 |
Case Series
Electrolyte imbalance in infants with diarrhea worsened by improper dilution of oral rehydration salt (ORS): Case reports from primary healthcare setting in Rohingya refugee camp
1 International Organization for Migration (IOM), Cox’s Bazar, Bangladesh
2 Université Paris Cité, Paris, Île-de-France, France
Address correspondence to:
Charls Erik Halder
International Organization for Migration (IOM), Cox’s Bazar,
Bangladesh
Message to Corresponding Author
Article ID: 101515Z01CH2025
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Halder CE, Das NK, Tasnim S, Sayum MA, Hasan MA, Soma ER, Okello JC. Electrolyte imbalance in infants with diarrhea worsened by improper dilution of oral rehydration salt (ORS): Case reports from primary healthcare setting in Rohingya refugee camp. Int J Case Rep Images 2025;16(2):14–19.ABSTRACT
Healthcare workers often miss to properly communicate on the proper way of oral rehydration salt (ORS) preparation, especially, regarding the volume of water to be mixed to get appropriate concentration of solution. Severe complications, like electrolyte imbalance and acute gastrointestinal (GI) bleeding, can happen if prepackaged ORS is dissolved in a smaller amount of water than the recommended amount. We presented here case reports of two infants from the Rohingya refugee camps with the diagnosis of acute watery diarrhea with dehydration and hypernatremia, potentially worsened by excessive salt intake due to inappropriate dilution of ORS.
Keywords: Diarrhea, Electrolyte imbalance, Infant, Oral rehydration therapy, Refugee camps, Rohingya
Introduction
In 2021, there were 1.17 million deaths worldwide attributed to diarrheal diseases, which represent a reduction of over 60% from the figures reported in 1990 [1]. However, still it remains a leading cause of death in infants and young children, particularly in developing countries and low-resource settings. The deaths are mostly attributed to dehydration [2].
Dehydration from diarrhea can be prevented and treated simply with oral rehydration salt (ORS), a cheap and effective treatment that has saved 70 million lives worldwide [3]. Commercially prepackaged ORS should be dissolved in the appropriate volume of water, which may vary between 500 and 1000 mL, depending on the specific pharmaceutical formulation or package volume [2].
Although, as of 2025, ORS is commonly prescribed by healthcare workers and it is well known to caregivers, evidence suggests that there remains a significant knowledge gap among caregivers on preparation of ORS [4]. Healthcare workers often miss to properly communicate on the proper way of ORS preparation, especially, regarding the volume of water to be mixed to get appropriate concentration of solution [5]. The availability of different packages (500 vs 1000 mL) by different health partners and providers may also create confusion [6]. Such knowledge gaps and poor communication can be pronounced in refugee settings, like Rohingya refugee camps, due to poverty, illiteracy, and overstraining of health system [7].
A few case reports suggest that severe complications can be resulted if prepackaged ORS is dissolved in a smaller amount of water than the recommended amount, including electrolyte imbalance [8] and acute gastrointestinal (GI) bleeding [9]. We experienced two cases of electrolyte imbalance in infants with diarrhea in a refugee setting, potentially worsened due to improper dilution of ORS. From the cases, we have tried to draw the lesson that improper knowledge and practice of caregivers on preparation of ORS can cause severe life-threatening complications, like electrolyte imbalance, which is often difficult to diagnose in resource-poor settings.
