 |
Case Report
Laryngeal abscess formation secondary to utilization of nasogastric tube in oral cancer patient: A case report
1 Department of Dentistry and Oral Surgery, Pediatric Dentistry, National Hospital Organization Tochigi Medical Center, Tochigi, Japan
2 Department of Oral and Maxillofacial Surgery, Tokyo Metropolitan Cancer and Infectious Diseases Center Komagome Hospital, Tokyo, Japan
3 Department of Dentistry and Oral Surgery, Keio University School of Medicine, Tokyo, Japan
4 Division of Dentistry and Oral Surgery, Shizuoka Cancer Center Hospital, Shizuoka, Japan
Address correspondence to:
Seiji Asoda
DDS, PhD, Department of Dentistry and Oral Surgery, Keio University School of Medicine, 35 Shinanomachi, Shinjyuku-ku, Tokyo 160-0016,
Japan
Message to Corresponding Author
Article ID: 101412Z01KN2023
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Nishi K, Yamada M, Karube T, Ochiai S, Asoda S, Suga K. Laryngeal abscess formation secondary to utilization of nasogastric tube in oral cancer patient: A case report. Int J Case Rep Images 2023;14(2):63–68.ABSTRACT
Introduction: Although laryngeal abscess is a rare disease in this day when antibiotics and vaccines are widely available, it can be fatal in terms of choking risk due to airway narrowing and thus requires an immediate diagnosis and treatment, including airway management. Even in the field of oral surgery, where nasogastric tubes are often used for nutritional management, there have been no reports of laryngeal abscesses.
Case Report: One month after right maxillary gingival carcinoma surgery, a 72-year-old man had hoarseness and a fever following nasogastric tube replacement, and blood tests showed a marked increase in inflammatory levels. The patient started chemotherapy with SBT/ABPC (12 g/day). Contrast-enhanced magnetic resonance imaging showed a low-density area with a rim enhancement effect from the left laryngeal surface of the epiglottis to the left supraglottis, which had caused airway narrowing, leading to a diagnosis of laryngeal abscess. Considering the risk of airway obstruction, a tracheostomy was performed under general anesthesia. On day 16, contrast-enhanced computed tomography showed a reduction in the lesion size. On day 36, antibiotic chemotherapy was terminated. At 10 months after surgery, lung metastasis developed without local or cervical recurrence, and chemotherapy was off-label due to his worsening renal function. Therefore, the best supportive care policy was selected. The patient’s general condition gradually deteriorated, and he died 11 months after the surgery.
Conclusion: There are very few reports related to nasogastric tubes, so it is necessary to keep the disease concept of laryngeal abscess in mind, especially in the field of oral surgery, where nasogastric tubes are often used for nutritional management.
Keywords: Laryngeal abscess, Pharyngeal pain, Vocal cord paralysis
Introduction
Although laryngeal abscess is a rare disease in this day when antibiotics and vaccines are widely available, it can be fatal in terms of choking risk due to airway narrowing and thus requires an immediate diagnosis and treatment, including airway management [1]. It is often secondary to acute epiglottitis or epiglottis cysts and has been suggested to be associated with endotracheal intubation, postoperative tumor surgery, and immunosuppressed states [2]. However, very few cases have been related to nasogastric tubes [2]. Indeed, even in the field of oral surgery, where nasogastric tubes are often used for nutritional management, there have been no reports of laryngeal abscesses. We herein report a case of laryngeal abscess that developed secondary to nasogastric tube insertion after maxillary gingival cancer surgery.
Case Report
In April 2021, a 72-year-old Japanese man was referred to our department for postextraction wound healing failure in the right maxillary molar region. Regarding the extraoral findings, a small and mobile lymph node, the size of the tip of a pinky finger, was palpated in the right submandibular region. Intraorally, a large exophytic mass measuring 25×20 mm in size with surrounding induration was observed on the gingiva of the right maxillary molar region (Figure 1). The patient’s medical history included diabetes. Panoramic X-ray revealed rough bone resorption in the extraction area. Computed tomography (CT) revealed irregular marginal bone resorption with buccal cortical bone destruction in the right maxillary molar region. In addition, an enlarged lymph node with a mild contrast effect 8 mm in short diameter was seen in the right submandibular region (Figure 2A and Figure 2B). Magnetic resonance imaging (MRI) revealed a lesion with low signal intensity on T1-weighted imaging and high signal intensity on fat-suppressed T2-weighted imaging in the right maxillary molar region. Gadolinium contrast-enhanced T1-weighted imaging showed internal heterogeneous contrast effects (Figure 2C). In the same month, we performed a biopsy under local anesthesia. Based on the results of a histopathological examination, the diagnosis was intermediate-differentiated squamous cell carcinoma. Fluorodeoxyglucose-position emission tomography (FDG-PET) revealed that the maximum standardized uptake value (SUVmax) of the lesion in the right maxillary and right submandibular lymph nodes and the right superior internal jugular vein lymph node was 9.83, 3.25, and 3.32, respectively. There were no obvious other metastases. Upper gastrointestinal endoscopy revealed no double cancer in the upper gastrointestinal tract. Based on these findings, the cancer was classified as T2N2bM0.
