 |
Case Report
Veno-arterial extracorporeal membrane oxygenation under dual antiplatelet therapy, immediately after craniotomy
1 Tokyo Metropolitan Police Hospital, 4-22-1 Nakano, Nakanoku, Tokyo, Japan
Address correspondence to:
Hiroshi Shimizu
Tokyo Metropolitan Police Hospital, 4-22-1 Nakano, Nakanoku, Tokyo,
Japan
Message to Corresponding Author
Article ID: 101483Z01HS2024
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Shimizu H, Fukunaga Y, Komatsu Y, Yamashita T, Imamura T, Kanai M. Veno-arterial extracorporeal membrane oxygenation under dual antiplatelet therapy, immediately after craniotomy. Int J Case Rep Images 2024;15(2):121–125.ABSTRACT
Introduction: Extracorporeal membrane oxygenation (ECMO) is often considered a relative contraindication for traumatic brain injury and cerebral hemorrhage because fatal intracranial hemorrhage can occur. Moreover, dual antiplatelet therapy (DAPT)-related cerebral hemorrhage is associated with a high mortality rate. Herein, we report a case in which the patient was placed on ECMO under DAPT and managed without anticoagulation immediately after craniotomy.
Case Report: A 51-year-old man was hospitalized for surgery for Moyamoya disease. The surgery was performed as scheduled; however, the patient experienced cardiac arrest while awakening from anesthesia. After return of spontaneous circulation, during the emergency percutaneous coronary intervention (PCI), he was placed on ECMO for cardiac arrest which caused an electrical storm. Because computed tomography (CT) after PCI revealed a new cerebral hemorrhage, ECMO was managed with DAPT without anticoagulation. Subsequently, the CT showed no increase in hematoma; however, a thrombus was observed in the membrane of the ECMO, and ECMO was withdrawn on the 4th intensive care unit day.
Conclusion: Anticoagulation therapy with or without DAPT should not be used because of the risk of bleeding associated with veno-arterial ECMO immediately after craniotomy. Additionally, the risk of thrombosis may be high; therefore, additional care must be taken, and it is necessary to manage the ECMO circuit to consider the possibility of early replacement it too.
Keywords: Craniotomy, DAPT, ECMO, Intracranial hemorrhage
Introduction
Extracorporeal membrane oxygenation (ECMO) is used in the critical care of patients with cardiac arrest. During ECMO, oxygenator thrombosis can occur in approximately 10–16% of patients, depending on the circuit type and the patient’s age [1],[2]. Therefore, anticoagulation therapy is recommended to prevent thrombosis [3]. On the other hand, bleeding is known to be a complication during ECMO, and is reported to occur in 30–50% cases [4],[5]. The rate of cerebral hemorrhage is low (2–6%) [5],[6]. However, the mortality rate of patients with central nervous system disorders is high, especially cerebral hemorrhage, which accounts for approximately 80% [7]. Therefore, ECMO is often considered a relative contraindication for traumatic brain injury and cerebral hemorrhage.
On the other hand, DAPT is typically continued after percutaneous coronary intervention (PCI) to prevent stent thrombosis. However, DAPT-related cerebral hemorrhage is associated with a high mortality rate [8]. Furthermore, the addition of anticoagulation therapy to DAPT has been reported to increase the risk of intracranial hemorrhage [9].
We report a case in which the patient was placed on ECMO under DAPT and managed without anticoagulation, immediately after craniotomy.
