 |
Case Report
Spontaneous rupture of a giant liver hemangioma
1 MD, Specialist Radiology, Sohar Hospital, Sohar, Oman
2 MD, Consultant Interventional Neurovascular Radiologist, Sohar Hospital, Sohar, Oman
3 MD, Consultant Radiologist, Sohar Hospital, Sohar, Oman
Address correspondence to:
Jamila Omar Abdalla
MD, Specialist Radiologist, Sohar Hospital, Sohar, Al Batinah,
Oman
Message to Corresponding Author
Article ID: 101519Z01JA2025
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Abdalla JO, Al-Risi M, Tayfor M, Selim YAR. Spontaneous rupture of a giant liver hemangioma. Int J Case Rep Images 2025;16(2):35–39.ABSTRACT
Introduction: Liver hemangiomas are the most prevalent benign hepatic tumors, which are frequently found incidentally when imaging for other conditions. They typically do not have any symptoms and do not require treatment. However, spontaneous rupture is an uncommon but potentially deadly consequence that mostly affects large hemangiomas. The patient described in this case study had anemia and abdominal discomfort. He was diagnosed by computed tomography (CT) and managed successfully by transarterial embolization.
Case Report: We report on an 80-year-old man who was blind, known to have hypertension, old stroke, epilepsy, recurrent lower limb deep-vein thrombosis. He was on multiple medications for forementioned conditions and on oral anticoagulants. He presented to our emergency department with vomiting and abdominal discomfort for a few days. There was low hemoglobin (6.26 g/dL), increased lactate (9.17 mmol/L), low blood pressure (90/40 mmHg) and heart rate (80/min) at admission. A heterogenous low echoic liver mass and intra-abdominal free fluid was seen on bedside sonography. An intra-abdominal hemorrhage and a ruptured liver hemangioma with subcapsular hematoma were discovered by CT. After a CT scan, the patient experienced tachycardia with a heart rate (HR) of 150 beats per minute. Urgent transarterial embolization was done after stabilization. The patient was admitted under observation for 12 days following intervention and then discharged.
Conclusion: Spontaneously ruptured hepatic hemangiomas are quite uncommon which can be easily diagnosed by CT. Transarterial embolization may be an alternative management to surgery in certain instances of atraumatic, ruptured hepatic hemangiomas.
Keywords: Embolization, Liver hemangioma, Spontaneous rupture
Introduction
Hepatic hemangiomas are common benign liver tumors and the second most common tumor seen in the liver after metastases. Most of the patients with hepatic hemangioma have no clinical symptoms and are only followed up. The prevalence, according to autopsy studies, ranges from 3% to 20%, with manifestations which are frequently asymptomatic [1]. Spontaneous rupture giant hemangiomas are an uncommon complication. Hepatic hemangiomas can be as large as 20 cm in diameter; however, they are usually modest (less than 4 cm) and solitary. Most of the patients, despite their size, have no symptoms [2]. The relationship between hemangioma size and rupture risk is not supported by science, however in a few cases, other factors like trauma or anticoagulant medications were found to play a role [3].
Only 20 cases of spontaneous rupture of hepatic hemangiomas have been reported in the literature, indicating that such events are uncommon [1].
An ultrasound evaluation of this emergency showed that there was free intraperitoneal fluid present. However, arterial and venous phase contrast-enhanced CT scanning is the gold standard modality for the diagnosis.
Case Report
An 80-year-old male presented with vomiting and abdominal pain of few days duration in emergencies. His medical history was notable for a stroke, hypertension, epilepsy, and recurrent lower limb deep-vein thrombosis (DVT). He is on several medications for these and has been taking oral anticoagulants. He was anemic (6.26 g/dL), had high lactate (9.17 mmol/L), low blood pressure (90/40 mmHg), and heart rate of 80 bpm at his due course of admission. On physical examination, there was widespread abdominal tender and mild sign of peritoneal irritation which localized to the upper abdomen. A bedside ultrasound was done, revealing a heterogeneous hypoechoic mass in the right liver lobe associated with intraperitoneal fluid in the splenorenal and hepatorenal spaces, as well as in the rectovesical pouch. Further evaluation with contrast-enhanced CT scan was recommended.