In May 2021, right-side partial maxillectomy and modified radical neck dissection (type III) were performed under general anesthesia, a nasogastric tube (12 Fr) was inserted intraoperatively, and postoperative nutritional management was provided by tube feeding. Based on the final histopathological examination, postoperative radiation therapy to the right side of the neck and maxilla was planned.
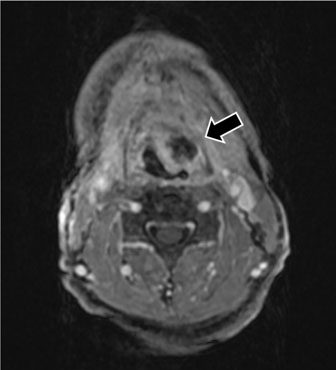
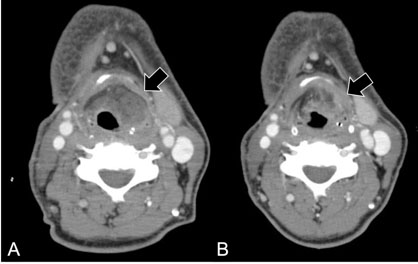
The postoperative course of the wound was good. A nasogastric tube (8 Fr) was replaced one month after surgery (setting this date as day 0), and the patient had discomfort in the laryngeal region from the next day (day 1) (Figure 3). Therefore, the nasogastric tube (8 Fr) was replaced again on day 2, but the patient had swallowing pain, and CT revealed mild swelling of the left pharynx (Figure 4). On day 4, the patient had hoarseness and a fever; furthermore, erythematous and tenderness were observed on the skin around the left thyroid cartilage. Blood tests performed on the same day showed a markedly increased white blood cell count of 28,700/μL and C-reactive protein (CRP) of 24.7 mg/dL, and chemotherapy with SBT/ABPC (12 g/day) was started. Contrast-enhanced MRI taken on day 6 showed a low-density area with a rim enhancement effect from the left laryngeal surface of the epiglottis to the left supraglottis, which caused the airway to narrow, leading to a diagnosis of laryngeal abscess (Figure 5). The patient was immediately referred to the Department of Otorhinolaryngology in our hospital. Laryngoscopy revealed abrasions on the laryngeal surface of the epiglottis, erythematous of the left glottis, and left vocal cords that were fixed in the fully open position, showing closure failure (Figure 6). Infection of the left side of the pharynx and larynx was thought to be the cause of the inflammation. Considering the risk of airway obstruction, the gastric tube was removed, and tracheostomy was performed under general anesthesia. Intraoperatively, an otolaryngologist performed surgical drainage directly with a laryngoscope. The patient continued to be treated with antibiotic chemotherapy. Since the patient was undernourished (Alb: 2.5 mg/dL), a nasogastric tube (12 Fr) was reinserted on day 7, and tube feeding was resumed. Steroid therapy with 300 mg/day hydrocortisone intravenously was started on the same day, and the dose was gradually decreased by 100 mg/day until day 9. On day 8, contrast-enhanced CT showed a slightly enlarged low-density area (Figure 7A), but blood tests showed a tendency toward improvement of inflammation. Considering that the patient had developed a sore throat and vocal cord paralysis under nasogastric tube insertion, the 12-Fr nasogastric tube was replaced with an 8-Fr one on day 14. On day 16, contrast-enhanced CT showed a reduction in the lesion size. On day 23, further improvement was observed, with white blood cell counts of 9600/μL and a CRP level of 0.56 mg/dL, and contrast-enhanced CT showed a further reduction in the lesion size (Figure 7B). The tracheal cannula was removed on the same day, and antibiotic chemotherapy was terminated on day 36. Thereafter, the patient had no relapse of his fever, sore throat, or vocal cord paralysis and was discharged from the hospital on day 92 after completing postoperative radiation therapy.
At 10 months after surgery, lung metastasis developed without local or cervical recurrence, and chemotherapy was off-label due to a worsening renal function. Therefore, the best supportive care policy was selected. The patient’s general condition gradually deteriorated, and he died 11 months after the surgery.





Discussion
The frequency of laryngeal abscesses has decreased dramatically with the development of antibiotics, becoming extremely rare in recent years [1],[3]. These lesions are thought to develop in association with damage to the laryngeal mucosa caused by trauma, radiation therapy, or tracheal intubation [2]. The symptoms include sore throat, hoarseness, and dyspnea. The time from the triggering episode to the onset of disease has been reported to typically range from a few days to a few weeks [4],[5], but there was also a report of a case that took four months to manifest [6].