Case Report
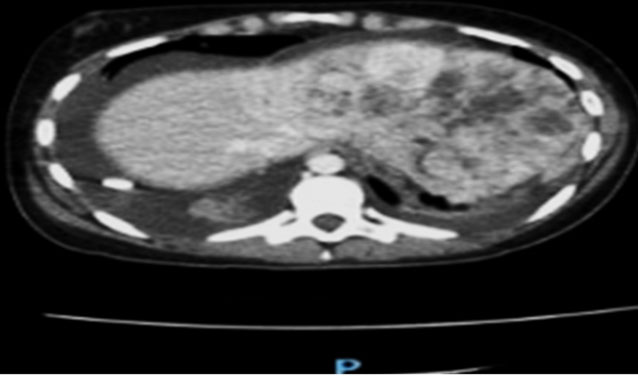
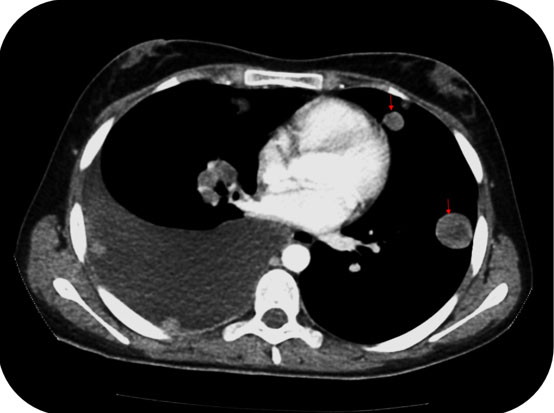
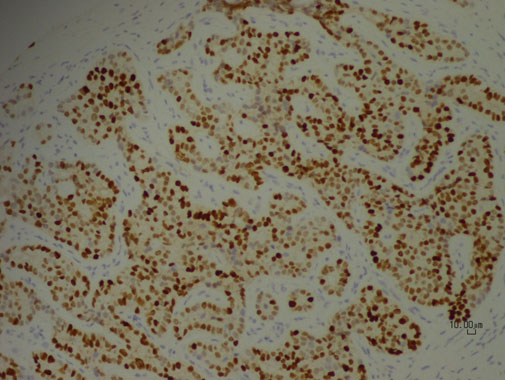
A 51-year-old man was hospitalized for surgery for Moyamoya disease. He had been hospitalized for bilateral frontal lobe cerebral infarction due to Moyamoya disease one year previously and had undergone a left superficial temporal artery to middle cerebral artery (STA-MCA) bypass for Moyamoya disease six months previously. Surgery was scheduled for a right STA-MCA bypass. There were no particular abnormalities in the previous surgery, and no abnormalities were noted on the preoperative electrocardiogram or echocardiogram. On admission, his height and weight were 175 cm and 99 kg, respectively, and body mass index (BMI) was 32.3. The laboratory test results revealed no abnormalities. The surgery was performed as scheduled; however, while awakening from anesthesia, ST-segment depression was observed on induction. Subsequently, the blood pressure decreased and the patient entered a state of pulseless electrical activity. Cardiopulmonary resuscitation was immediately performed, and the return of spontaneous circulation took 25 min. Emergency coronary angiography showed 75% stenosis in the left main coronary trunk (LMT) and 90% stenosis in #2 of right coronary artery (RCA); overall vasospastic changes were observed. Myocardial ischemia is thought to be caused by a combination of severe coronary stenosis and vasospasm. Subsequently, he was placed on ECMO for cardiac arrest, which caused an electrical storm. Subsequently, aspirin 100 mg and prasugrel 20 mg were administered orally, and PCI was performed for the LMT. After PCI, defibrillation was performed to restore the sinus rhythm. A total of 5000 units of heparin were injected during PCI with a final activated clotting time of 256 s, and laboratory tests showed a fibrinogen level of 177 mg/dL. The computed tomography (CT) after the PCI revealed a new cerebral hemorrhage (Figure 1). After consulting with neurosurgeons and cardiology departments, ECMO was managed with aspirin 10 mg and clopidogrel 75 mg without heparin, and cerebral hemorrhage was followed up with CT imaging. After admission to the intensive care unit (ICU), 6 units of fresh frozen plasma (FFP) were transfused, and 12 h later, a follow-up CT showed an increase in hematoma and midline shift; therefore, an emergency decompressive craniotomy was performed (Figure 2). In addition, 12 units of FFP were transfused both intraoperatively and postoperatively. Follow-up CT showed no increase in the hematoma (Figure 3); however, a thrombus was observed in the membrane of the ECMO, and as the hemodynamics became stable, ECMO was thus withdrawn on the 4th ICU day.
As his consciousness was impaired, a tracheostomy was performed on the 10th ICU day. The ventilator was weaned off on the 12th ICU day, and he was transferred to the general ward on the 14th ICU day. He currently has a Cerebral Performance Category score of 3 and is undergoing rehabilitation in a general ward.
Discussion
In this study, two important clinical issues were encountered. One refers to the use of ECMO in situations where there is a risk of cerebral hemorrhage after craniotomy, and the other is ECMO management performed under DAPT without heparin.