CASE SERIES
Case 1
A 7-month-old infant, Rohingya, male, presented at one of the refugee camp-based infectious disease treatment centers in Cox’s Bazar, Bangladesh, operated by International Organization for Migration (IOM), complaining of passage of loose watery stools for two days and three episodes of vomiting since the previous night. The stool was watery, and the vomiting was non-bilious and non-projectile. The patient was referred from a primary healthcare center with the diagnosis of acute watery diarrhea due to probable cholera (rapid diagnostic test positive) with some signs of dehydration. Based on clinical assessment, the dehydration was classified as moderate. The patient had a history of intake of concentrated oral rehydration saline meaning that the ORS was not diluted properly with the recommended amount of water. The ORS was prepared by the child’s father at home without knowing properly the exact volume of water required to prepare the solution. The child did not have a history of fever, abdominal distension, or significant decrease in urine output. Furthermore, there were no reports of similar illnesses among family members or close contacts. The family accessed drinking water from a deep tube well in their block, which is only accessible two times a day, 8–9 AM and 3–4 PM, indicating difficulty in accessing safe drinking water round-the-clock.
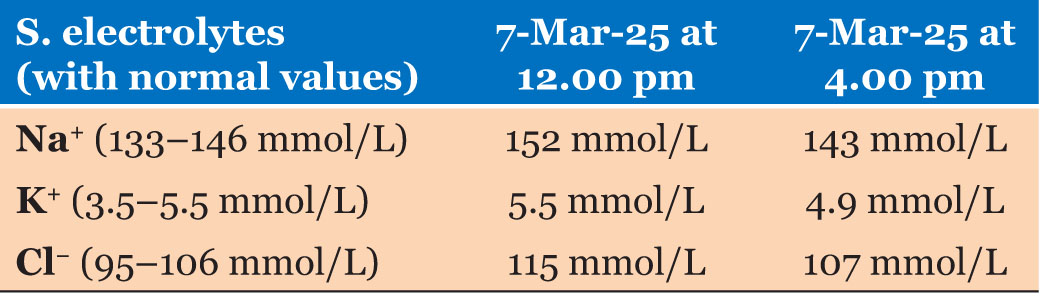
On examination, we found that the child was slightly lethargic with some signs of dehydration (moderate dehydration), especially sunken eyes, increased thirst (eager to drink) and slow return of the skin pinch. His vital signs were within the expected range, with temperature of 36.9 °C, pulse of 144 bpm, and respiratory rate of 36 breaths per minute. On investigation of serum electrolytes, his sodium level was found moderately elevated (152 mmol/L) and serum creatinine remained within the normal range. We diagnosed that patient as a case of acute watery diarrhea with some sign of dehydration with hypernatremia. The possible cause of dehydration and electrolyte imbalance was diarrhea with probable cholera, which could be worsened by excessive salt intake due to inappropriate dilution of ORS (Table 1).
After stabilization at emergency room, the patient was admitted to the inpatient ward, where diarrhea, dehydration and electrolyte imbalance were managed through continuation of breastfeeding, plain water, azithromycin (for cholera) and the slow administration of half neutralized sodium chloride (0.45% sodium chloride and 5% dextrose solution IV). After initiating correction and close monitoring for 4 hours, the patient’s condition stabilized. Full normalization of electrolytes was confirmed later during hospitalization. The dehydration was also resolved. With continuation of treatment with plan A (with ORS) the child was discharged.
Case 2
A 4-month-old infant, Rohingya, male, presented to one of the infectious disease treatment centers, operated by IOM in the refugee camp in Cox’s Bazar with a history of passing loose watery stools for approximately 10 times and vomiting 3 times in the past 24 hours. The illness started suddenly, stools were watery in consistency and without blood or mucus. The vomiting was non-projectile and contained partially digested milk. The mother reported that the child had reduced oral intake, showed irritability and reduced urine output. The child did not have a history of fever, abdominal distension, or convulsions. As per the mother’s statement the patient was treated initially with syrup Nitazoxanide, syrup Zinc Sulfate, and ORS. However, ORS was not prepared correctly, as the volume of water used to dissolve the ORS was less than the recommended volume. The child’s family can access drinking water from a deep tube well in their block only from 8 to 9 AM in a day.
