 |
Case Report
Unique case study of HbS-β* thalassemia presenting as multifocal emphysematous osteomyelitis and life-threatening E. coli septicemia
1 Manager, Academics and Research, Fortis Memorial Research Institute, Gurgaon 122002, India
2 MBBS, DNB Resident, Fortis Memorial Research Institute, Gurgaon 122002, India
3 Associate Consultant, Paediatric Haematology Oncology & BMT Fortis Memorial Research Institute, Gurgaon 122002, India
4 Consultant, Infectious Disease, Fortis Memorial Research Institute, Gurgaon 122002, India
5 Consultant, Radiology, Fortis Memorial Research Institute, Gurgaon 122002, India
6 Senior Director & Unit Head, Internal Medicine, Fortis Memorial Research Institute, Gurgaon 122002, India
Address correspondence to:
Yogita Singh
Head, Academics and Research, Fortis Memorial Research Institute, Gurgaon 122002,
India
Message to Corresponding Author
Article ID: 101525Z01YS2025
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Singh Y, Jaiswal A, Kumar NM, Rastogi N, Mehta L, Parti A. Unique case study of HbS-β* thalassemia presenting as multifocal emphysematous osteomyelitis and life-threatening E. coli septicemia. Int J Case Rep Images 2025;16(2):69–72.ABSTRACT
Introduction: Sickle beta-thalassemia (S/β-thalassemia) is a compound heterozygous hemoglobinopathy with clinical manifestations influenced by the type of beta-thalassemia gene inherited. Sickle beta-thalassemia has a variable prevalence globally, ranging from 0.1% to 0.3% in certain Indian populations and higher rates in Mediterranean and African regions. Although osteomyelitis is a known complication in hemoglobinopathies, emphysematous osteomyelitis (EO)—a gas-forming, life-threatening infection—is exceptionally rare, particularly with Escherichia coli as the causative organism.
Case Report: Emphysematous Osteomyelitis commonly presents with localized bone pain, swelling, high-grade fever, and signs of systemic sepsis. Imaging typically reveals gas within the bone. A 32-year-old Asian male with a known history of sickle β-thalassemia major presented with high-grade fever, abdominal pain, and back pain. Previously treated for E. coli septicemia and subacute appendicitis, he showed persistent symptoms despite antibiotics. Imaging revealed multifocal EO involving the clavicles, sacrum, and shoulder joint. Bone biopsy confirmed E. coli infection. Hemoglobin electrophoresis (HPLC) confirmed sickle β-thalassemia major. Management included broad-spectrum intravenous (IV) antibiotics (imipenem, teicoplanin, polymyxin B), empirical antifungal therapy, hydroxyurea, and red blood cell exchange transfusion to reduce HbS below 30%. The patient showed clinical improvement and was discharged with a 6-week antibiotic regimen.
Conclusion: This is the first documented case of multifocal E. coli-induced emphysematous osteomyelitis in a patient with sickle β-thalassemia major. The case underscores the importance of early diagnosis through magnetic resonance imaging (MRI) and positron emission tomography-computed tomography (PET-CT), aggressive antimicrobial therapy, and hematologic optimization via exchange transfusion. Clinicians should consider atypical pathogens like E. coli in hemoglobinopathy-related infections for timely and effective intervention.
Keywords: Emphysematous osteomyelitis, E. coli, Hemoglobinopathy, Magnetic resonance imaging, Musculoskeletal radiology, PET-CT, Sickle beta-thalassemia
Introduction
Sickle beta-thalassemia (S/β-thalassemia) is a genetic disorder resulting from the inheritance of both a sickle cell gene and a at beta-thalassemia gene. The clinical presentation varies depending on whether the beta-thalassemia gene is β+ or β+o. Early diagnosis is essential for starting supportive treatment and forecasting the clinical course, especially in patients with homozygous sickle cell disease (SS disease) [1].
S/β-thalassemia occurs when one parent passes down an abnormal hemoglobin S gene and the other an abnormal beta-thalassemia gene. Both genes are located on chromosome 11, with one gene for each condition present on each chromosome [2]. The inheritance patterns are summarized in Table 1.