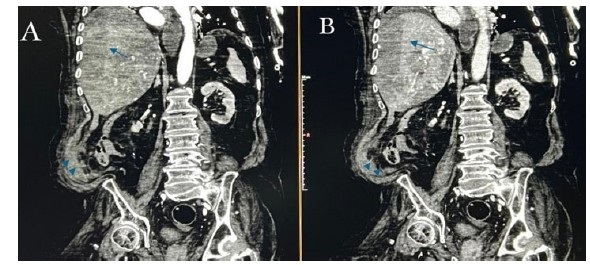
A CT scan was performed, showing a large hypodense mass with peripheral enhancement in the right hepatic lobe segments VI and VII, along with lentiform fluid beneath the capsule and in the intraperitoneal recesses, with density measuring approximately 56–58 HU, indicative of hemorrhage (Figure 1 and Figure 2).
After a CT scan, the patient was hemodynamically unstable, with following vitals: a heart rate of 150 beats per minute, and a blood pressure of 90/40 mmHg alongside a hemoglobin level of 6.26 g/dL, and an elevated International Normalized Ratio (INR) of 3.8. He was transfused with two units of blood and four units of platelets, 10 mg of vitamin K stat, four units of fresh frozen plasma (FFP), one unit of packed red blood cells (PRBC), Verapamil 2.5 mg was given slowly via intravenous (IV) route, and Lanoxin 500 mcg. The patient was maintained on IV fluids at a rate of 65 mL/h, received nasogastric tube (NGT) feeding, and was prescribed antibiotics.
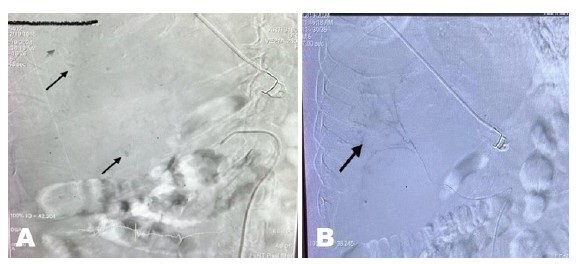
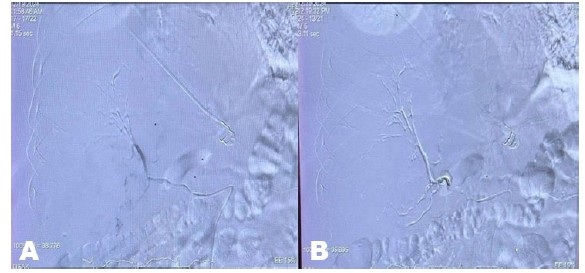
The patient regained his hemodynamic stability and a hemoglobin of 8.6 g/dL, he was sent to interventional radiology (IR) angio suite for embolization and controlling of bleeding. Under fluoroscopy selective hepatic artery angiogram revealed right liver lobe spotty contrast deposits, no arteriovenous fistula (AV fistula) or tumor vessels noted, features indicating benign right hepatic lobe hemangioma.
Microcatheter super selective embolization of the feeders was performed using glue, followed by coiling and occlusion of the right hepatic artery (Figure 3 and Figure 4). The left hepatic artery and gastro-duodenal artery were preserved. The procedure was performed under local anesthesia.
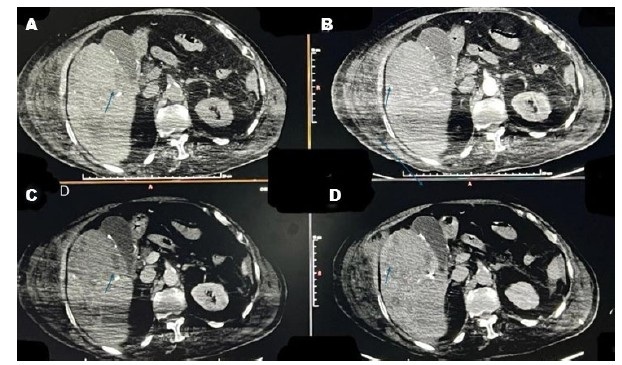
A follow-up CT scan a week later showed intraperitoneal hemorrhage had decreased and the hepatic subcapsular hematoma had slightly shrunk. Despite not being enhanced, the giant hepatic hemangioma has increased in density; it read between 70 and 80 HU, which indicates a clotted hematoma (Figure 5).