On examination, the child was lethargic with signs of severe dehydration including sunken eyes, unable to drink, very dry and furred tongue and a very slow return of skin pinch. There were no signs of anaemia, jaundice, cyanosis, edema, lymphadenopathy, or organomegaly. He was tachycardic with pulse rate of 163 bpm and respiratory rate of 45 breaths per minute. His axillary temperature was 36.2 °C and saturation of oxygen (SpO2) was 98% on room air. Nothing significant was found on systemic examination. After the relevant investigations, we found a moderately high serum sodium level of 167 mmol/L with the rest of the test parameters were within the normal range. Rapid diagnostic test for cholera was negative. There were no signs of gastrointestinal bleeding (GI) observed during examination and throughout the hospital stay.
The case was diagnosed as acute watery diarrhea with severe dehydration and severe hypernatremia. After initial stabilization in the emergency room, the patient was admitted to the inpatient department. After correction of dehydration with cholera saline, plain water and breastfeeding, we started the slow correction of hypernatremia by half neutralized normal saline (0.45% sodium chloride and 5% dextrose IV). His hypernatremia was corrected slowly, at a rate of no more than 0.5 mmol/L/h and returned to normal limits in 48 hours. The child was stabilized and switched to oral treatment (Table 2).

Discussion
This case report is among the few that document incidents of salt toxicity caused by improper dilution of ORS in the Indian sub-continent, and one of the first reports from refugee setting [10]. Improperly prepared oral rehydration salt has resulted in hypernatremia [8],[10] and gastrointestinal bleeding [9], sometimes with fatal outcomes [8]. Theoretically, when ORS is diluted in a smaller volume of water, there is high concentration of sodium in the solution, the intake of which would increase the sodium level of plasma. If it is associated with diarrhea, dehydration may worsen due to high concentration of sodium, resulting in signs and symptoms of dehydration and hypernatremia, such as thirst, lethargy, irritability, seizure and coma.
In our cases, both children had a history of diarrhoea with concentrated intake of ORS, which potentially exacerbated the dehydration and resulted in salt toxicity. This has been further evidenced from the results of plasma electrolytes demonstrating hypernatremia. There is a dilemma in managing dehydration due to concentrated ORS, while some academic guidelines suggest rapid correction [2], most recommend for slow correction [11],[12]. We have successfully treated both children with slow correction of hypernatremia.
In Rohingya refugee camps, there are two formulations available of ORS, one where one sachet should be diluted in 500 mL water, while the other with 1000 mL. Moreover, there is high rate of illiteracy among the Rohingya refugees [7]. Therefore, if the healthcare workers do not provide appropriate information on preparation of ORS, the caregivers can improperly dilute ORS resulting in severe and fatal outcomes [13]. Furthermore, in such resource poor setting, most primary care centres lack sufficient equipment for biochemical analysis, especially for serum electrolytes. Therefore, there is high chance that diagnosis of electrolyte imbalance could be missed by the clinicians resulting in poor outcome of treatment [14]. Additionally, the exact amount of ORS administered could not be confirmed, as caregivers were unable to recall the volume given per day or per kilogram of body weight.
To ensure proper dilution of ORS with the proper volume of water at the client level, we propose:
- International standardization of the ORS formulation or having country-level health authorities to regulate one specific type of sachet with a consistent volume of water to avoid confusion at the client level.
- Clinicians should spend more time to demonstrate how to prepare ORS, preferably providing the first dose in the presence of the caretaker.
- To ensure package labelling having clear instructions for mixing ORS.
- To provide accurate information to the community on the proper mixing of ORS.
Conclusion
From our cases it is evident that improper knowledge and practice of caregivers on preparation of ORS properly can result in electrolyte imbalance among infants. Though, we have successfully treated our cases with slow correction of hypernatremia, it required availability of biochemical analysis, especially, serum electrolyte, which is often not available in resource-poor settings, like refugee camps. Therefore, proper communication should be provided to the caregivers, and awareness should be raised among the community on preparation of ORS in proper way to prevent such incidents.
