 |
Case Report
Utilization of triple phase nuclear medicine bone scan for diagnosis of extradigital glomus tumors
1 MS4 Student, Indiana University School of Medicine, Fort Wayne, IN, USA
2 IU Health Orthopaedic Surgery, Fort Wayne, IN, USA
Address correspondence to:
Jay Fiechter
BS, 13785 Alicante Way, Fort Wayne, IN 46845,
USA
Message to Corresponding Author
Article ID: 101454Z01JF2024
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Fiechter J, Noyes M. Utilization of triple phase nuclear medicine bone scan for diagnosis of extradigital glomus tumors. Int J Case Rep Images 2024;15(1):95–98.ABSTRACT
Introduction: Presentations of glomus tumors in atypical areas have been documented and often lack the classic symptoms typically associated with glomus tumors. Diagnosis of extradigital glomus tumors is difficult and often comes after years of misdiagnosis.
Case Report: We present the case of an 82-year-old male with an extradigital glomus tumor at the tip of the olecranon. Gold standard magnetic resonance imaging (MRI) was negative and 3-phase nuclear medicine scan identified uptake near the olecranon process. Glomus tumor diagnosis was confirmed after pathology results. At two weeks post-op, the patient reported complete resolution of the pain. At the final follow-up, the patient had returned to all functional activities without pain and his strength was symmetric to the contralateral side.
Conclusion: This case demonstrates the importance of clinical suspicion in the workup and diagnosis of an atypical extradigital glomus tumor and how nuclear medicine scans can provide additional information in the presence of negative MRI.
Keywords: Elbow, Glomus tumor, Nuclear medicine scan
Introduction
Glomus tumors account for 1.5–4.5% of benign soft tissue tumors [1]. These tumors are benign neoplasms of the glomus apparatus typically located in the subcutaneous tissue. Quintessential glomus tumors present in the hands but they can less often present extradigitally. One review found a prevalence of such glomus tumors in extradigital areas between 11% and 65% [2]. Of these extradigital tumors, one study found a prevalence of glomus of the elbow of 4.4% [1],[2],[3]. We present a case report of a glomus tumor of the elbow at the tip of the olecranon process. This specific tumor was not identified by the gold standard magnetic resonance imaging (MRI) and a nuclear medicine scan assisted in making the final diagnosis.
Case Report
An 82-year-old male presented to the senior author for a second opinion with persistent elbow pain for more than two years that developed of insidious onset. Three months prior, he underwent an ulnar nerve decompression which failed to relieve his symptoms. Radiographs of the right elbow demonstrated mild osteoarthritis and disuse osteopenia (Figure 1).
Physical exam identified hypersensitivity and extreme pain over the right elbow just over the tip of the olecranon. There was no change in skin pigmentation or palpable nodule. The patient rated the pain as a 10/10 when the elbow was even lightly touched. Magnetic resonance imaging (MRI) without intravenous (IV) contrast of the right elbow was obtained and was negative for fracture or complete ligament/tendon complete tear. Small partial tears of the common flexor and extensor tendon were noted (Figure 2).
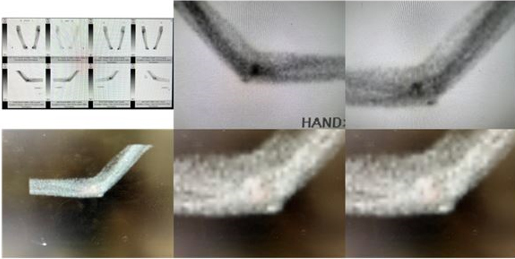
Three weeks after initial presentation to the senior author, 1 cc of triamcinolone and 1 cc of 1% lidocaine was injected at the tip of the olecranon for both diagnostic and therapeutic purposes. This provided only a few days of pain relief. A 3-phase nuclear medicine bone scan was then ordered. The radiologist interpretation from the 3-phase bone scan reported mild uptake in the radiocapitellar joint consistent with arthritis. The senior author’s interpretation of the nuclear scan identified uptake at the olecranon process which correlated clinically to the location of the patient’s pain (Figure 3).
After a lengthy discussion with patient and family discussing treatment options, they elected to proceed with surgery. During the procedure, a yellow-brownish soft tissue mass was excised and sent to pathology. Histology was consistent with a glomus tumor. At two weeks post-op, the patient reported complete resolution of the pain that had been present for two years. At the 2-month follow-up, the patient had no pain, full range of motion, and triceps strength symmetric with the contralateral side.


Discussion
Glomus tumors have been well described and documented in the literature. Wood first described each of 8 lesions in 1812 as a “painful subcutaneous tubercle” [2]. The term “glomus tumor” was then coined in 1924 by Masson [4]. Since the founding work of these two scholars, numerous cases have been reported. The classic triad for a glomus tumor is pain, cold sensitivity, and point tenderness [2],[5]. They are classically bluish purple on examination, can have bluish purple presentation on the skin, and can often be palpated as an encapsulated nodule [6],[7]. Diagnosis and workup was well described by Tang et al. by first noticing the classic triad, performing 3 common physical exam tests, and lastly confirming with an MRI or ultrasound [8]. The three tests described are Love’s Pin test, Hildreth’s test, and a cold sensitivity test. Love’s pin test involves pressing on the painful site with the head of a pin or tip of a paper clip: extreme pain is a positive test. Hildreth’s test is described by the Journal of Hand Surgery as a reliable clinical sign for diagnosis of glomus tumors. It involves using a tourniquet to artificially produce ischemia to the painful area. Reduction or absence of pain is a positive finding [9]. Lastly, ice or commonly ethyl chloride can be applied over the area of pain. Extreme pain on exposure to cold (cold sensitivity test) is a positive finding. Confirmatory MRI shows glomus tumors as hypointense on T1 and hyperintense on T2 [10].
