 |
Case Report
Iatrogenic bilocular femoral artery pseudoaneurysm in a patient with end-stage renal disease undergoing regular hemodialysis: An unexpected occurrence after a common procedure and surgical cure
1 MS (General Surgery), DNB, M.Ch (Plastic Surgery), DNB, MNAMS, DAFPRS, FICS, Head of Department, Department of Plastic, Craniofacial and Microsurgery, Vivekananda Polyclinic and Institute of Medical Sciences, Lucknow, Uttar Pradesh, India
2 MD (Radiodiagnosis), Assistant Professor, Department of Radiodiagnosis, Era's Lucknow Medical College and Hospital, Lucknow, Uttar Pradesh, India
3 Resident Doctor, Department of Plastic, Craniofacial and Microsurgery, Vivekananda Polyclinic and Institute of Medical Sciences, Lucknow, Uttar Pradesh, India
Address correspondence to:
Sarika Gangwar
Resident Doctor, Department of Plastic, Craniofacial and Microsurgery, Vivekananda Polyclinic and Institute of Medical Sciences, Lucknow, Uttar Pradesh,
India
Message to Corresponding Author
Article ID: 101445Z01AG2024
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Agarwal A, Chakrabarti D, Gangwar S. Iatrogenic bilocular femoral artery pseudoaneurysm in a patient with end-stage renal disease undergoing regular hemodialysis: An unexpected occurrence after a common procedure and surgical cure. Int J Case Rep Images 2024;15(1):55–60.ABSTRACT
Introduction: Pseudoaneurysms of the femoral artery can develop as an uncommon complication following penetrating trauma or arterial catheterization for cardiovascular procedures or hemodialysis. It is commonly diagnosed with color duplex imaging and usually a single pseudoaneurysm is present.
Case Report: We present a 62-year-old woman with end-stage renal disease who developed a very rare bilocular pseudoaneurysm of the femoral artery caused by inadvertent puncture of the artery during elective hemodialysis which remained uneventful and undiagnosed until the pseudoaneurysm was itself punctured by the dialysis catheter iatrogenically and another large connecting pseudoaneurysm was formed above the initial one. Typical unilocular pseudoaneurysm presents as Yin-Yang sign on color duplex imaging but here bidirectional turbulent flow was seen as double Yin-Yang sign suggestive of bilocular pseudoaneurysm mimicking the shape of a snowman, hence Yin-Yang Snowman sign. The patient presented with signs and symptoms of rapid progression of the pseudoaneurysm resulting in femoral nerve compression with compromised skin viability. Therefore, surgical management was planned and the bilocular pseudoaneurysms were excised with repair of the femoral artery and then covered with vascularized rectus femoris muscle flap.
Conclusion: An arterial pseudoaneurysm should be included in the differential diagnosis for a groin mass after femoral catheterization or other vascular procedures. A non-invasive imaging approach using color flow duplex sonography can be used with confidence and safety. But in complicated cases or cases with impending complications, surgical exploration and excision remains the mainstay of treatment.
Keywords: Bilocular pseudoaneurysm, Femoral artery pseudoaneurysm, Groin mass, Snowman Yin-Yang sign
Introduction
A pseudoaneurysm is a pulsating encapsulated hematoma in communication with a ruptured vessel. It is not bound by all 3 layers but is either contained by the media or adventitia or sometimes by only the local tissue surrounding the injured vessel [1]. The cause behind pseudoaneurysm formation is damage to arterial wall which may be due to any of the following like needle puncture, blunt injury, infectious exposure, or iatrogenically during surgical or vascular procedures [1] or as a result of poor hemostasis at the time of the initial treatment. Frequently these patients are anticoagulated or have a co-agulopathy which may compound the problem. Symptoms include pain, swelling, and bruising in the groin area and possible rupture of the pseudoaneurysm. They are a major cause for concern as they can rupture, bleed, or cause sudden death.
Case Report
The index patient was a 62-year-old woman diagnosed case of non-insulin dependent diabetes mellitus and end-stage renal disease (ESRD) from chronic glomerulonephritis. She was on regular hemodialysis twice weekly. She had been counseled earlier concerning the treatment options for ESRD and referred to the vascular surgeon for an arteriovenous (AV) fistula creation. She however declined, believing that the disease will abate over time with medications and few sessions of hemodialysis. She presented to the dialysis unit with a history of a painful mass of sudden onset in the left femoral region which developed 48 hours after the last session of hemodialysis. Pain was sharp, severe, and continuous with radiation to anterior thigh suggestive of femoral nerve compression along with reddish skin discoloration of the overlying skin and decreased movements of the left lower limb. On physical examination, a pulsatile tender mass was noted in the left femoral region, measuring 20 cm × 21 cm with differential warmth and reddish discoloration of the overlying skin (Figure 1) with fixity to underlying structures. There was a systolic bruit over the mass. All peripheral pulsations were present with normal volume. The patient was hemodynamically stable, and other systemic examination findings were unremarkable.
