 |
Case Report
Diagnosis of pancreatic head cancer with prominent fatty change in the pancreatic body using 3 Tesla-enhanced magnetic resonance imaging: A case report
1 Department of Gastroenterology, Kishiwada City Hospital, Osaka, Japan
2 Department of Interventional Bilio-Pancreatology, Kawasaki Medical School, Okayama, Japan
Address correspondence to:
Kyosuke Goda
Department of Gastroenterology, Kishiwada City Hospital, 1001 Gakuharatyo, Kishiwada City, Osaka Prefecture 596-8501,
Japan
Message to Corresponding Author
Article ID: 101432Z01KG2023
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Goda K, Miyake T, Sato T, Tada Y, Nakashima Y, Yoshida K. Diagnosis of pancreatic head cancer with prominent fatty change in the pancreatic body using 3 Tesla-enhanced magnetic resonance imaging: A case report. Int J Case Rep Images 2023;14(2):164–170.ABSTRACT
Introduction: Pancreatic cancer is the seventh leading cause of cancer-related deaths worldwide, and early diagnosis is necessary to obtain a favorable postoperative prognosis. Contrast-enhanced computed tomography is generally recommended when pancreatic cancer is suspected. Herein, we present a case in which contrast-enhanced magnetic resonance imaging was used to detect pancreatic cancer, while contrast-enhanced computed tomography and endoscopic ultrasonography were unable to reveal possible pancreatic cancer.
Case Report: We present a case of a man in his 70s whose diabetes had worsened, and the main pancreatic duct was dilated, with suspicion of pancreatic cancer. Contrast-enhanced computed tomography did not reveal a tumor that indicated possible pancreatic cancer, and endoscopic ultrasonography exhibited similar findings. Therefore, 3 Tesla-enhanced magnetic resonance imaging was performed to make an image diagnosis of pancreatic cancer.
Conclusion: In lesions exhibiting invasive growth accompanied by prominent fatty change in the pancreatic body, obtaining the contrast effect of adipose tissue by contrast computed tomography is difficult. In addition, an association between prominent fatty change in the pancreatic body and pancreatic cancer has been reported. Therefore, we performed 3 Tesla-enhanced magnetic resonance imaging examination, which tends to yield favorable tissue contrast on adipose tissue images.
Keywords: Fatty change, Pancreatic body, Pancreatic head cancer, 3-T enhanced magnetic resonance imaging
Introduction
Pancreatic cancer is the seventh leading cause of cancer-related deaths worldwide [1], and the cancer-related mortality rate is estimated to be 2.5 and 14.8 per 100,000 people in developing and developed countries, respectively [2]. According to the Union for International Cancer Control (UICC), the 5-year survival rate of pancreatic cancer at the T1 and IA stages is approximately 68.7% [3]. Early diagnosis is necessary to obtain a favorable postoperative prognosis for pancreatic cancer. However, pancreatic cancer is characterized by a malignant tumor that is difficult to diagnose early, with 47.4% of cases already progressing to stage IV at the time of diagnosis [4]. Among various proposed diagnostic methods, contrast-enhanced computed tomography (CT) exhibits high diagnostic ability in both sensitivity and specificity [5],[6],[7], which are reported to be 77% and 100%, respectively, even for small pancreatic tumors [8]. Contrast-enhanced magnetic resonance imaging (MRI) theoretically visualize cancer lesion at an earlier stage by providing a comprehensive analysis of the morphological changes of the pancreas parenchyma. Despite this, contrast-enhanced MRI has almost the same sensitivity and specificity as that of contrast-enhanced CT [9],[10],[11],[12]. For this reason, MRI is not widely used as the primary imaging modality due to the length and cost of imaging time and availability.
Various lifestyle habits such as cigarette smoking, high body mass index, diabetes, and chronic pancreatitis have been reported as a risk factor for pancreatic cancer [13],[14],[15],[16]. Furthermore, Emily et al. have investigated the diffuse pancreatic steatosis associated with metabolic syndrome for the risk of pancreatic cancer [17]. On the other hand, only a few case series have reported the direct relationship between focal fatty change in the pancreas and localization of pancreatic cancer [18]. In this report, we present a unique case of pancreatic head cancer which was not visible on contrast-enhanced CT due to prominent fatty change, for which 3 Tesla (3-T)-enhanced MRI was useful for diagnosis; furthermore, we also review the associated literature.
