 |
Letter to Editor
Silicon-rich technology combined with calcium for dentin hypersensitivity management in molar incisor hypomineralization
1 MSc, Private practice of Pediatric Dentistry, Universidade Federal de São Paulo, Rua Joaquim Floriano, 466 - cj 1012, Itaim Bibi, São Paulo 04534-002, Brazil
2 PhD, Graduate Program in Pediatric Dentistry, Institute and Research Center São Leopoldo Mandic, Rua Alferes José Caetano, 1858-124 Piracicaba, São Paulo 13400126, Brazil
Address correspondence to:
Kelly Maria Silva Moreira
Rua Alferes José Caetano, 1858-124 Piracicaba, São Paulo 13400126,
Brazil
Message to Corresponding Author
Article ID: 101485Z01FG2024
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Gorini FV, Moreira KMS. Silicon-rich technology combined with calcium for dentin hypersensitivity management in molar incisor hypomineralization. Int J Case Rep Images 2024;15(2):131–134.ABSTRACT
No abstract
Keywords: Dentin hypersensitivity, Molar incisor hypomineralization, Regeneration, Silicon, Tooth demineralization
To the Editor
In daily clinical practice, molar incisor hypomineralization (MIH) is currently present, being a challenge for dental professionals. Molar incisor hypomineralization is defined as a developmental disorder of dental enamel compromising the structure, aesthetics, and shape of the tooth. Additionally, MIH-affected teeth may present dentin hypersensitivity (DH), which may have a negative impact on a patient’s quality of life [1]. There are many proposals for managing MIH, but without a standard protocol. Among the treatments for MIH, the use of fluoride has proven important in preventing cavities and somewhat contributing to the management of hypersensitivity. However, fluoride (F) is limited in its ability to incorporate minerals into structures affected by MIH [1]. A possible reason could be associated with the action of F ions on dental structures. F ions could substitute hydroxyl ions (OH) in the hydroxyapatite—Ca10(PO4)6(OH)2, and this substitution tends to reinforce the pre-existing hydroxyapatite structure (less solubility) [2],[3]. On the other hand, the exploration of substitution in phosphate ions (PO4), also known as the site of bioactivity by silicon-containing compounds, has gained acceptance in recent decades [3],[4],[5],[6],[7],[8],[9],[10],[11] and could be particularly helpful in the management of MIH [3],[7]. Bioactive compounds containing silicon can nucleate calcium and phosphate resulting in the formation of new biomimetic surface apatite layers [3],[4],[5],[6],[7],[8],[9],[10].
A new silicon-dependent technology associated with toothpaste, known as REFIX, has proven effective in forming silicon-enriched hydroxyapatite in dental structures (enamel and dentin) under adverse conditions, such as in an acidified environment, during remineralization processes [4],[5],[6],[7],[8],[11]. Also, according to Athanasiadou et al., the association of REFIX toothpaste and the regenerating calcium booster gel could accelerate the process of mineral deposition compared to the others silicon-based technologies [7]. This mineral built by REFIX on teeth exhibits regenerative/protective properties against mineral loss [3],[4],[5],[11] and potentially improving the treatment of DH [3],[6],[7],[8]. However, not yet tested for reducing DH due to MIH.
We report a DH remission in patients with MIH who underwent a prophylactic protocol with a combination of REFIX silicon-based dentifrice and calcium booster called REFIX BOOSTER System—Dentalclean US LLC, USA (Si/Ca protocol) [6],[7],[8]. This system comprising two dental gels—Crystallizer silica/phosphate gel—gray color and Accelerator calcium gel—white color (Figure 1). This article is considered no experimental study on humans since the products are FDA approved. Besides all the ethical precepts were complied.
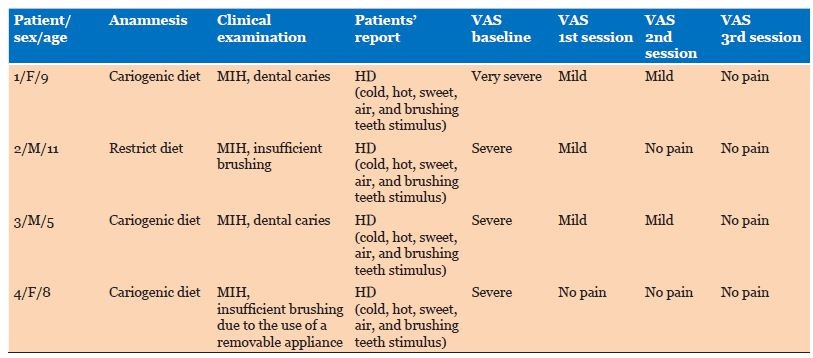
Patients with MIH were included in this study since the main complaint reported was DH. To assess the severity of DH, three-way tip to blow the patient’s teeth with MIH and a visual analogue pain scale (VAS) was used as previously described [12]. After the patient’s guardians signed the dental record and informed consents, which was used to inform and consent to the right to access information, the patients underwent an anamnesis and clinical examination, and MIH was observed. The Si/Ca protocol was carried out after the patients and their guardians received instructions on treatment both in the dental clinic office and at home (Figure 1).
