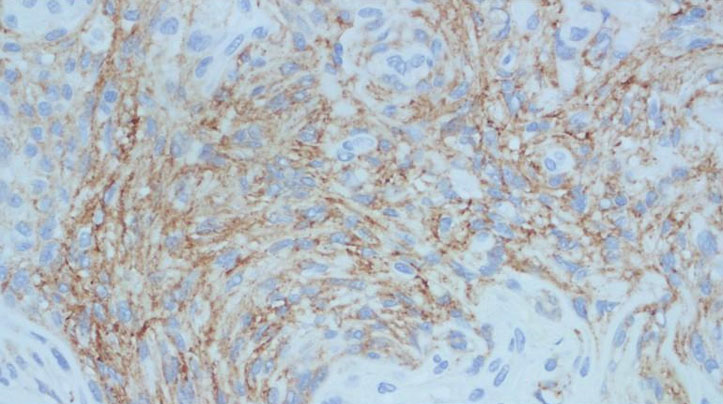
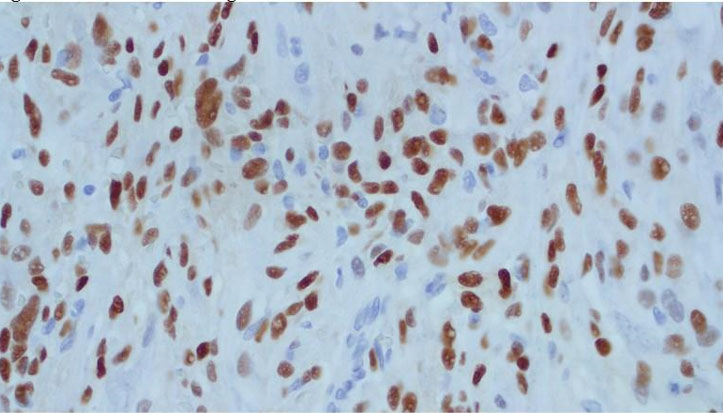
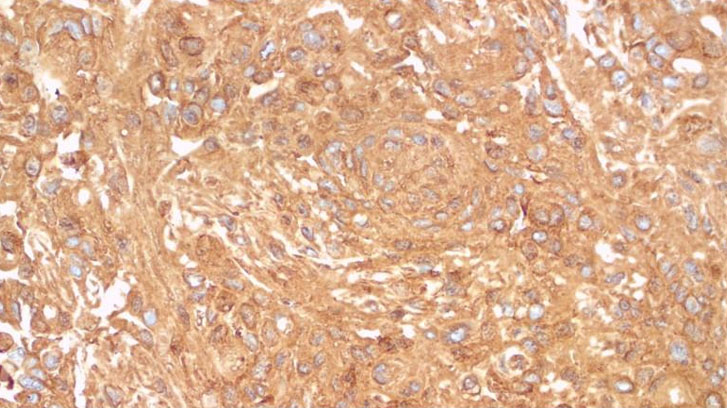
On immunohistochemical analysis, the tumor cells stained positive with EMA, PR, Vimentin, SMA, CD31, CD56 (focally), S100 (focally), ER (focally), Fascin (focally), D2-40, CKIT (focally), CD99, and negatively stained for Desmin, CD34, Calretinin, WT1, AE1/AE3, HMB45, CD68, MelanA, CAM5.2, FVIII, DOG1, Caldesmon, CD23, CD138, HHV8, Langerin, CD21 and CK5/6. BCL-2 showed focal positive staining in the background lymphocytes (Figure 5, Figure 6, Figure 7). The morphology and immunohistochemical staining profile were consistent with a meningioma. Upon close follow-up, the patient is free of any residual disease five years after surgery.

Discussion
Extracranial meningiomas (ECM) are rare tumors. Most of the ECM are anatomically located in the sinonasal tract, ear, temporal bone, and scalp. Primary pulmonary meningiomas (PPM) are extremely rare, with only about 40 cases reported in the literature. Most of these lesions are benign [1]. Incarbone et al. found that 8% of primary pulmonary meningioma cases had malignant features. Pathological features that would elucidate suspicion of potential malignancy include nuclear pleomorphism, increased mitotic figures, and invasion into surrounding tissue [2]. However, this case demonstrates a well-circumscribed homogenous lesion. Additionally, no increased mitotic figures and significant nuclear pleomorphism were noted.