Case Report
We were presented with a male patient in his 70s whose main complaint was weight loss. The patient had a history of hypertension, diabetes, and rectal cancer; his social history included no alcohol consumption and smoking history of 20 cigarettes/day for 55 years. He also reported no allergies. The patient was being treated for diabetes by a family doctor, was administered several hypoglycemic agents, and his glycosylated hemoglobin (HbA1c) concentration (7.0%) was stable. Starting in February 2019, his HbA1c concentration rose sharply to =10.0%, and his body weight decreased by =5 kg in half a year. An abdominal echo performed by a family doctor revealed dilation of the main pancreatic duct, and pancreatic head cancer was suspected.
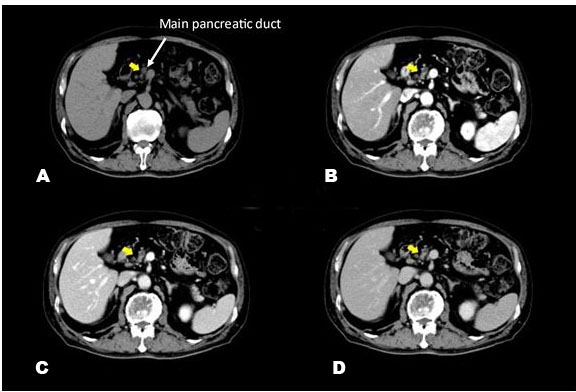
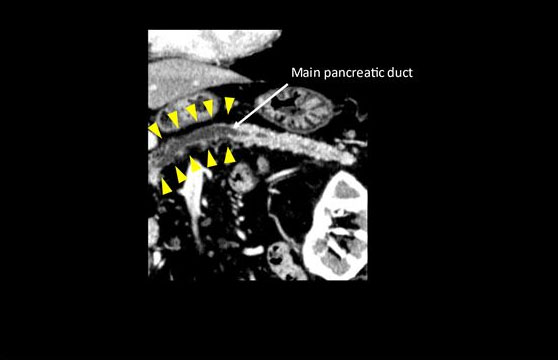
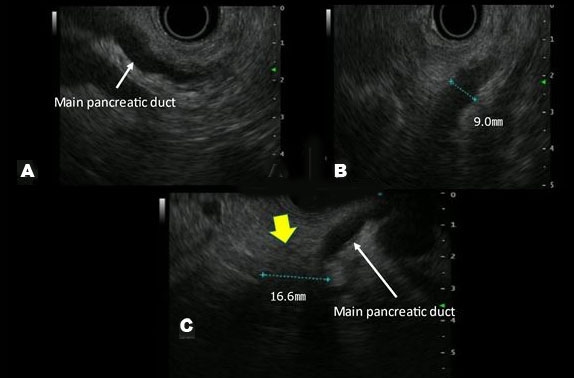
A blood test revealed increases in HbA1c and carcinoembryonic antigen to 11.2% and 8.7 ng/mL, respectively. Abdominal ultrasonography and Sonazoid® (Daiichi-Sankyo, Tokyo, Japan; GE Healthcare, Milwaukee, WI, USA) enhanced ultrasound (Figure 1) did not reveal a hypoechoic figurine indicative of pancreatic cancer on the pancreatic head side of the dilated main pancreatic duct. In the horizontal-section image of the contrast-enhanced CT arterial phase (Figure 2), a tumor suspected to be typical of pancreatic cancer that was contrasted late on the pancreatic head side of the interrupted main pancreatic duct, could not be recognized. In the coronary image (Figure 3), the pancreas was atrophied from the body to the head and there was dilation of the main pancreatic duct, revealing prominent fatty change in the pancreatic body; however, no neoplastic lesion was detectable (Figure 4). Endoscopic ultrasonography (EUS) revealed dilation of the main pancreatic duct and atrophy of the pancreas as on the abdominal ultrasonography; nevertheless, the tumor could not be clearly visualized. Therefore, histological diagnosis using endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA) was considered difficult. Hence, we decided to conduct a detailed examination using other modalities.