The Si/Ca protocol includes the following: Step 1: A dappen dish was filled with equal amounts of crystallizer gel and accelerator gel; Step 2: After mixing the dental gels during 15 seconds, apply the mixture to the teeth surface and wait 1 minute to begin the reaction on the tooth surface; Step 3: To promote dental cleaning, a soft prophy brush in slow rotation with mixed gels was used; Step 4: The patients were instructed to brush their teeth three times a day at home, applying small amounts of both dental gels directly to the toothbrush.
Each patient was instructed to attend three clinical sessions for treatment and follow-up with an interval of one week between the first and second session and three weeks between the second and third session.
Table 1 illustrates anamnesis, clinical examination, and patient reports before and after treatment. A pattern of carious lesions associated with insufficient brushing, as well as HD with cold, hot, sweet, air, and brushing teeth stimulus, was found in this study. A rapid and significant relief of hypersensitivity was also observed from the first session of the protocol application for all patients.
Molar incisor hypomineralization, a qualitative developmental enamel defect, has received increasing attention in recent years, with a prevalence of 13% worldwide [13]. The current fluoride-dependent technologies have failed to incorporate minerals into the affected structure. Also, patients with MIH frequently present sensitive teeth, one of its most common consequences, even if their enamel is intact [1],[14]. In this study the Si/Ca protocol has been shown to be effective in reducing DH. This outcome is in line with literature that reported decrease in DH after using the REFIX Si/Ca protocol [7],[8]. REFIX dental technology is an acidified bioactive complex made from silica and phosphates. When in contact with dental tissues induced the formation of silicon-rich hydroxyapatite layers [3],[5],[7],[11]. These newly formed minerals regenerate and reinforce demineralized dental structures [3],[4],[5],[7]. Since the patients reported immediate pain relief after Si/Ca protocol, it was assumed that the structural integrity of the MIH affected teeth has been significantly restored, with consequent reduction of DH.
Molar incisor hypomineralization-affected teeth are known for the imperfect formation of apatite crystals, resulting in incomplete or deficient formation of the tooth enamel structure [1]. Thus, the treatment to be employed on teeth affected by MIH should be based on the choice of materials with biomimetic characteristics. In clinical dentistry, biomimetics refers to the repair of affected dentition by mimicking the characteristics of a natural tooth in terms of appearance, biomechanical properties, and functional abilities [2],[3],[11]. In this sense, silicon-based technologies have demonstrated the ability to form a protective mineral shield over dentin, also known as an enamel-like layer, which is capable of obliterating dentin tubules and protecting the teeth [3],[4],[5],[7].
Molar incisor hypomineralization hypersensitivity can cause substantial discomfort, difficulty in the consumption of cold or hot food or drink, as well as inadequate oral hygiene, which may increase the risk of caries, and limitations to daily life [1],[14],[15]. The teeth with the MIH tend to reveal more tooth sensitivity than healthy teeth. Conditions such as having MIH and tooth sensitivity might have a negative impact on the oral health-related quality of life. In addition, more sensitivity to the stimulus was observed in the teeth with lower tooth maturity status and dental age [15]. In this setting, the young age of many patients may complicate dental treatment. The use of the Si/Ca protocol improved the patient’s clinical and emotional condition since pain was no longer reported.
The treatment of MIH emphasizes the need for more awareness and effective preventive actions, addressing the lack of clear guidelines. Some therapies are recommended for the treatment of hypersensitivity, such photobiomodulation, glass ionomer sealant, bioactive materials, and even pulp therapy [1]. However, mainly minimally invasive treatments have been studied for this purpose. An assertive decision should be based on bioactive materials [1], since these materials can form new mineral compounds containing hydroxyapatite in dental structures [3],[4],[5],[7],[9],[10],[11]. In this regard, the new Si/Ca protocol could be included in the guidelines for MIH-related hypersensitivity. Although the study is a report of 4 unique cases, which may be a limitation of the study, it is the first study in which this protocol was tested for reducing DH due to MIH. The application of cutting-edge bioactive materials for dental regeneration using silicon-based technologies for oral health care demonstrated highly promising outcomes since a pattern of rapid reduction in DH in MIH was observed after the use of the prophylactic Si/Ca protocol in all patients.