Following a successful intervention, the patient spent 12 days in the hospital under supervision and was released from the hospital after a smooth recovery.

Discussion
Liver hemangiomas are benign tumors of the liver that are more common in women. Hemangiomas can range in size from less than 1 cm to more than 20 cm, and they are typically seen in the right liver lobe subcapsular area [4].
Hepatic hemangiomas are considered large when they have a diameter of more than 5 cm and may cause symptoms such as internal bleeding, rupture, abdominal pain, and coagulation disorders [5].
It usually grows slowly and is typically small, asymptomatic, and incidentally found during abdominal imaging for another reason. Less than 40% of cases involve the hepatic hemangioma progressing. Perhaps hormone stimulation contributes to hepatic hemangioma growth [5].
The rupture of hepatic hemangioma with hemoperitoneum is a rare (1–4%) but frequently lethal consequence, with a high mortality rate of 60–75% [6]. Usually, its clinical symptoms are not specific. Severe abdominal pain, hemoperitonea anemia, and disseminated intravascular coagulopathy are a few examples of clinical manifestations. Emergency management should only be necessary in these situations. Individuals who have concomitant conditions and comorbidities may be at high risk for liver transplant surgery [7].
One useful method for treating giant liver hemangiomas in people who are not candidates for surgery is transcatheter arterial embolization (TAE). The ability to destroy the vascular supply of these lesions and less invasive techniques are a more important benefit than surgery.
Conclusion
An accurate clinical decision-making and therapy would follow a hemangioma’s diagnosis as the cause of hemoperitoneum. Contrast-enhanced CT and immediate management are very important ruptured hepatic hemangioma.
Optimizing results requires careful patient selection, planning, and follow-up. One effective and minimally invasive treatment for patients with large liver hemangiomas is TAE. Through our case, we seek to raise awareness of this clinical practice consequence. This necessitates re-evaluating surgical indications.
REFERENCES
1.
Sciano D, Mingione A, Pezzulo CM, Lombari P, Iarrobino F, Donnarumma MC, et al. Spontaneous rupture of hepatic hemangioma: Case report and literature review. Il G Chir 2024;44(4):e50.

2.
Gandolfi L, Leo P, Solmi L, Vitelli E, Verros G, Colecchia A. Natural history of hepatic haemangiomas: Clinical and ultrasound study. Gut 1991;32(6):677–80. [CrossRef]
[Pubmed]
3.
Donati M, Stavrou GA, Donati A, Oldhafer KJ. The risk of spontaneous rupture of liver hemangiomas: A critical review of the literature. J Hepatobiliary Pancreat Sci 2011;18(6):797–805. [CrossRef]
[Pubmed]
4.
Choi BY, Nguyen MH. The diagnosis and management of benign hepatic tumors. J Clin Gastroenterol 2005;39(5):401–12. [CrossRef]
[Pubmed]
5.
Leon M, Chavez L, Surani S. Hepatic hemangioma: What internists need to know. World J Gastroenterol 2020;26(1):11–20. [CrossRef]
[Pubmed]
6.
Jain V, Ramachandran V, Garg R, Pal S, Gamanagatti SR, Srivastava DN. Spontaneous rupture of a giant hepatic hemangioma – Sequential management with transcatheter arterial embolization and resection. Saudi J Gastroenterol 2010;16(2):116–9. [CrossRef]
[Pubmed]
7.
Tonpe S, Warbhe H, Banode P, Bandi S, Suryadevara M, Reddy Guggella S. A case report: Giant liver hemangioma treated with transcatheter embolization. Cureus 2024;16(8):e65927. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Jamila Omar Abdalla - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Maimouna Al-Risi - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Mohamed Tayfor - Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Yasser AR Selim - Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2025 Jamila Omar Abdalla et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}