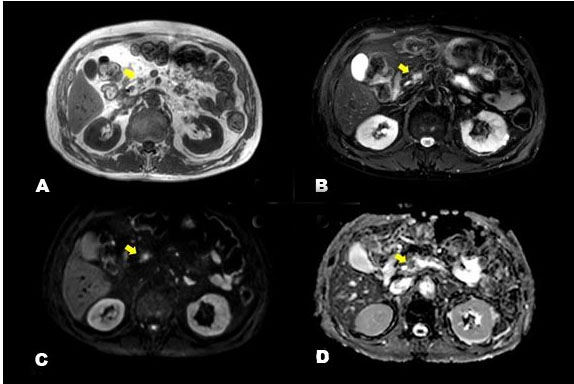
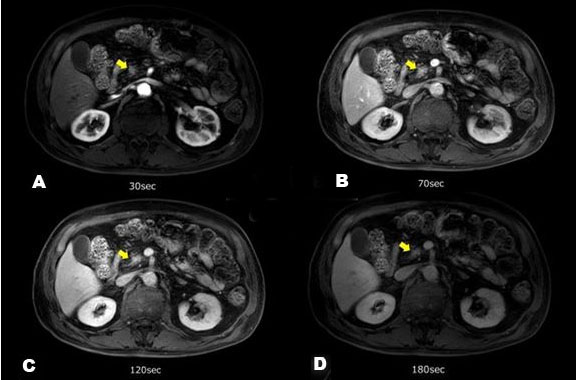
We conducted 3-T contrast-enhanced MRI which revealed a low-intensity mass of approximately 1 cm in the pancreatic head on T1-weighted images and on T2 fat suppression; it was recognized as a tumor, exhibiting clearer high-intensity than did the adipose tissue (Figure 5). In addition, the lesion showed high intensity on diffusion-weighted imaging (DWI) and low intensity on the apparent diffusion coefficient (ADC), indicating that pancreatic cancer was present in the pancreatic head. Gadolinium-enhanced MRI (Figure 6) revealed that the mass was late-enhanced, and we were able to make a definitive diagnosis of pancreatic cancer. Endoscopic retrograde pancreatography (ERP) and magnetic resonance cholangiopancreatography (MRCP) (Figure 7) confirmed disruption of the main pancreatic duct and dilation of the pancreatic duct. Serial pancreatic juice aspiration cytological examination (SPACE) was performed. After performing endoscopic nasopancreatic drainage and pancreatic duct brush cytology, pancreatic juice was collected thrice via a pancreatic catheter. Cytopathology revealed class IIIa disease (Papanicolaou classification). Based on the imaging test results, the patient was confidently diagnosed with pancreatic cancer (T1c, N0, M0, stage IA), and we decided to perform pancreaticoduodenectomy as treatment.
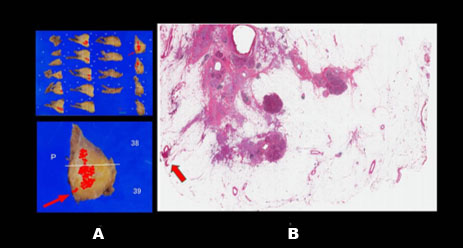
In the resected histopathological specimen (Figure 8), cancer cells had invaded the highly fatty pancreatic tissue, and posterior invasion of the pancreatic tissue was also observed. The pancreatic tumor was classified as pT2, pN1, M0, G3, R1, stage IIB according to the tumor-node-metastasis classification (UICC, 8th edition). Since the progression of pancreatic cancer was judged to be R1, which indicates that the cancer tissue could not be completely resected, we decided to perform postoperative adjuvant chemotherapy.


