 |
Case Report
Spontaneous gallbladder perforation presenting as gastroenteritis
1 Emergency Department, Royal Lancaster Infirmary, University Hospitals of Morecambe Bay NHS Foundation Trust, Lancaster, United Kingdom
Address correspondence to:
Muhammad Faisal Khilji
Emergency Department, Royal Lancaster Infirmary, Ashton Road, LA1 4RP, Lancaster,
United Kingdom
Message to Corresponding Author
Article ID: 101492Z01MK2025
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Khilji MF, Saeed MA. Spontaneous gallbladder perforation presenting as gastroenteritis. Int J Case Rep Images 2025;16(1):20–23.ABSTRACT
Introduction: Spontaneous gallbladder perforation is a rare condition associated with high mortality.
Case Report: We present a case of a 75-year-old woman presenting with diarrhea, vomiting, and abdominal pain that began the same day. Her stools were loose, watery, brownish in color and contained no blood or mucous. She vomited several times since morning and her abdominal pain was mainly central and not radiating anywhere. She was vitally stable and moderately dehydrated on examination with mild umbilical tenderness and audible gut sounds. Her blood investigations showed slightly raised inflammatory markers with normal Amylase and Lactate. Intravenous hydration was started with anti-emetic injection. As she was dehydrated and vomiting persistently, she was referred to Medicine for continued hydration. Later in the ward her computed tomography (CT) abdomen was done due to her persistent abdominal pain which showed perforated gallbladder. She was then referred to surgeons and she was treated with intravenous antibiotics and pigtail cholecystostomy drain. She was discharged after eight days with oral antibiotics, a drain in place, and red flags explained. The patient did not behave clinically or biochemically as perforated gallbladder making it a case of spontaneous gallbladder perforation.
Conclusion: Spontaneous gallbladder perforation can present in a number of different ways including gastroenteritis. The possibility of spontaneous gall bladder perforation should be considered if abdominal pain is not settling in an elderly patient.
Keywords: Gallbladder, Gastroenteritis, Spontaneous perforation
Introduction
The gallbladder perforation is a serious condition that requires immediate surgical intervention [1]. It is an important complication of acute cholecystitis and its incidence ranges between 2% and 18% [2]. The incidence of acalculous perforation is higher than calculous perforation [3]. Gallbladder perforations present clinically in the same way despite different etiologies [4]. Rarely gallbladder perforation occurs without typical clinical, radiological, or histopathological features of perforation called spontaneous gallbladder perforation and the diagnosis is usually missed or delayed in such conditions [5]. Our patient presented with gastroenteritis and did not behave clinically or biochemically as perforated gallbladder making it a case of spontaneous gallbladder perforation.
Case Report
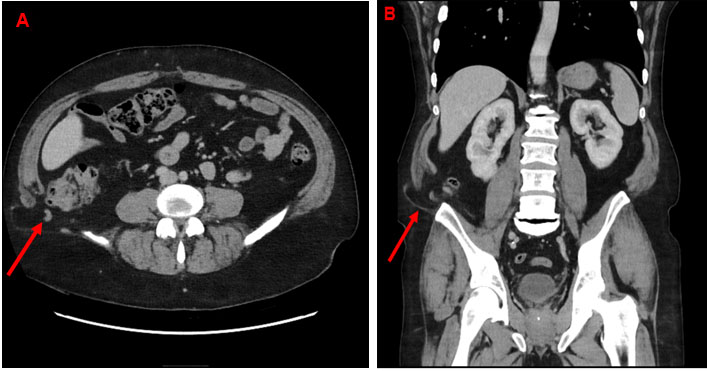
A 75-year-old woman came to the emergency department (ED) with complaint of diarrhea, vomiting, and abdominal pain for one day. Abdominal pain was in whole abdomen and colicky in nature without any aggravating or relieving factors. Her stools were loose, watery, brownish in color and contain no blood or mucous. She vomited several times since morning and her abdominal pain was mainly central and not radiating anywhere. She was vitally stable, afebrile, and moderately dehydrated on examination with mild umbilical tenderness and audible gut sounds. She was maintaining her vitals, but as she was still having symptoms, she was treated symptomatically. Blood tests were done and she was referred to the medical team for admission. Her blood showed white cell count of 11.8×109/L and C-reactive protein of 12 mg/L. Her serum amylase, glucose, renal, and liver functions were normal. Her symptoms of diarrhea and vomiting settled by the next day but as her abdominal pain was not improving, hence, she was referred to the surgical team. Her abdominal examination showed mild tenderness in epigastric and right hypochondriac areas but not peritonitic. Her CT abdomen was done which showed acute cholecystitis with possible small perforation of gallbladder (Figure 1).