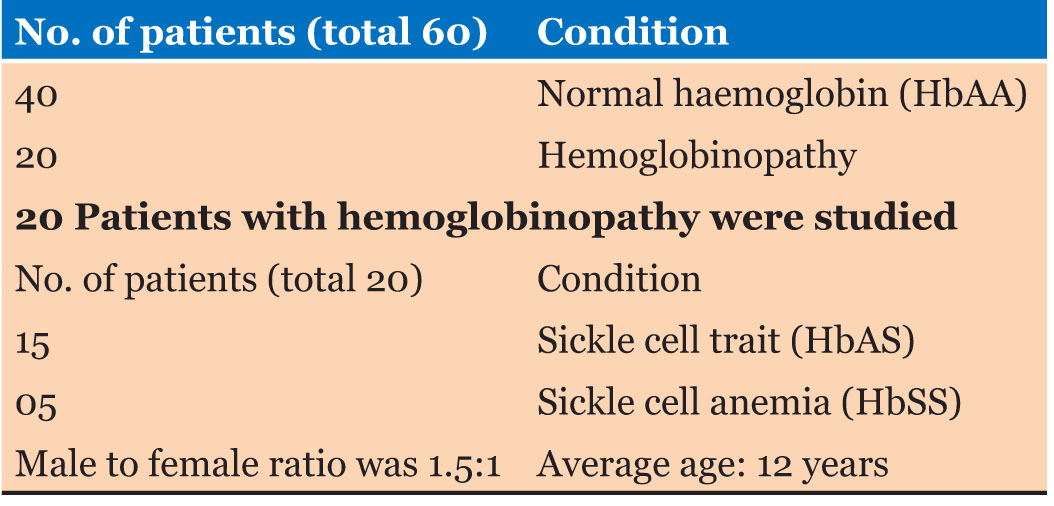
Chronic osteomyelitis is a major cause of prolonged illness in patients with hemoglobinopathies, especially in developing nations. A study in Nigeria by Onuminya and Onabowale [3] involving 60 chronic osteomyelitis patients found that 20 had hemoglobinopathies, with sickle cell trait (HbAS) and sickle cell anemia (HbSS) being the most prevalent as shown in Table 2. The femur was the most commonly affected bone, and treatment generally involved culture-specific antibiotics along with surgical procedures like saucerization and sequestrectomy.
Emphysematous osteomyelitis (EO) is a severe, life-threatening condition with a reported mortality rate of up to 32% [4]. Since the first case was reported in 1981, only 29 cases have been documented worldwide [5], EO is characterized by the formation of gas within the bone, often caused by anaerobic bacteria or members of the Enterobacteriaceae family, while Salmonella osteomyelitis is well known in sickle cell anemia, EO caused by E. coli is extremely rate, with just one previous case reported in a beta-thalassemia trait patient [6],[7].
This report describes a rare case of multifocal emphysematous osteomyelitis caused by E. coli in a 32-year-old male with sickle β+ thalassemia major, a combination not previously reported in the literature.

Case Report
A 32-year-old Asian male was admitted to a tertiary care hospital in Northern India on July 29, 2023, with a 15-day history of high fever, chills, lower abdominal pain, and back pain. He had previously been hospitalized 10 days earlier at another facility for subacute appendicitis and E. coli septicemia, but his condition worsened despite treatment. At the referring hospital, the patient was managed conservatively with intravenous antibiotics for subacute appendicitis. No rupture or surgical intervention was reported. E. coli was isolated from blood cultures during that admission, suggesting a gastrointestinal source of bacteremia.
Upon admission, his vitals were: pulse rate 122/min, blood pressure 140/90 mmHg, oxygen saturation 94% on room air, respiratory rate 18/min, and temperature 103 °F. Physical examination revealed course crepitations in both scapular regions and tenderness in the gluteal area.
Initial lab results showed microcytic anemia, thrombocytopenia, indirect hyperbilirubinemia, and nutritional deficiencies (iron, vitamin B12, and vitamin D) Hemoglobin levels were decreasing (7.7 g/dL), while white blood cell count was elevated (13,000/µL). C-reactive protein (CRP) was significantly high at 386.2 mg/L. Imaging studies included an unremarkable chest X-ray, an abdominal ultrasound showing hepatosplenomegaly, and a high-resolution CT (HRCT) of the chest indicating diffuse ground-glass opacities. Contrast-enhanced CT (HRCT) of the abdomen suggested subacute appendicitis, blood cultures grew E. coli (ESBL producer).
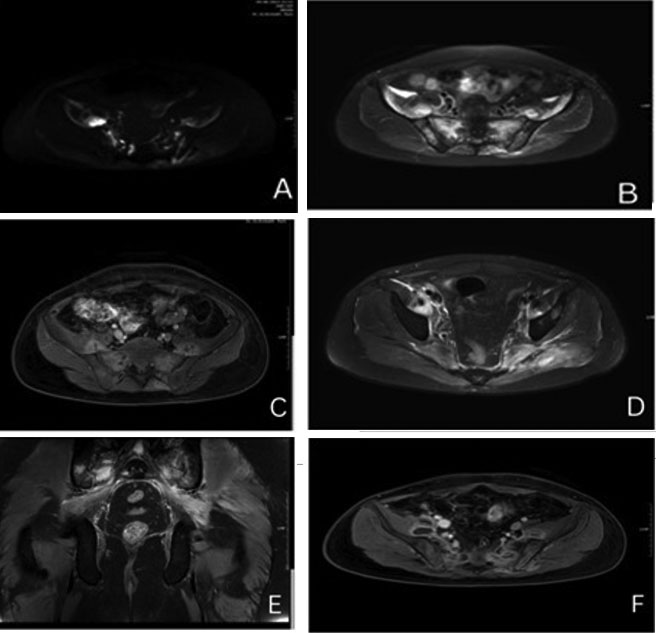
Despite treatment with meropenem and ciprofloxacin, the patient’s fever and back pain persisted. Further investigation with MRI and PET-CT revealed multifocal emphysematous osteomyelitis affecting the clavicles, sacrum, and left shoulder joint, along with adjacent soft tissue inflammation and abscess formation as shown in Figure 1. Deep bone biopsy and tissue cultures confirmed E. coli as the causative agent.