First, there are few reports of a patient being placed on ECMO immediately after or during craniotomy. However, there have been several reports on the use of ECMO for multiple injuries complicated by traumatic brain injury, including intracranial hemorrhage. In one report, 13 patients with traumatic brain injury were placed on ECMO; however, none showed exacerbation of intracranial hemorrhage on CT [10]. In another report, three patients with traumatic brain injury complicated by acute respiratory distress syndrome were placed on ECMO; however, there were no bleeding complications [11]. Thus, ECMO may not increase the risk of bleeding even in the presence of brain injury, including intracranial hemorrhage. A previous study reported that 61.9% of patients with traumatic brain injury who were treated with ECMO were discharged alive [12]. The risk of bleeding may not be high even after craniotomy, because ECMO for intracranial hemorrhage does not increase the risk of bleeding. However, many of these ECMO procedures involve veno-venous (VV)-ECMO for trauma-associated respiratory failure. There is a difference in the bleeding risk between VV-ECMO and veno-arterial (VA)-ECMO, and the risk of bleeding and serious bleeding has been reported to be higher with VA-ECMO than with VV-ECMO [6],[13],[14]. This patient also showed an increase in hematoma after being placed on ECMO, and craniotomy was performed to remove the hematoma. Therefore, there remains a concern about the bleeding risk associated with VA-ECMO immediately after craniotomy.
Second, there are several reports on the bleeding risk associated with DAPT and anticoagulation therapy with VA-ECMO. The rate of bleeding during ECMO with anticoagulation is reported to be 30–50% [4],[5] and that without anticoagulation is reported to be 32.8%. Thus, there is little difference in the rate of bleeding [15]. In addition to anticoagulation, the high bleeding risk under ECMO can be attributed to multiple treatment-related factors associated with ECMO, including the ECMO circuit and pump itself, impairing multiple innate primary and secondary hemostatic mechanisms. However, the rate of cerebral hemorrhage alone was 0.5%, which is lower than that reported previously [15]. Therefore, anticoagulation therapy is not preferred if there is a risk of cerebral hemorrhage. Regarding the bleeding risk of DAPT, DAPT and anticoagulation were reported to be more likely to cause bleeding than anticoagulation alone; however, the difference was not statistically significant [16]. Additionally, DAPT should be continued because anticoagulation therapy alone is ineffective in preventing stent thrombosis. Based on these concerns, it is desirable to avoid anticoagulation, at least judging that there is a risk of bleeding when placed on ECMO in combination with DAPT after craniotomy, as reported in this case.
However, the risk of thrombosis may increase without anticoagulation therapy during ECMO. In this case, the thrombosis formed early in the ECMO circuit. However, the rate of thrombosis during ECMO even without anticoagulation was 13.4%, which is within the range reported by previous studies that used systemic anticoagulation due to the coating of the ECMO circuit and the improvement of the oxygenator [15]. In this case, the cerebral hemorrhage tended to increase and the fibrinogen level was low; therefore, a large amount of FFP was transfused during ECMO. Therefore, it is thought that the thrombosis formed early in the ECMO circuit.
We administered ECMO under extraordinary circumstances. Although it is difficult to generalize the management in such situations, it will serve as a guide for similar situations in the future. In addition, it can also be useful as a reference when an intracranial hematoma is detected during VA-ECMO and a craniotomy is performed.
Conclusion
In conclusion, we report a case in which the patient was placed on ECMO under DAPT and managed without anticoagulation immediately after craniotomy. As there remains a concern about the bleeding risk of VA-ECMO immediately after craniotomy, it is advisable to not use anticoagulation with or without DAPT. In addition, the risk of thrombosis may be high, especially when receiving blood transfusions; therefore, care must be taken, and it is necessary to manage the ECMO circuit to consider the possibility of early replacement it too.
REFERENCES
1.
Paden ML, Conrad SA, Rycus PT, Thiagarajan RR; ELSO Registry. Extracorporeal life support organization registry report 2012. ASAIO J 2013;59(3):202–10. [CrossRef]
[Pubmed]

2.