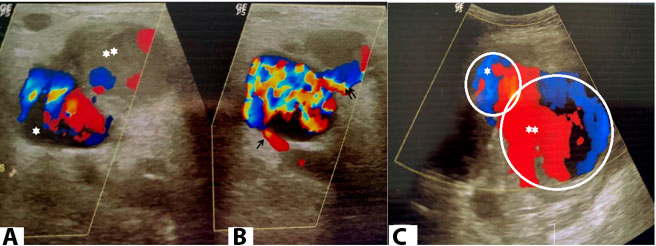
To characterize this mass better, color flow duplex sonography was done. A large bilocular cystic lesion was seen in right groin which comprised of a larger superficial locule 18×12 cm in size communicating through a short narrow neck with the deeper smaller locule of 6×3 cm size (Figure 2A). The smaller locule was seen communicating with the superficial femoral artery through a long neck (4 mm) with peak systolic flow (PSV) of blood jet of 112 cm/s (Figure 2B). The neck of the bilocular mass connecting the smaller pseudoaneurysm to the superficial femoral artery showed to and fro flow in the track with swirling flow inside the smaller locule. The flow through the narrow short interlocular neck showed PSV of 88 cm/s. Both the locules demonstrated bidirectional turbulent flow seen as double Yin-Yang sign suggestive of bilocular pseudoaneurysm (Figure 2C). This appearance mimicked the shape of a snowman on Doppler. The deep smaller aneurysm showed synchrony with cardiac cycle whereas the superficial larger aneurysm did not. The larger aneurysm also showed partial thrombosis. There was no arteriovenous (AV) fistula, retroperitoneal blood collection, or erosion of underlying structures. Other laboratory investigations including complete blood counts, liver function tests were unremarkable.
Surgical exploration was planned for excision of the pseudoaneurysms with reconstruction after routine investigations. Under regional anesthesia, left inguinal ligament was marked and a curvilinear incision extending from the left mid inguinal point traversing over the swelling and distally 15 cm proximal to the knee joint was marked. Incision was given proximal to the swelling to identify external iliac artery and vein. Further distal exploration was done to trace the common femoral artery and its superficial and deep branches. Proximal control of these vessels including the vein was taken with the vascular loops (Figure 3A). Similarly, superficial femoral artery and vein were identified and looped distal to the swelling (Figure 3B). Incision was then given over the swelling as per the marking. Subcutaneous fat was found atrophied and inflamed. Dissection was done in the subcutaneous plane to circumferentially delineate the pulsatile larger pseudoaneurysm (Figure 3C) which was fixed to the sartorius muscle laterally and gracilis muscle medially. It was dissected from the adjacent muscles except from the underlying fixed structures (Figure 3D). A smaller pseudoaneurysm was found hidden below the larger one and was connected to it with a small opening. The larger one was excised completely along with the parts of adjacent involved muscles (Figure 3E). The smaller pseudoaneurysm, dissected free from surrounding structures was found to be arising directly from the femoral artery (Figure 4A and Figure 4B). It was then excised (Figure 4C) after controlling the flow in the region with the proximal and distal vascular loops. Primary repair of the femoral artery was done with 7-0 prolene and proximal and distal controls were released to ensure blood flow through the femoral vessels with no leakage (Figure 4D). The non-viable and inflamed skin was excised. Femoral artery was then covered with rectus femoris muscle flap from the adjoining region to provide well vascularized and supple tissue over the exposed vessels to prevent blow out (Figure 4E). Hemostasis was achieved and with suction drain in place, primary closure in layers was done. Postoperatively, the patient recovered uneventfully. Drain was removed on postoperative day 4 and patient discharged on postoperative day 8. The patient was on regular follow-up twice weekly and sutures were removed on postoperative day 14 (Figure 4F).



