 |
Case Report
Lumbo-renal arteriovenous fistula: An unusual complication of percutaneous kidney biopsy
1 DNB (Nephrology), MD (Medicine), PD Hinduja Hospital and Medical Research Centre, Veer Savarkar Marg, Mahim, Mumbai 400016, India
Address correspondence to:
Khairwar Mahesh Prasad
Consultant Nephrology, Nephrology Department, PD Hinduja Hospital and Medical Research Centre, Veer Savarkar Marg, Mahim, Mumbai 400016,
India
Message to Corresponding Author
Article ID: 101419Z01KP2023
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Prasad KM. Lumbo-renal arteriovenous fistula: An unusual complication of percutaneous kidney biopsy. Int J Case Rep Images 2023;14(2):102–105.ABSTRACT
Arteriovenous fistula formation after percutaneous kidney biopsy is not uncommon. Most of these fistulas are intrarenal and close spontaneously. Formation of a fistula between an intercostal branch of the lumbar artery and the renal vein is a very rare complication. Our case has lumbo-renal arteriovenous fistula (AVF) following a percutaneous kidney biopsy. The AVF was successfully treated with embolization. Post-biopsy observations should include Doppler surveillance in order to detect such rare but potentially catastrophic complications.
Keywords: Fistula embolization, Kidney biopsy, Lumbar artery aneurysm, Lumbo-renal fistula
Introduction
Percutaneous kidney biopsy is a common procedure used to diagnose renal pathologies. Although various complications have been documented in the literature, the formation of a lumbo-renal arteriovenous fistula (AVF) as a result of this procedure remains undocumented. Despite an extensive search across various medical databases including Google Scholar, PubMed, Medline, and Uptodate, no similar case report has been identified. While previous reports have primarily focused on intrarenal AVF following kidney biopsy. This report presents an unprecedented case of a lumbo-renal fistula formation subsequent to percutaneous kidney biopsy, marking a significant contribution to the current body of medical knowledge.
Case Report
A 77-year-old male was admitted with breathlessness and decreased urine output. He had no known comorbidities. Investigations revealed Urea 211 mg/dL, Creatinine 10.7 mg/dL, and Hemoglobin 7.6 g/dL. He was dialyzed immediately through a temporary right Internal Jugular Vein catheter.
A kidney biopsy was planned to know the cause of kidney failure. Left lower pole kidney biopsy done under ultrasound (USG) guidance. The patient was shifted to the ward after 2 hours of supervision.
Check sonography and Doppler were done after 24 hours, it showed the continuous movement of blood out of the kidney. There was no hypotension or drop in the hemoglobin.
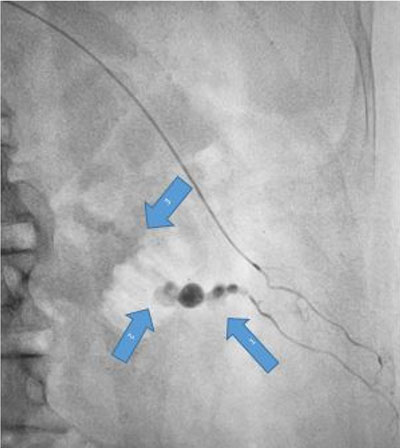
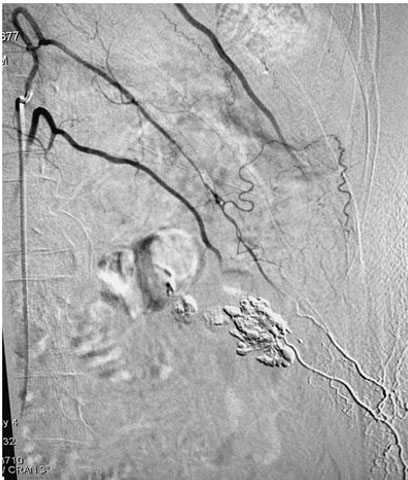
Urgent digital subtraction angiography (DSA) was done through right femoral access. The aortic angiogram showed no pseudoaneurysm or contrast extravasation from the left renal artery. However, the left lumbar artery at the L2 level showed a pseudoaneurysm with fistulous communication with the renal vein along the biopsy tract with contrast leak on delayed figures (Figure 1 and Figure 2).
Selective cannulation of the lumbar artery was attempted but it failed due to acute angulation. Cannulation of the lumbar artery at the L1 level was done using a Sim catheter. Super selective angiographic runoff was taken with a progreat microcatheter. It showed filling of the lower L2 level lumbar artery through distal lumbo-limbar collateral vessels and confirmed the pseudoaneurysm and left lumbo-renal venous fistula. Because of difficult anatomy glue embolization of the fistula was done using glue: lipiodol mixture (16% glue). Post-procedure angiogram showed closer of fistula and contrast extravasation (Figure 3).

Discussion
Complications after kidney biopsies have been reduced tremendously with the advent of real-time Doppler and sonography. However, needling the highly vascular kidney’s cortex through the richly vascular retroperitoneal area cannot be completely risk-free.
The kidney cortex receives 20% of cardiac output in its extensive network of blood vessels. Similarly, the lumbar arteries make multiple anastomoses with intercostal, vertebral, and iliac arteries, creating a richly vascular retroperitoneal bed. Any intervention in this area is likely to result in vascular injuries and related consequences [1],[2],[3],[4].
The AVF formation is one of the complications of doing a kidney biopsy through the retroperitoneal area. The incidence of intra-renal AVF formation ranges from 0.3% to 5.6% in native kidneys and 10–16% in transplant kidney biopsies [5]. Intra-renal AVF usually forms between renal vessels, and it is uncommon for extrarenal vessels to form a fistula with intrarenal vessels.