Lubnow M, Philipp A, Foltan M, et al. Technical complications during veno-venous extracorporeal membrane oxygenation and their relevance predicting a system-exchange – Retrospective analysis of 265 cases. PLoS One 2014;9(12):e112316. [CrossRef]
[Pubmed]
3.
McMichael ABV, Ryerson LM, Ratano D, Fan E, Faraoni D, Annich GM. 2021 ELSO adult and pediatric anticoagulation guidelines. ASAIO J 2022;68(3):303–10. [CrossRef]
[Pubmed]
4.
Sklar MC, Sy E, Lequier L, Fan E, Kanji HD. Anticoagulation practices during venovenous extracorporeal membrane oxygenation for respiratory failure. A systematic review. Ann Am Thorac Soc 2016;13(12):2242–50. [CrossRef]
[Pubmed]
5.
Mazzeffi M, Greenwood J, Tanaka K, et al. Bleeding, transfusion, and mortality on extracorporeal life support: ECLS working group on thrombosis and hemostasis. Ann Thorac Surg 2016;101(2):682–9. [CrossRef]
[Pubmed]
6.
Thiagarajan RR, Barbaro RP, Rycus PT, et al. Extracorporeal life support organization registry International Report 2016. ASAIO J 2017;63(1):60–7. [CrossRef]
[Pubmed]
7.
Lorusso R, Gelsomino S, Parise O, et al. Neurologic injury in adults supported with veno-venous extracorporeal membrane oxygenation for respiratory failure: Findings from the extracorporeal life support organization database. Crit Care Med 2017;45(8):1389–97. [CrossRef]
[Pubmed]
8.
Cordonnier C, Demchuk A, Ziai W, Anderson CS. Intracerebral haemorrhage: Current approaches to acute management. Lancet 2018;392(10154):1257–68. [CrossRef]
[Pubmed]
9.
Hansen ML, Sørensen R, Clausen MT, et al. Risk of bleeding with single, dual, or triple therapy with warfarin, aspirin, and clopidogrel in patients with atrial fibrillation. Arch Intern Med 2010;170(16):1433–41. [CrossRef]
[Pubmed]
10.
Parker BM, Menaker J, Berry CD, et al. Single center experience with veno-venous extracorporeal membrane oxygenation in patients with traumatic brain injury. Am Surg 2021;87(6):949–53. [CrossRef]
[Pubmed]
11.
Muellenbach RM, Kredel M, Kunze E, et al. Prolonged heparin-free extracorporeal membrane oxygenation in multiple injured acute respiratory distress syndrome patients with traumatic brain injury. J Trauma Acute Care Surg 2012;72(5):1444–7. [CrossRef]
[Pubmed]
12.
Mader MMD, Lefering R, Westphal M, Maegele M, Czorlich P. Extracorporeal membrane oxygenation in traumatic brain injury – A retrospective, multicenter cohort study. Injury 2023;54(5):1271–7. [CrossRef]
[Pubmed]
13.
Vaquer S, de Haro C, Peruga P, Oliva JC, Artigas A. Systematic review and meta-analysis of complications and mortality of veno-venous extracorporeal membrane oxygenation for refractory acute respiratory distress syndrome. Ann Intensive Care 2017;7(1):51. [CrossRef]
[Pubmed]
14.
Zangrillo A, Landoni G, Biondi-Zoccai G, et al. A meta-analysis of complications and mortality of extracorporeal membrane oxygenation. Crit Care Resusc 201315(3):172–8.
[Pubmed]
15.
Olson SR, Murphree CR, Zonies D, et al. Thrombosis and bleeding in extracorporeal membrane oxygenation (ECMO) without anticoagulation: A systematic review. ASAIO J 2021;67(3):290–6. [CrossRef]
[Pubmed]
16.
Staudacher DL, Biever PM, Benk C, Ahrens I, Bode C, Wengenmayer T. Dual antiplatelet therapy (DAPT) versus no antiplatelet therapy and incidence of major bleeding in patients on venoarterial extracorporeal membrane oxygenation. PLoS One 2016;11(7):e0159973. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Acknowledgments
We would like to thank Editage for English language editing.
Author ContributionsHiroshi Shimizu - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Yu Fukunaga - Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Yumi Komatsu - Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Tatsuya Yamashita - Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Tomonori Imamura - Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Masayuki Kanai - Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2024 Hiroshi Shimizu et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}