REFERENCES
1.
GBD 2021 Diarrhoeal Diseases Collaborators. Global, regional, and national age-sex-specific burden of diarrhoeal diseases, their risk factors, and aetiologies, 1990–2021, for 204 countries and territories: A systematic analysis for the Global Burden of Disease Study 2021. Lancet Infect Dis 2025;25(5):519–36. [CrossRef]
[Pubmed]

2.
Global Health Supply Chain Program. MNCH Commodities: Oral Rehydration. 2019. [Available at: https://www.ghsupplychain.org/sites/default/files/2019-02/MNCH%20Commodities-OralRehydration.pdf]
3.
Mahfuz M, Tariful Islam Khan AKM, Yunus M. Development of oral rehydration salt solution: A triumph of medical science. Indian J Med Res 2024;160(1):6–9. [CrossRef]
[Pubmed]
4.
Alam N, Hossain M, Rahman A. Knowledge and practice of oral rehydration solution preparation among caregivers in rural Bangladesh. J Health Popul Nutr 2020;38(1):1–7.
5.
Khan MA, Sultana R, Ahmed T. Communication gaps in ORS preparation instructions by healthcare providers: A cross-sectional study. BMC Public Health 2021;21(1):1123.
6.
ColaLife. How many sachets of ORS should an ORS/ zinc co-pack contain and what size should they be? [Blog post]. 16 February, 2023. [Available at: https://www.colalife.org/2023/02/16/how-many-sachets-of-ors-should-an-ors-zinc-co-pack-contain-and-what-size-should-they-be]
7.
Education Cluster, REACH Bangladesh, and Inter-Sector Coordination Group. Bangladesh: Assessment of the Education Sector response to the Rohingya crisis – Rohingya refugee response (March 2021). 2021. [Available at: https://reliefweb.int/report/bangladesh/bangladesh-assessment-education-sector-response-rohingya-crisis-rohingya-refugee]
8.
Quereshi AM. Hypernatraemia due to improperly prepared oral rehydration salts: A case study. J Pediatr Emerg Care 2010;26(4):321–5.
9.
Chung HY. Acute gastrointestinal bleeding following excessive sodium intake from oral rehydration solution: A rare case. Pediatr Gastroenterol Hepatol Nutr 2020;23(4):405–10.
10.
Das SK. Overdilution and underdilution of ORS: Consequences and prevention. J Med Case Rep 2015;9(1):211.
11.
American Academy of Pediatrics. Hypernatremia. In: Kimberlin DW, Brady MT, Jackson MA, Long SS, editors. Red book: 2018 Report of the Committee on Infectious Diseases. 31st ed. Elk Grove Village, IL: American Academy of Pediatrics; 2018.
12.
Aghsaeifard Z, Heidari G, Alizadeh R. Understanding the use of oral rehydration therapy: A narrative review from clinical practice to main recommendations. Health Sci Rep 2022;5(5):e827. [CrossRef]
[Pubmed]
13.
Ahmed RH, Chowdhury N, Jahan S. Misadministration of ORS: Implications for dehydration management in children. Int J Public Health Res 2019;10(2):112–25.
14.
BMC Health Services Research. MSF experiences of providing multidisciplinary primary level NCD care for Syrian refugees and the host population in Jordan: An implementation study. 2021. [Available at: https://bmchealthservres.biomedcentral.com/articles/10.1186/s12913-021-06333-3]
SUPPORTING INFORMATION
Acknowledgments
We sincerely thank all healthcare workers for their successful patient management. We also acknowledge the Migration Health Division (MHD) Research Unit of the International Organization for Migration (IOM) for reviewing the case report.
Author ContributionsCharls Erik Halder - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Niranta Kumar Das - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Sumaya Tasnim - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Md Abu Sayum - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Md Abeed Hasan - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Emmanuel Roba Soma - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
James Charles Okello - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2025 Charls Erik Halder et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}