Discussion
After catheterization, arterial injuries including femoral artery hematoma, arteriovenous fistula, or a pseudoaneurysm, are common because of high pressure flow from the punctured vessel. Femoral artery pseudoaneurysm is a rare diagnosis with 0.2–6% of reported cases following diagnostic and therapeutic procedures [2]. Out of these, it is more common in the superficial femoral artery, less commonly it can be seen in the deep and common femoral arteries, and at junction of deep and superficial femoral arteries [3]. Left femoral region was her usual site of cannulation during hemodialysis. Repeated cannulation caused arterial wall trauma resulting in pseudoaneurysm. The cause of the pseudoaneurysm in above-described case was due to the placement of a commonly used catheter for hemodialysis where the dialysis technician might have entered the catheter into the femoral artery and punctured it and a small pseudoaneurysm was formed which remained dormant and asymptomatic and uncomplicated. On subsequent dialysis, the technician punctured the pseudoaneurysm itself while gaining access which lead to formation of a bigger pseudoaneurysm superficial to the previous one and connecting with it through a small opening which gave it a bilocular shape. Apart from clinical examination, radiological evidence is also required to confirm the diagnosis of arterial pseudoaneurysm such as Doppler ultrasonography (DUS), computed tomography (CT) scan, magnetic resonance imaging (MRI), and angiography [4]. Color DUS is the gold standard for diagnosis of pseudoaneurysms of the femoral artery1 wherein bidirectional blood flow in a saccular structure is depicted by swirling motion pattern known as “Yin-Yang sign” [5]. Color Doppler is non-invasive, non-ionizing, and inexpensive as compared to CT angiography. In addition, Doppler has the advantage of real time assessment for assessing velocity and to-and-fro waveform in the communicating neck of pseudoaneurysm and demonstrating the classical Yin-Yang sign. These features are not appreciated on CT angiography. Ultrasound-guided compression can also reduce small superficial pseudoaneurysms. Computed tomography angiography is advantageous in locating the exact point of pseudoaneurysm as a presurgical workup.
However, this pattern can also be seen with a true aneurysm [4]. Kumar et al. [6] demonstrated 51 (11.5%) bilocular, 6 (1.3%) trilocular, and 3 (0.67%) tertralocular pseudoaneurysms in their experience of 444 patients. 95% were managed by manual compressions and only 5% by surgical methods. Color duplex study in our case elicited a new finding where a typical Yin-Yang sign of pseudoaneurysm was seen at the interface of femoral artery and the smaller pseudoaneurysm and an atypical Yin-Yang sign was elicited at the interface of the smaller and the larger pseudoaneurysm due to presence of thrombus in the larger pseudoaneurysm which was obstructing the typical swirling flow of blood in to and fro direction. Therefore, we suggest a new name for this rare finding which is “Yin-Yang Snowman sign.”
Treatment of the femoral arterial pseudoaneurysm becomes necessary if it produces ischemic or neuropathic signs and symptoms in the ipsilateral limb. Treatment approaches may be conservative or surgical excision. Approach for management is decided depending on the size of pseudoaneurysm. Conservative management can be considered for pseudoaneurysms with a diameter of <3 cm and volume of <6 cm3 as these may get thrombosed by themselves, however, cautious monitoring is required for those who are on anticoagulant medication [1],[7]. As much as 87–93% of pseudoaneurysms falling into this category resolve spontaneously [1]. But serial ultrasonographic monitoring should be done to confirm the resolution of pseudoaneurysm. Non-surgical treatment approaches include ultrasound-guided thrombin injection, ultrasound-guided compression, biodegradable collagen injection, coated stents, coil embolization, and use of various vascular closure devices [8]. Surgical repair in pseudoaneurysms larger than 20 mm is safe and essential [3].
Rapidly expansile mass, distal neurovascular deficits, mycotic infections, compromised soft tissue viability, and failure of percutaneous interventions are the indications for surgical treatment of femoral artery pseudoaneurysm. Signs of rapid progression with femoral nerve entrapment and compromised skin viability were present in the lady, therefore immediate surgical exploration was planned. In cases where excision of artery is also required and the vessel defect is too large to anastomose end to end, autologous or synthetic graft can be used. The great saphenous vein (GSV), the superficial femoral and popliteal veins are commonly used for autologous vein grafts [8]. We were able to achieve primary repair of the femoral artery. The exposed artery, being at risk of blow out, is to be given a vascularized muscle flap cover. Various muscle flaps that can be used to cover groin region include rectus femoris, sartorius, gracilis, rectus abdominis, and tensor fascia lata [9]. Vascularized rectus femoris muscle flap based on descending branch of lateral circumflex femoral artery was harvested in the presented case to cover the defect as it was adjacent to the defect, of appropriate size to achieve complete cover and other muscles (gracilis and sartorius) were involved by the extent of the pseudoaneurysm. Therefore, they had to be excised partially along with the pseudoaneurysm. Groin wound reconstruction option includes rectus femoris muscle flap which does not cause any functional deficit at the knee joint. The muscle flap is dependable and the donor site is not problematic, even in the presence of peripheral vascular disease [10].