The cell of origin of PPM is not specific, and there are several theories about its origin, including development from arachnoid lung cells and meningothelial-like nodules [3]. Evidence-based literature suggests that pulmonary meningothelial nodules typically present clinically as an incidental finding [7],[8].
Masago et al. suggested that PPM are giant forms of pulmonary meningothelial-like nodules (PMLN) [9]. Interestingly, Niho et al. conducted various immunohistochemical analyses suggesting that PMLNs are reactive rather than neoplastic [10]. In their extensive review, Mukhopadhyay et al. found that PMLN ranged in size from a few cells up to 4 mm. The authors concluded that multiple PMLNs were present in 41% of cases, but none were more than 4 mm in size [5]. Ionescu et al., using 20 polymorphic microsatellite markers, found that PPMs have specific molecular genetic events involving chromosomes 22q, 14q, and 1p, which were not seen in cases of PMLNs [6].
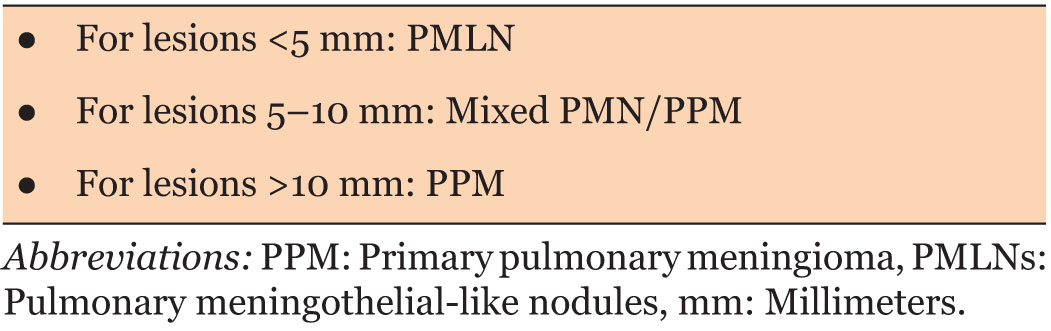
The differentiation of PMN from PMLN is based more on size characteristics than morphologic features. We propose that, in conjunction with molecular findings, a cut-off size of 1 cm be used to differentiate between the two entities. Accordingly, we propose a novel three-tiered nomenclature for classification and differentiation of PPM and PMLN (Table 1).
Notably, PPM is a diagnosis of exclusion. Two strict criteria must be met for a definitive diagnosis: (1) Histopathological confirmation of a meningioma within a resected pulmonary specimen, and (2) The comprehensive radiological exclusion of a primary meningioma within the intracranial or intraspinal compartments [7]. There are no characteristic radiological findings of PPM. They are usually well circumscribed with homogeneous or heterogeneous enhancement on contrast-enhanced CT scans [8]. Positron emission tomography/computed tomography (PET/CT) scanning with 18-fluoro-2-deoxy-D-glucose (FDG) is a standard tool for evaluating the metabolic activity of pulmonary nodules to assess the likelihood of malignancy. However, in the context of PPM, FDG-PET is highly unreliable [9]. Our case showed a well-circumscribed, slowly enlarging mass over 12 years with abutment of the pleural surface. Most PPMs are solitary benign lesions, best treated by surgical resection. Long-term follow-up of these patients demonstrates excellent prognosis with prolonged disease-free survival spanning many years. No established guidelines exist regarding the duration and modality of follow-up. In our case, after ruling out the presence of a primary cranial or spinal meningioma, pulmonary surveillance for 10 years using magnetic resonance imaging (MRI) of the chest was proposed. Magnetic resonance imaging provides the added benefit of decreasing radiation exposure (as compared to a CT scan), while allowing for careful size estimates and evaluation of radiographic features. Furthermore, several potential differential diagnoses must be considered when radio-pathologically investigating PPM. Metastatic meningioma, primary lung cancer, solitary fibrous tumor, and schwannoma must be carefully considered.