Glomus tumors commonly present in the hands, often in the subungual region. These tumors are more easily diagnosed as they more commonly portray the classic features of glomus tumors. Extradigital glomus tumors are diagnostic anomalies, as each has a distinct set of symptoms and exam findings [11]. Our specific patient presented with pain, no palpable nodule, and no abnormal skin findings. Plain radiograph can detect glomus tumors in 25% or cases [6]. It was not surprising to have a negative finding on plain radiograph. The negative MRI was surprising after final diagnosis. In one study, MRI was found to be 100% sensitive [8], and another found it to be 90% sensitive [6]. Nuclear medicine scans are a newer imaging modality to identify glomus tumors. Two separate studies demonstrated uptake in glomus tumors using a nuclear medicine study [12],[13]. In our case, the positive uptake on the nuclear medicine assisted in decision making to surgically excise the source of uptake and was the correct treatment choice to alleviate the patient’s long-standing pain.
This patient’s delayed diagnosis and chronic pain illustrates the importance of interdisciplinary communication and collaboration. Multiple disciplines had seen this patient without successful diagnosis and treatment. Communication with orthopedics and radiology is an example of interdisciplinary collaboration that is paramount in cases with complexity such as this one.
Conclusion
Extradigital glomus tumors are a rare finding and present a diagnostic challenge. This specific glomus tumor proved to be extremely abnormal, was not identified on the gold standard MRI test, and was only detectable by a nuclear medicine scan. This case demonstrates the importance of maintaining clinical suspicion of glomus tumors and utilizing nuclear medicine scans to identify uptake to localize to the source of patient’s symptoms in the setting of atypical presentation and delay in diagnosis.
REFERENCES
1.
Anley C, Vrettos B, Roche S, Solomons M. A glomus tumour of the elbow: A case report and review of the literature. Shoulder Elbow 2014;6(1):60–2. [CrossRef]
[Pubmed]

2.
Takei TR, Nalebuff EA. Extradigital glomus tumour. J Hand Surg Br 1995;20(3):409–12. [CrossRef]
[Pubmed]
3.
Chun JS, Hong R, Kim JA. Extradigital glomus tumor: A case report. Mol Clin Oncol 2014;2(2):237–9. [CrossRef]
[Pubmed]
4.
Masson P. Le glomus neuromyo-areteriel des resions tactiles et ses tumeurs. Lyon Chir 1924;21:257–80.
5.
Beaton LE, Davis L. Glomus tumor – Reports of three cases; analysis of 271 recorded cases. Q Bull Northwest Univ Med Sch 1941;15(4):245–54.
6.
Schiefer TK, Parker WL, Anakwenze OA, Amadio PC, Inwards CY, Spinner RJ. Extradigital glomus tumors: A 20-year experience. Mayo Clin Proc 2006;81(10):1337–44. [CrossRef]
[Pubmed]
7.
Lee DW, Yang JH, Chang S, et al. Clinical and pathological characteristics of extradigital and digital glomus tumours: A retrospective comparative study. J Eur Acad Dermatol Venereol 2011;25(12):1392–7. [CrossRef]
[Pubmed]
8.
Tang CYK, Tipoe T, Fung B. Where is the lesion? Glomus tumours of the hand. Arch Plast Surg 2013;40(5):492–5. [CrossRef]
[Pubmed]
9.
Giele H. Hildreth’s test is a reliable clinical sign for the diagnosis of glomus tumours. J Hand Surg Br 2002;27(2):157–8. [CrossRef]
[Pubmed]
10.
AlNuaim B, Binsulaiman N, Alkohlani A, Al-Ghannam A, AlMohsen Z, Al-Saati M. Diagnosis of glomus tumor of the elbow: A case report. Int J Surg Case Rep 2022;90:106709. [CrossRef]
[Pubmed]
11.
Zreik N, Talbot C, Peach C. Glomus tumour of the elbow: A case of mistaken identity. Shoulder Elbow 2014;6(2):134–6. [CrossRef]
[Pubmed]
12.
Shao D, Gao Q, Wang S, Cheng Y, Wang S. 18F-FDG PET/CT of benign tracheal glomus tumor. Clin Nucl Med 2020;45(2):141–2. [CrossRef]
[Pubmed]
13.
Vangu M. 68Ga-DOTA-TATE PET/CT – Is this the holy grail of glomus tumors imaging? Journal of Nuclear Medicine 2014;55(Suppl 1):1535.
SUPPORTING INFORMATION
Author Contributions
Jay Fiechter - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Matthew Noyes - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2024 Jay Fiechter et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}