Sickle β+ thalassemia major was diagnosed based on high-performance liquid chromatography (HPLC) results (HbA 41.3%, HbA2 4.8%, HbF 8.0%, HbS 41.4%) and parental screening, which identified the mother the mother as a carrier of the beta-thalassemia trait.
Treatment involved intravenous antibiotics (imipenem, teicoplanin, and polymyxin B), empirical antifungal therapy, and hydroxyurea to prevent sickling. A partial red blood cell exchange transfusion was performed to reduce HbS levels to below 30%. The patient gradually improved clinically, with fever resolution and normalization of lab parameters. He was discharged with a plan for six weeks of intravenous ceftriaxone based on sensitivity profile of the E. coli isolate.
Discussion
Emphysematous osteomyelitis is a rare and potentially life-threatening condition, with E. coli being an unusual pathogen in sickle cell disease [8], while the link between sickle cell disease and osteomyelitis is well documented, Salmonella is typically the most common cause. This case emphasizes the need to consider fewer common pathogens like E. coli in patients with hemoglobinopathies.
The patient's treatment involved a team-based approach. The patient was managed by a multidisciplinary team involving internal medicine, infectious diseases, hematology, and surgery. Surgical consultation was essential for diagnostic evaluation and exclusion of residual intra-abdominal focus. Other modalities that included targeted antibiotics, surgery, and exchange transfusion to minimize sickling were also administered. Positron emission tomography-computed tomography and MRI were crucial in diagnosing multifocal emphysematous osteomyelitis, and tissue cultures confirmed E. coli as the causative organism. Given the patient’s recent history of subacute appendicitis and E. coli septicemia, this organism was suspected early. Although Salmonella is more typical in sickle cell disease, the recent gastrointestinal (GI) infection pointed to E. coli.
Conclusion
This case highlights the uncommon occurrence of E. coli-induced emphysematous osteomyelitis in sickle β+ thalassemia major and emphasizes the critical need for prompt diagnosis and aggressive treatment. A combination of exchange transfusion to lower Hbs levels and culture-targeted antimicrobial therapy is crucial for effectively managing these complex cases.
REFERENCES
1.
Luey C, Tooley D, Briggs S. Emphysematous osteomyelitis: A case report and review of the literature. Int J Infect Dis 2012;16(3):e216–20. [CrossRef]
[Pubmed]

2.
Needs T, Gonzalez-Mosquera LF, Lynch DT. Beta Thalassemia. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2025.
[Pubmed]
3.
Onuminya J, Onabowale B. Chronic osteomyelitis in patients who have haemoglobinopathy. Nigerian Medical Practitioner 2004;44(5)92–95. [CrossRef]
4.
Engh CA, Hughes JL, Abrams RC, Bowerman JW. Osteomyelitis in the patient with sickle-cell disease. J Bone Joint Surg Am 1971;53(1):1–15.
[Pubmed]
5.
Rayan F, Mukundan C, Shukla DD. A case of relapsing Salmonella osteomyelitis in a thalassaemia trait patient. J Orthop Traumatol 2009;10(1):31–3. [CrossRef]
[Pubmed]
6.
Ram PC, Martinez S, Korobkin M, Breiman RS, Gallis HR, Harrelson JM. CT detection of intraosseous gas: A new sign of osteomyelitis. AJR Am J Roentgenol 1981;137(4):721–3. [CrossRef]
[Pubmed]
7.
Potocki J, Kaushik S, Mira JL. Anaerobic osteomyelitis of femoral head with intraosseous, intra-articular, bursal and muscle pneumatosis. Skeletal Radiol 2003;32(1):46–8. [CrossRef]
[Pubmed]
8.
Ram A, Panneerselvam K, Muthiah R, Rajendran R. Emphysematous osteomyelitis due to Escherichia coli in a diabetic patient: A rare case report. J Infect Dev Ctries 2019;13(10):891–94.
SUPPORTING INFORMATION
Author Contributions
Yogita Singh - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Akhilesh Jaiswal - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Nikhil M Kumar - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Neha Rastogi - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Lakshay Mehta - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Amitabh Parti - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2025 Yogita Singh et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}