Our case involves an AVF between an intercostal branch of the lumbar arteries and the renal vein which developed after a percutaneous lower pole kidney biopsy. This is an extremely rare complication that has not been reported thus far.
The majority of AVFs (intrarenal) do not require intervention and typically close spontaneously in a few months. Extrarenal AVF is usually symptomatic and needs intervention. The usual symptoms are macro-or micro-hematuria, retroperitoneal hematoma, renal hypoperfusion, accelerated or difficult-to-treat hypertension, and flank pain [6].
Selective embolization of the affected vessels is the preferred treatment option and has been successful in obliterating AVF in more than 85% of cases. Rarely total or partial nephrectomy is required. Angiography followed by selective embolization is a minimally invasive technique and results are usually immediately evident. Embolization agents such as particles of polyvinyl alcohol (PVA), microcoils, and glue and gelatine sponge are used [7],[8],[9],[10],[11],[12]. The microcoil is the best option for the arterial embolization and it does not have any untoward effect on renal perfusion. Gelatin sponge can be used if a coil does not induce complete thrombosis.
However, embolization in the lumber artery requires special attention due to its role in supplying blood to the spinal cord. Liquid agents for embolization in this anatomical location are generally not advisable.
Complications after embolization are relatively infrequent and include post-embolization syndrome, infection, and sometimes progressive renal dysfunction.
Post-embolization syndrome is characterized by fever and low back pain which usually improve with symptomatic treatment. Patients at risk of infection should receive antibiotic prophylaxis.
Conclusion
In conclusion, the formation of post-biopsy arterial aneurysms and AVF is not uncommon. Fortunately, most of these instances involve small and intrarenal AVF with a high rate of spontaneous closer. However close observation is needed at least for initial few months to avoid renal hypoperfusion which can compromise kidney’s function in long term. Resistant or new onset hypertension is also an indication for the treatment of AVF. Extrarenal fistulas are very rare and usually require interventions.
REFERENCES
1.
Salam B, Khandwala K. Lumbar artery pseudoaneurysm following renal biopsy. Cureus 2018;10(5):e2634. [CrossRef]
[Pubmed]

2.
Mifune Y, Yagi M, Iwasaki Y, Doita M. Pseudoaneurysm of lumbar artery following a vertebral biopsy: A case report. Case Rep Radiol 2012;2012:127124. [CrossRef]
[Pubmed]
3.
Ramsay DW, Marshall M. Lumbar artery pseudoaneurysm following renal biopsy: Treatment with ultrasound-guided thrombin injection. Australas Radiol 2002;46(2):201–3. [CrossRef]
[Pubmed]
4.
Ito T, Ishikawa E, Ito M. Lumbar artery injury following renal biopsy. Clin Exp Nephrol 2016;20(1):145–6. [CrossRef]
[Pubmed]
5.
Sosa-Barrios RH, Burguera V, Rodriguez-Mendiola N, et al. Arteriovenous fistulae after renal biopsy: Diagnosis and outcomes using Doppler ultrasound assessment. BMC Nephrol 2017;18(1):365. [CrossRef]
[Pubmed]
6.
Rüth EM, Dittrich K, Jüngert J, Uder M, Rascher W, Dötsch J. Successful interventional treatment of arteriovenous fistula after kidney biopsy in pediatric patients—A report of three cases. Nephrol Dial Transplant 2008;23(10):3215–8. [CrossRef]
[Pubmed]
7.
Paredes-Mariñasa E, Llort-Ponta C, Mateos-Torres E, Crespo-Barrio M, Barrios-Barrera C, Clará-Velasco A. Percutaneous treatment of an arteriovenous fistula and pseudoaneurysm after a transplanted kidney biopsy. Nefrologia 2013;33(5):744–5. [CrossRef]
[Pubmed]
8.
Haochen W, Jian W, Li S, Tianshi L, Xiaoqiang T, Yinghua Z. Superselective renal artery embolization for bleeding complications after percutaneous renal biopsy: A single-center experience. J Int Med Res 2019;47(4):1649–59. [CrossRef]
[Pubmed]
9.
Somani BK, Nabi G, Thorpe P, McClinton S. Endovascular control of haemorrhagic urological emergencies: An observational study. BMC Urol 2006;6:27. [CrossRef]
[Pubmed]
10.
Mavili E, Dönmez H, Ozcan N, Sipahioğlu M, Demirtaş A. Transarterial embolization for renal arterial bleeding. Diagn Interv Radiol 2009;15(2):143–7.
[Pubmed]
11.
Ierardi AM, Floridi C, Fontana F, et al. Transcatheter embolisation of iatrogenic renal vascular injuries. Radiol Med 2014;119(4):261–8. [CrossRef]
[Pubmed]
12.
Sayani R, Azeemuddin M, ul Haq T, Hamid RS, Salam B. An institutional review of transarterial embolization in haemorrhagic urological emergencies. J Pak Med Assoc 2012;62(2):107–11.
[Pubmed]
SUPPORTING INFORMATION
Acknowledgments
The author thanks B Poat (Department of Interventional Radiology, Hinduja Hospital), R Balsarkar (Department of Radiology, Hinduja Hospital), A Almeida, R Sirsat, A Dey, K Bijapur, S Lute (Department of Nephrology, Hinduja Hospital) for their help.
Author ContributionsKhairwar Mahesh Prasad - Conception of the work, Design of the work, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthor declares no conflict of interest.
Copyright© 2023 Khairwar Mahesh Prasad. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}