Conclusion
In summary, an arterial pseudoaneurysm should be included in the differential diagnosis for a groin mass after femoral catheterization or other vascular procedures. A non-invasive imaging approach using color flow duplex sonography can be used with confidence and safety. But in complicated cases or cases with impending complications, surgical exploration and excision remains the mainstay of treatment. The type of surgery and the technique of repair would depend on the severity and extent of pseudoaneurysm.
Learning points in this study were:
(1) Bilocular pseudoaneurysm is a very rare occurrence and there should be a criteria for its diagnosis as we mentioned a “Snowman Yin-Yang” sign.
(2) This should be considered a surgical emergency due to risk of femoral artery blow out which can be life threatening.
We have formulated a treatment protocol for such cases which ensures femoral artery repair and prevention of recurrence.
Occurrence of such pseudoaneurysm can be prevented by keeping in mind following measures:
(1) After attempted cannulation or removal of cannula post hemodialysis, pressure should be applied at the site.
(2) Only skilled doctor or nursing staff should perform the procedure.
(3) Technician should confirm whether the cannula is in artery or in vein during the procedure before proceeding further
In case of any visible or palpable swelling at previous puncture site, early Doppler USG should be done to make and early diagnosis to avoid life threatening situations.
REFERENCES
1.
Lønnebakken MT, Gerdts E, Pedersen OM. Femoral pseudoaneurysm with a communicating arteriovenous fistula: A complication after percutaneous coronary intervention. Circulation 2012;126(11):e161–2. [CrossRef]
[Pubmed]

2.
Ahmad F, Turner SA, Torrie P, Gibson M. Iatrogenic femoral artery pseudoaneurysms—A review of current methods of diagnosis and treatment. Clin Radiol 2008;63(12):1310–6. [CrossRef]
[Pubmed]
3.
Lazarides MK, Arvanitis DP, Liatas AC, Dayantas JN. Iatrogenic and noniatrogenic arterial trauma: A comparative study. Eur J Surg 1991;157(1):17–20.
[Pubmed]
4.
Saad NEA, Saad WEA, Davies MG, Waldman DL, Fultz PJ, Rubens DJ. Pseudoaneurysms and the role of minimally invasive techniques in their management. Radiographics 2005;25 Suppl 1:S173–89. [CrossRef]
[Pubmed]
5.
Mahmoud MZ, Al-Saadi M, Abuderman A, et al. “To-and-fro” waveform in the diagnosis of arterial pseudoaneurysms. World J Radiol 2015;7(5):89–99. [CrossRef]
[Pubmed]
6.
Kumar V, Paul B, Sharma V, Sachdeva A, Shrivastava S. Non-surgical management of iatrogenic arterial pseudoaneurysms-ultrasound-guided manual compression, an Indian experience. Indian Heart J 2008;60(6):574–7.
[Pubmed]
7.
O'Sullivan GJ, Ray SA, Lewis JS, et al. A review of alternative approaches in the management of iatrogenic femoral pseudoaneurysms. Ann R Coll Surg Engl 1999;81(4):226–34.
[Pubmed]
8.
Bell CL, Ali AT, Brawley JG, et al. Arterial reconstruction of infected femoral artery pseudoaneurysms using superficial femoral-popliteal vein. J Am Coll Surg 2005;200(6):831–6. [CrossRef]
[Pubmed]
9.
Williams IM, Milling MAP, Shandall AA. Vascularised muscular flaps and arterial graft infection in the groin. Eur J Vasc Endovasc Surg 2003;25(5):390–5. [CrossRef]
[Pubmed]
10.
Alkon JD, Smith A, Losee JE, Illig KA, Green RM, Serletti JM. Management of complex groin wounds: Preferred use of the rectus femoris muscle flap. Plast Reconstr Surg 2005;115(3):776–83. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Amit Agarwal - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Debalina Chakrabarti - Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Sarika Gangwar - Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2024 Amit Agarwal et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}