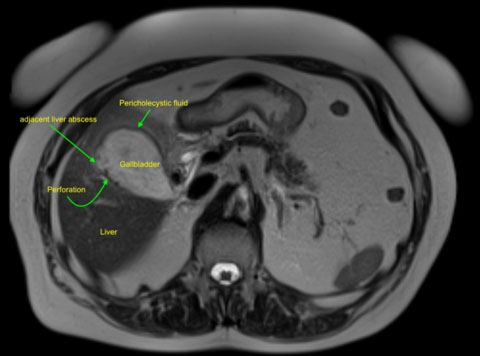
Her magnetic resonance cholangiopancreatography (MRCP) was done after two days which showed perforation of gallbladder with 4×4.5 cm abscess in adjacent liver (Figure 2).
She was treated with intravenous antibiotics and pigtail cholecystostomy drain. She was discharged after eight days with oral antibiotics, a drain in place, and red flags explained. She was seen weekly in the outpatient department where every time she presented asymptomatically and finally her cholecystostomy tube was removed after four weeks when the output was nil.

Discussion
Gallbladder perforation is associated with high mortality and classified by Niemeier, in 1934, into three types, type 1 acute perforation with peritonitis, type 2 subacute perforation with pericholecystic abscess, and type 3 as chronic perforation forming fistula [6],[7],[8]. Spontaneous perforation is caused by ischemia, infection, and lithiasis. The most common cause of perforation is the ischemia of fundus of gallbladder due to the blockage of the most distant feeding artery. The typical presentation of gallbladder perforation is clinical peritonitis in the form of abdominal pain, fever, and sickness [9],[10]. According to Chen et al., sudden loss of intra-cholecystic pressure due to perforation causes abrupt relief in pain of the patient; however, if left untreated the patient will soon become toxic as reported by Gore et al. [11],[12]. It is usually diagnosed by ultrasound or CT scan, showing a thickened gallbladder wall and pericholecystic fluid collection [13]. Ultrasonography can be used for the diagnosis but CT scan is more sensitive. The findings of CT scan are cholecystic including thickening of wall, intramural abscess, and gallstones. The pericholecystic CT scan findings include pericholecystic fluid, abscess, and fat stranding [14]. Inflammatory markers are raised with deranged liver enzymes. The diagnosis between acute cholecystitis and perforated gallbladder is difficult. Usually, surgical treatment is used for type 1 gallbladder perforation but in spontaneous perforation, type 2 as in our case, the conservative treatment the conservative treatment with intravenous antibiotics and pigtail catheter placement is often used. In our patient conservative approach was chosen due to the lack of acute features, relatively normal inflammatory markers, and age of the patient. This approach was used in studies by Biolato et al. and Basara et al. Biolato et al. used this approach to avoid post-cholecystectomy complications in a patient waiting for liver transplant and Basara et al. used this approach in an elderly patient with spontaneous gall bladder perforation [15],[16].
Conclusion
Spontaneous gallbladder perforation is rare and can present in a number of different ways, as in our case presented as gastroenteritis. If abdominal pain is not settling specially in elderly, then possibility of spontaneous gallbladder perforation should be considered. Early diagnosis and treatment are important as they are associated with significant morbidity and mortality.
REFERENCES
1.