On gross examination, PPMs typically appear as well-circumscribed, unencapsulated, firm, solid nodules. A homogenous texture is found on the cut surface of PPMs. The color is variable, ranging from tan to white, greyish-white, and even yellow [9],[11]. Under the microscope, whorl formation and psammoma bodies are histopathological features of PPM. The characteristic epithelioid and spindle-shaped cells with eosinophilic cytoplasm often have indistinct or invisible cell borders. In PPM, the nuclei are oval and contain fine chromatin [9]. The pathognomonic feature is the arrangement of these cells into tight, concentric whorls, often resembling small eddies or onions [12]. The presence of psammoma bodies is a classic pathognomonic feature. Laminated, concentric microcalcifications characterize psammoma bodies [13]. Also evident are the presence of intranuclear pseudoinclusions, which are invaginations of the cytoplasm into the nucleus [9]. Immunohistochemical staining is a ubiquitous tool for confirming the meningothelial origins of the tumor. In chronological order of clinical association, indicative markers of PPM include epithelial membrane antigen (EMA), somatostatin receptor 2A (SSTR2A), vimentin, and progesterone receptor (PR) [7].
Complete surgical resection is the universally accepted standard of care for PPM. The most common procedure is a wedge resection. Wedge resection is a minimally invasive technique used for smaller, peripherally located tumors [7],[9]. Larger or more centrally located tumors may require more extensive surgeries, such as a lobectomy [7]. In rare circumstances, for high-risk patients with stable nodules, a conservative “watch-and-wait” approach with close surveillance may be considered instead of surgery [14]. Radiotherapy and chemotherapy are alternative therapeutic strategies in advanced or metastatic PPM [15]. The long-term prognosis for patients with PPM is almost entirely dependent on the tumor's WHO grade. WHO grade 1 is the benign manifestation of PPM, making this category the perfect candidate for complete surgical resection for an excellent prognosis [7]. WHO Grade II and III are high-grade variants that have a more aggressive course and are more likely to predispose to recurrence post-resection [7]. Primary pulmonary meningiomas have the potential to undergo malignant transformation, particularly when they recur [16],[17],[18],[19].
Conclusion
The unique presentation of this case highlights the necessity of diligent clinical monitoring driven by robust patient-centered care. Primary pulmonary meningioma is a rare benign tumor belonging to the family of ectopic meningiomas. Albeit PPM’s clinical significance is its capability to mimic more aggressive pathologies. The radiological ambiguity of a solitary pulmonary nodule with a potential high 18-fluoro-2-deoxy-D-glucose (FDG) avidity can pivot the diagnostic and therapeutic strategy. Lung-guided imaging confirmed by histopathological biopsy and diagnosis of exclusion via neuroimaging is the most sensible approach. Hallmark histological findings such as cellular whorls and psammoma bodies, in conjunction with a positive immunohistochemical staining profile, provide a definitive diagnosis. Dissemination of radio-pathological awareness of PPMs' clinical presentation can educate future clinicians on how to navigate the challenging nature of PPMs.
REFERENCES
1.
Ong K, Rajapaksha K, Ahmed A. P2.04-038 Primary pulmonary meningioma: Rare tumor with malignant potential. Journal of Thoracic Oncology 2017;12(1):S1020.

2.
Incarbone M, Ceresoli GL, Di Tommaso L, Cappuzzo F, Inzirillo F, Infante M, et al. Primary pulmonary meningioma: Report of a case and review of the literature. Lung Cancer 2008;62(3):401–7. [CrossRef]
[Pubmed]
3.
Iaconetta G, Santella A, Friscia M, Abbate V, Califano L. Extracranial primary and secondary meningiomas. Int J Oral Maxillofac Surg 2012;41(2):211–7. [CrossRef]
[Pubmed]
4.
Gürçay N, Öztürk A, Demirağ F, İncekara F. Primary pulmonary meningioma mimicking pulmonary metastasis: A rare case report. Turk Gogus Kalp Damar Cerrahisi Derg 2020;28(4):699–701. [CrossRef]
[Pubmed]
5.