Discussion
Herein, we present a case of pancreatic head cancer with prominent fatty change in the pancreatic body that was difficult to diagnose. Finally, we performed definitive imaging diagnosis using 3-T enhanced MRI. Compared with that of conventional 1.5-T MRI, 3-T MRI has twice the static magnetic field strength and provides high spatial resolution; thus, its usefulness in the imaging diagnosis of pancreatic cancer has been reported [19],[20],[21]. In a study comparing the usefulness of 3-T contrast-enhanced MRI with that of multidetector computed tomography (MD-CT), no significant difference was observed between MD-CT and 3-T MRI in the sensitive and specific in diagnosing and staging pancreatic cancer respectively [9],[10],[11],[12]. Because of the sensitivity and specificity of MD-CT are already enough high [5],[6],[7],[8], it is likely difficult to find a statistically significant difference when compared with MD-CT. Nevertheless, most expert opinion shows the added utility of MRI over MD-CT in particular situations including the differentiating isoattenuating pancreatic lesions [22]. Furthermore, specific situations MRI seems to have an advantage over MD-CT in differentiating pancreatic tumors in mass-forming pancreatitis, in the presence of hypertrophied pancreatic head or focal fatty infiltration of the parenchyma [23]. In this case, 3-T contrast-enhanced MRI was clearly superior to contrast-enhanced CT in the visualization and enhancement of the lesion. In lesions that exhibit invasive growth in pancreatic tissue are highly adipose-degenerated, obtaining contrast between the adipose tissue and such lesions on contrast-enhanced CT may be difficult. In contrast, 3-T MRI examination, which can easily obtain tissue contrast with good fat suppression images, is considered more useful for diagnosing such lesions. In the authors’ experience, 3-T contrast-enhanced MRI is often used as a second-line imaging modality for a high clinical suspicion of pancreatic cancer despite none being visible on CT.
However, making a differential diagnosis between pancreatic cancer and an inflammatory mass based on imaging alone is not easy. Of the patients diagnosed with pancreatic cancer based on imaging tests alone, 10.7% had benign diseases, such as chronic pancreatitis, among those who underwent pancreaticoduodenectomy [24]. In this case, visualizing the tumor clearly using EUS was difficult; therefore, histological diagnosis using EUS-FNA was considered unreliable and difficult. SPACE has been reported to be highly useful in diagnosing pancreatic cancer [25]. Therefore, we attempted to make a definitive diagnosis using SPACE; however, the cytopathological diagnosis was class III; hence, we could not make a definitive preoperative diagnosis. Nevertheless, we believe that actively performing pancreatic cancer surgery in cases where the tumor cannot be clearly visualized is preferred, such as in this case.
In this case, prominent fatty change in the pancreatic body was observed from the pancreatic head adjacent to the lesion compared to the tail. Atrophy, fibrosis, and steatosis of the pancreas are generally recognized as some of the age-related changes [26]. Nonetheless, pancreatic cancer is potentially related to focal atrophy and fatty change in the pancreas [18],[27]. The peroxisome proliferator-activated receptor γ (PPARγ) is an intracellular transcription factor required for the differentiation and maturation of adipocytes. Peroxisome proliferator-activated receptor γ activation suppresses transforming growth factor-β, resulting in the suppression of pancreatic cancer growth [28],[29]. Kikuyama et al. proposed that PPARγ may be activated to suppress cancer progression at sites where pancreatic cancer exists, resulting in fatty transformation of the surrounding pancreatic tissue [18]. As in this case, we speculate that prominent fatty change in the pancreatic body near the tumor was caused by obstructive pancreatitis due to pancreatic duct obstruction and PPARγ activation by cancer. In recent years, a small number of case reports on focal fatty change in the pancreatic body and pancreatic cancer have surfaced [18]. A study that quantitatively evaluated pancreatic adiposity using MRI-proton density fat fraction (MRI-PDFF) found that MRI-PDFF and the histological pancreatic fat fraction were higher in pancreatic cancer cases [30]. The case findings also support the possibility of using fatty changes in pancreatic tissue as an essential imaging biomarker for the early detection of pancreatic cancer. To prove the usefulness of this key finding, it is necessary to accumulate related case reports in the future.
Conclusion
In lesions exhibiting invasive growth accompanied by prominent fatty change in the pancreatic body, obtaining the contrast effect of adipose tissue by contrast computed tomography is difficult. In addition, an association between prominent fatty change in the pancreatic body and pancreatic cancer has been reported. Therefore, we performed 3 Tesla-enhanced magnetic resonance imaging examination, which tends to yield favorable tissue contrast on adipose tissue images. To prove the usefulness of this key finding, it is necessary to accumulate related case reports in the future.