Menakuru SR, Kaman L, Behera A, Singh R, Katariya RN. Current management of gall bladder perforations. ANZ J Surg 2004;74(10):843–6. [CrossRef]
[Pubmed]

2.
Roslyn J, Busuttil RW. Perforation of the gallbladder: A frequently mismanaged condition. Am J Surg 1979;137(3):307–12. [CrossRef]
[Pubmed]
3.
Kalliafas S, Ziegler DW, Flancbaum L, Choban PS. Acute acalculous cholecystitis: Incidence, risk factors, diagnosis, and outcome. Am Surg 1998;64(5):471–5.
[Pubmed]
4.
Kwon KH, Hong SJ, Park CW, et al. A case of gallbladder perforation treated by percutaneous transhepatic chotecystic drainage and percutaneous peritoneal drainage. Korean J Gastrointesti Endosc 1994;14:482–8.
5.
Tanaka M, Takahashi H, Yajima Y, Okamura K, Kosaka A, Mizumoto R. Idiopathic perforation of the gallbladder: Report of a case and a review of the Japanese literature. Surg Today 1997;27(4):360–3. [CrossRef]
[Pubmed]
6.
MacDonald JA. Perforation of the gallbladder associated with acute cholecystitis: 8-year review of 20 cases. Ann Surg 1966;164(5):849–52. [CrossRef]
[Pubmed]
7.
Jansen S, Doerner J, Macher-Heidrich S, Zirngibl H, Ambe PC. Outcome of acute perforated cholecystitis: A register study of over 5000 cases from a quality control database in Germany. Surg Endosc 2017;31(4):1896–900. [CrossRef]
[Pubmed]
8.
Niemeier OW. Acute free perforation of the gallbladder. Ann Surg 1934;99(6):922–4. [CrossRef]
[Pubmed]
9.
Badru F, Litton T, Puckett Y, Bansal S, Guzman M, Vane D, Villalona GA. Spontaneous gallbladder perforation in a child secondary to a gallbladder cyst: A rare presentation and review of literature. Pediatr Surg Int 2016;32(6):629–34. [CrossRef]
[Pubmed]
10.
Mirza B, Ijaz L, Saleem M, Iqbal S, Sharif M, Sheikh A. Management of biliary perforation in children. Afr J Paediatr Surg 2010;7(3):147–50. [CrossRef]
[Pubmed]
11.
Chen JJ, Lin HH, Chiu CT, Lin DY. Gallbladder perforation with intrahepatic abscess formation. J Clin Ultrasound 1990;18(1):43–5. [CrossRef]
[Pubmed]
12.
Gore RM, Ghahremani GG, Joseph AE, Nemcek AA Jr, Marn CS, Vogelzang RL. Acquired malposition of the colon and gallbladder in patients with cirrhosis: CT findings and clinical implications. Radiology 1989;171(3):739–42. [CrossRef]
[Pubmed]
13.
Soiva M, Pamilo M, Päivänsalo M, Taavitsainen M, Suramo I. Ultrasonography in acute gallbladder perforation. Acta Radiol 1988;29(1):41–4.
[Pubmed]
14.
Sheoran SK, Sahai RN, Indora J, Biswal UC. Spontaneous perforation of gallbladder: Case report. Gastroenterology Res 2016;9(2–3):61–3. [CrossRef]
[Pubmed]
15.
Başara I, Seçil M. Spontaneous asymptomatic gallbladder perforation. Quant Imaging Med Surg 2014;4(3):212–3. [CrossRef]
[Pubmed]
16.
Biolato M, Tarli C, Marrone G, et al. Gallbladder perforation without cholecystitis in a patient awaiting liver transplantation: A peculiar case report of anaemia in cirrhosis. BMC Gastroenterol 2019;19(1):112. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Muhammad Faisal Khilji - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Muhammad Akbar Saeed - Conception of the work, Design of the work, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestThe case was presented as poster presentation in “RCEM EMSAS conference” at Scarborough on 13th and 14th November 2024.
Copyright© 2025 Muhammad Faisal Khilji et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}