Hong S, Jiang J, Zhou F, Liu J. Computed tomography findings of primary pulmonary meningioma: A case report. Medicine (Baltimore) 2018;97(2):e9651. [CrossRef]
[Pubmed]
6.
Yang B, Qiu J. Primary pulmonary meningioma with associated multiple micronodules: A case report and literature review. J Surg Case Rep 2023;2023(2):rjad034. [CrossRef]
[Pubmed]
7.
Mukhopadhyay S, El-Zammar OA, Katzenstein ALA. Pulmonary meningothelial-like nodules: New insights into a common but poorly understood entity. Am J Surg Pathol 2009;33(4):487–95. [CrossRef]
[Pubmed]
8.
Mizutani E, Tsuta K, Maeshima AM, Asamura H, Matsuno Y. Minute pulmonary meningothelial-like nodules: Clinicopathologic analysis of 121 patients. Hum Pathol 2009;40(5):678–82. [CrossRef]
[Pubmed]
9.
Masago K, Hosada W, Sasaki E, Murakami Y, Sugano M, Nagasaka T, et al. Is primary pulmonary meningioma a giant form of a meningothelial-like nodule? A case report and review of the literature. Case Rep Oncol 2012;5(2):471–8. [CrossRef]
[Pubmed]
10.
Niho S, Yokose T, Nishiwaki Y, Mukai K. Immunohistochemical and clonal analysis of minute pulmonary meningothelial-like nodules. Hum Pathol 1999;30(4):425–9. [CrossRef]
[Pubmed]
11.
Fujikawa R, Arai Y, Otsuki Y, Nakamura T. A case of a primary pulmonary meningioma mimicking a metastasis from a papillary thyroid carcinoma due to a size reduction after radioactive iodine therapy. Surg Case Rep 2020;6(1):57. [CrossRef]
[Pubmed]
12.
Liu Q, Luo S, Guo M. Primary pulmonary meningioma: A case report and literature review. Front Oncol 2025;15:1601698. [CrossRef]
[Pubmed]
13.
Pannu MK, Ehrsam JP, Schöb OM, Inci I. Primary pulmonary meningioma: A case report. J Surg Case Rep 2024;2024(6):rjae406. [CrossRef]
[Pubmed]
14.
Liu LD, Zhang KX, Zhang HN, Zheng YW, Xu HT. Primary pulmonary meningioma and minute pulmonary meningothelial-like nodules: Rare pulmonary nodular lesions requiring more awareness in clinical practice. World J Clin Cases 2024;12(11):1857–62. [CrossRef]
[Pubmed]
15.
Cheng J, Guo C. Primary pulmonary meningioma: A case report and literature review. J Cardiothorac Surg 2025;20(1):44. [CrossRef]
[Pubmed]
16.
Yu J, Deng J, Ren L, Hua L, Gong Y. Malignant transformation of meningiomas. J Cancer 2025;16(5):1684–93. [CrossRef]
[Pubmed]
17.
Ionescu DN, Sasatomi E, Aldeeb D, Omalu BI, Finkelstein SD, Swalsky PA, et al. Pulmonary meningothelial-like nodules: A genotypic comparison with meningiomas. Am J Surg Pathol 2004;28(2):207–14. [CrossRef]
[Pubmed]
18.
Rushing EJ, Bouffard JP, McCall S, Olsen C, Mena H, Sandberg GD, et al. Primary extracranial meningiomas: An analysis of 146 cases. Head Neck Pathol 2009;3(2):116–30. [CrossRef]
[Pubmed]
19.
Zhang DB, Chen T. Primary pulmonary meningioma: A case report and review of the literature. World J Clin Cases 2022;10(13):4196–206. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Acknowledgments
Artificial Intelligence (AI) Statement: No AI was utilized in the formulation and drafting of this manuscript.
Author ContributionsMoaz Alowami - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
John Agzarian - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Ehsan Haider - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Michael Bonert - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Asghar Naqvi - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionDr. Asghar Naqvi is the guarantor of submission and accepts full responsibility for the integrity of the work, had access to all the data in the study, and controlled the decision to publish.
Source of SupportNone
Consent StatementIn accordance with the research ethics board, patient consent was not required because no patient identifiers were used.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2025 Moaz Alowami et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}