REFERENCES
1.
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018;68(6):394–424. [CrossRef]
[Pubmed]

2.
Veisani Y, Jenabi E, Khazaei S, Nematollahi S. Global incidence and mortality rates in pancreatic cancer and the association with the Human Development Index: Decomposition approach. Public Health 2018;156:87–91. [CrossRef]
[Pubmed]
3.
Egawa S, Toma H, Ohigashi H, et al. Japan Pancreatic Cancer Registry; 30th year anniversary: Japan Pancreas Society. Pancreas 2012;41(7):985–92. [CrossRef]
[Pubmed]
4.
Hospital cancer registry 2013–2014 summary of 5-year survival rate; 2021. Cancer registry center: National Cancer Center. [Available at: https://ganjoho.jp/public/qa_links/report/hosp_c/hosp_c_reg_surv/pdf/hosp_c_reg_surv_2013-2014]
5.
Yamada Y, Mori H, Matsumoto S, Kiyosue H, Hori Y, Hongo N. Pancreatic adenocarcinoma versus chronic pancreatitis: Differentiation with triple-phase helical CT. Abdom Imaging 2010;35(2):163–71. [CrossRef]
[Pubmed]
6.
Ahn SS, Kim MJ, Choi JY, Hong HS, Chung YE, Lim JS. Indicative findings of pancreatic cancer in prediagnostic CT. Eur Radiol 2009;19(10):2448–55. [CrossRef]
[Pubmed]
7.
Ishigami K, Yoshimitsu K, Irie H, et al. Diagnostic value of the delayed phase image for iso-attenuating pancreatic carcinomas in the pancreatic parenchymal phase on multidetector computed tomography. Eur J Radiol 2009;69(1):139–46. [CrossRef]
[Pubmed]
8.
Bronstein YL, Loyer EM, Kaur H, et al. Detection of small pancreatic tumors with multiphasic helical CT. AJR Am J Roentgenol 2004;182(3):619–23. [CrossRef]
[Pubmed]
9.
Treadwell JR, Zafar HM, Mitchell MD, Tipton K, Teitelbaum U, Jue J. Imaging tests for the diagnosis and staging of pancreatic adenocarcinoma: A meta-analysis. Pancreas 2016;45(6):789–95. [CrossRef]
[Pubmed]
10.
Takakura K, Sumiyama K, Munakata K, et al. Clinical usefulness of diffusion-weighted MR imaging for detection of pancreatic cancer: Comparison with enhanced multidetector-row CT. Abdom Imaging 2011;36(4):457–62. [CrossRef]
[Pubmed]
11.
Motosugi U, Ichikawa T, Morisaka H, et al. Detection of pancreatic carcinoma and liver metastases with gadoxetic acid-enhanced MR imaging: Comparison with contrast-enhanced multi-detector row CT. Radiology 2011;260(2):446–53. [CrossRef]
[Pubmed]
12.
Koelblinger C, Ba-Ssalamah A, Goetzinger P, et al. Gadobenate dimeglumine-enhanced 3.0-T MR imaging versus multiphasic 64-detector row CT: Prospective evaluation in patients suspected of having pancreatic cancer. Radiology 2011;259(3):757–66. [CrossRef]
[Pubmed]
13.
Fuchs CS, Colditz GA, Stampfer MJ, et al. A prospective study of cigarette smoking and the risk of pancreatic cancer. Arch Intern Med 1996;156(19):2255–60.
[Pubmed]
14.
Michaud DS, Giovannucci E, Willett WC, Colditz GA, Stampfer MJ, Fuchs CS. Physical activity, obesity, height, and the risk of pancreatic cancer. JAMA 2001;286(8):921–9. [CrossRef]
[Pubmed]
15.
Huxley R, Ansary-Moghaddam A, Berrington de González A, Barzi F, Woodward M. Type-II diabetes and pancreatic cancer: A meta-analysis of 36 studies. Br J Cancer 2005;92(11):2076–83. [CrossRef]
[Pubmed]
16.