Finally, although promising results were found, the number of participants is a limitation of this study. Long-term randomized clinical studies are indicated to evaluate the effectiveness of the prophylactic Si/Ca protocol in reducing sensitivity in patients with MIH and consequently dental mineralization. Silicon bioactive material for dental regeneration seems to reduce the MIH hypersensitivity since the patients no longer reported pain after treatment.

REFERENCES
1.
Inchingolo AM, Inchingolo AD, Viapiano F, et al. Treatment approaches to molar incisor hypomineralization: A systematic review. J Clin Med 2023;12(22):7194. [CrossRef]
[Pubmed]

2.
Zhang OL, Niu JY, Yin IX, Yu OY, Mei ML, Chu CH. Bioactive materials for caries management: A literature review. Dent J (Basel) 2023;11(3):59.
[Pubmed]
3.
Sampaio FC, Oliveira AFBd, Fernandes NLS, et al. Silicon-, silica-, and silicate-toothpastes for remineralization and repair of teeth: A scoping review. Oral 2024;4(4):467–86. [CrossRef]
4.
Vilhena FV, Lonni AASG, D’Alpino PHP. Silicon-enriched hydroxyapatite formed induced by REFIX-based toothpaste on the enamel surface. Braz Dent Sci 2021;24(4 Suppl 1):1–7. [CrossRef]
5.
Vilhena FV, Grecco SDS, González AHM, D'Alpino PHP. Regenerative and protective effects on dental tissues of a fluoride-silicon-rich toothpaste associated with a calcium booster: An in vitro study. Dent J (Basel) 2023;11(6):153. [CrossRef]
[Pubmed]
6.
Reis ALM, dos Reis MC, Mazzola T, da Cruz Pegoraro JV, de Lima DC, Fernandes LA. A novel clinical protocol for dentin hypersensitivity management based on regenerative dental gel associated with calcium: A case study in a patient with periodontal disease. Int J Case Rep Images 2023;14(1):70–4. [CrossRef]
7.
Athanasiadou D, Eymael D, Hajhamid B, Carneiro KMM, Prakki A. Chemical and ultrastructural characterization of dentin treated with remineralizing dentifrices. J Funct Biomater 2024;15(1):25. [CrossRef]
[Pubmed]
8.
Alonso RCB, de Oliveira L, Silva JAB, et al. Effectiveness of bioactive toothpastes against dentin hypersensitivity using evaporative and tactile analyses: A randomized clinical trial. Oral 2024;4(1):36–49. [CrossRef]
9.
Gibson IR, Best SM, Bonfield W. Chemical characterization of silicon-substituted hydroxyapatite. J Biomed Mater Res 1999;44(4):422–8. [CrossRef]
[Pubmed]
10.
Patel N, Best SM, Bonfield W, Gibson IR, Hing KA, Damien E, Revell PA. A comparative study on the in vivo behavior of hydroxyapatite and silicon substituted hydroxyapatite granules. J Mater Sci Mater Med 2002;13(12):1199–206. [CrossRef]
[Pubmed]
11.
Singer L, Fouda A, Bourauel C. Biomimetic approaches and materials in restorative and regenerative dentistry: Review article. BMC Oral Health 2023;23(1):105. [CrossRef]
[Pubmed]
12.
Cardoso M, Moreira KMS, Cardoso AA, Rontani RMP. CPP-ACP complex as an alternative to treatment of incisor molar hypomineralization: Case report. RGO, Rev Gaúch Odontol 2019;67.
13.
Shields S, Chen T, Crombie F, Manton DJ, Silva M. The impact of molar incisor hypomineralisation on children and adolescents: A narrative review. Healthcare (Basel) 2024;12(3):370. [CrossRef]
[Pubmed]
14.
Gevert MV, Wambier LM, Ito LY, Feltrin de Souza J, Chibinski ACR. Which are the clinical consequences of molar incisor hypomineralization (MIH) in children and adolescents? Systematic review and meta-analysis. Clin Oral Investig 2024;28(7):415. [CrossRef]
[Pubmed]
15.
Kisacik S, Ozler CO, Olmez S. Molar incisor hypomineralization and oral health-related quality of life: A sample of 8–12-years-old children. Clin Oral Investig 2024;28(1):105. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Fernanda Valone Gorini - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Kelly Maria Silva Moreira - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2024 Fernanda Valone Gorini et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}