Talamini G, Falconi M, Bassi C, et al. Incidence of cancer in the course of chronic pancreatitis. Am J Gastroenterol 1999;94(5):1253–60. [CrossRef]
[Pubmed]
17.
Truong E, Pandol S, Jeon C. Uniting epidemiology and experimental models: Pancreatic steatosis and pancreatic cancer. EBioMedicine 2022;79:103996. [CrossRef]
[Pubmed]
18.
Kikuyama M, Hanada K, Ueki T. Pancreatic carcinoma in situ presenting prominent fatty change of the pancreatic body on CT: Experiences from 3 cases. Suizo 2015;30(4):626–32. [CrossRef]
19.
Fusari M, Maurea S, Imbriaco M, et al. Comparison between multislice CT and MR imaging in the diagnostic evaluation of patients with pancreatic masses. Radiol Med 2010;115(3):453–66. [CrossRef]
[Pubmed]
20.
Shin SS, Armao DM, Burke LMB, et al. Comparison of the incidence of pancreatic abnormalities between high risk and control patients: Prospective pilot study with 3 Tesla MR imaging. J Magn Reson Imaging 2011;33(5):1080–5. [CrossRef]
[Pubmed]
21.
Uchida M, Uozumi J, Hayabuchi N. Clinical utility of dynamic 3T MRI for pancreatobiliary cancer. J Gastroenterol Cancer Screen 2009;47(3):357–65. [CrossRef]
22.
Sheridan MB, Ward J, Guthrie JA, et al. Dynamic contrast-enhanced MR imaging and dual-phase helical CT in the preoperative assessment of suspected pancreatic cancer: A comparative study with receiver operating characteristic analysis. AJR Am J Roentgenol 1999;173(3):583–90. [CrossRef]
[Pubmed]
23.
Fattahi R, Balci NC, Perman WH, et al. Pancreatic diffusion-weighted imaging (DWI): Comparison between mass-forming focal pancreatitis (FP), pancreatic cancer (PC), and normal pancreas. J Magn Reson Imaging 2009;29(2):350–6. [CrossRef]
[Pubmed]
24.
Abraham SC, Wilentz RE, Yeo CJ, et al. Pancreaticoduodenectomy (Whipple resections) in patients without malignancy: Are they all ‘chronic pancreatitis’? Am J Surg Pathol 2003;27(1):110–20. [CrossRef]
[Pubmed]
25.
Iiboshi T, Hanada K, Fukuda T, Yonehara S, Sasaki T, Chayama K. Value of cytodiagnosis using endoscopic nasopancreatic drainage for early diagnosis of pancreatic cancer: Establishing a new method for the early detection of pancreatic carcinoma in situ. Pancreas 2012;41(4):523–9. [CrossRef]
[Pubmed]
26.
Glaser J, Stienecker K. Pancreas and aging: A study using ultrasonography. Gerontology 2000;46(2):93–6. [CrossRef]
[Pubmed]
27.
Majumder S, Philip NA, Takahashi N, Levy MJ, Singh VP, Chari ST. Fatty pancreas: Should we be concerned? Pancreas 2017;46(10):1251–8. [CrossRef]
[Pubmed]
28.
Toyota M, Miyazaki Y, Kitamura S, et al. Peroxisome proliferator-activated receptor gamma reduces the growth rate of pancreatic cancer cells through the reduction of cyclin D1. Life Sci 2002;70(13):1565–75. [CrossRef]
[Pubmed]
29.
Lee SJ, Yang EK, Kim SG. Peroxisome proliferator-activated receptor-gamma and retinoic acid X receptor alpha represses the TGFbeta1 gene via PTEN-mediated p70 ribosomal S6 kinase-1 inhibition: Role for Zf9 dephosphorylation. Mol Pharmacol 2006;70(1):415–25. [CrossRef]
[Pubmed]
30.
Fukui H, Hori M, Fukuda Y, et al. Evaluation of fatty pancreas by proton density fat fraction using 3-T magnetic resonance imaging and its association with pancreatic cancer. Eur J Radiol 2019;118:25–31. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Kyosuke Goda - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Tomoo Miyake - Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Tatsuki Sato - Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Yamato Tada - Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Yoshihiro Nakashima - Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Koji Yoshida - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2023 Kyosuke Goda et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}