Laryngeal abscess is diagnosed by blood tests, laryngoscopy, and contrast-enhanced CT of the neck. There has only been one other reported case of laryngeal abscess triggered by a nasogastric tube in the field of otorhinolaryngology [2], as in the present case. In that case, when the nasogastric tube was removed on day 4 after insertion, the patient developed pharyngeal pain and neck tenderness two days after the tube was removed, and tracheotomy was performed to relieve the symptoms. In our case, the day after the nasogastric tube was replaced, the patient reported discomfort in the laryngeal region, and after the gastric tube was removed and reinserted the next day, hoarseness and left-sided vocal cord paralysis were observed. In addition, laryngoscopy revealed abrasions on the laryngeal surface of the epiglottis and in the supraglottis, suggesting that the laryngeal mucosa had been damaged by irritation of the periglottic tissues in a short period of time, which led to the development of a laryngeal abscess. Complications associated with nasogastric tube insertion may include esophageal injury and incorrect insertion into the airway. The usual route of insertion is likely to damage the posterior wall of the pharynx, but there have also been reports of ulceration of the deep cricoid cartilage due to nasogastric tube insertion. While a rare occurrence, nasogastric tube insertion can also damage the perilaryngeal mucosa [7]. Another possible complication is nasogastric tube syndrome [8]. This is a rare syndrome that causes sore throat, bilateral vocal cord paralysis, and laryngeal edema during nasogastric tube insertion, but it is an extremely urgent condition, as the bilateral vocal cords become fixed and closed in the midline position. Laryngeal abscesses also often cause some vocal cord symptoms by affecting their movement due to the spread of inflammation [4], but bilateral midline fixation of the vocal cords is extremely rare. In the present case, the unilateral vocal cord was fixed in a fully opened position; it was in a state of disclosure and was not bilateral. Therefore, this case was not diagnosed as nasogastric tube syndrome but rather laryngeal abscess alone.
Diabetes mellitus, corticosteroid administration, and an immunocompromised status are risk factors for the development of laryngeal abscesses [9]. Our patient had a medical history of diabetes mellitus and a low Alb level (Alb 2.8 g/dL on the 13th postoperative day) on blood test. The delayed healing of the abraded wound was attributed to decreases in the immunity and wound healing functions, leading to the formation of an abscess.
The treatment of laryngeal abscesses requires antibiotic administration and surgical drainage, as well as airway management in many cases. Steroid administration for anti-inflammatory purposes may be useful, but as mentioned above, it is also a risk factor for laryngeal abscess, and its use should be carefully considered [10]. In general, abscesses under the hyoid bone have a very high risk of developing into mediastinal abscesses or causing respiratory compromise [11]; therefore, adequate management is needed, including tracheostomy and surgical drainage, as in this case.
Although laryngeal abscesses are extremely rare in the field of oral surgery, they can occur in postoperative patients undergoing general anesthesia requiring endotracheal intubation and patients undergoing nasogastric tube insertion in any age group. If a laryngeal abscess develops, the rapid deterioration of the disease can be fatal. Therefore, the possibility of laryngeal abscess or nasogastric tube syndrome should always be kept in mind when a postoperative patient or a patient with a nasogastric tube inserted has a sore throat. Since there are no clear guidelines for the diagnosis and treatment of these conditions and the evidence base is insufficient, the further accumulation of knowledge is desirable.
Conclusion
In the present study, we experienced a case of laryngeal abscess secondary to nasogastric tube insertion after maxillary gingival cancer surgery. There are very few reports of laryngeal abscesses associated with nasogastric tubes, and it is necessary to keep the disease concept of laryngeal abscesses in mind, especially in the field of oral surgery, where nasogastric tubes are often used for nutritional management.
REFERENCES
1.
Canalis RF, Jenkins HA, Osguthorpe JD. Acute laryngeal abscesses. Ann Otol Rhinol Laryngol 1979;88(2 Pt 1):275–9. [CrossRef]
[Pubmed]

2.
Souliere CR Jr., Kirchner JA. Laryngeal perichondritis and abscess. Arch Otolaryngol 1985;111(7):481–4. [CrossRef]
[Pubmed]
3.
Clemons JE, Portilla W. Laryngeal abscess. Otolaryngol Head Neck Surg 1979;87(3):339–41. [CrossRef]
[Pubmed]
4.
Cohen E, Blickstein D, Inbar E, Samra Z, Weinberger M. Unilateral vocal cord paralysis as a result of a Nocardia farcinica laryngeal abscess. Eur J Clin Microbiol Infect Dis 2000;19(3):224–7. [CrossRef]
[Pubmed]
5.
Zapanta PE, Bielamowicz SA. Laryngeal abscess after injection laryngoplasty with micronized AlloDerm. Laryngoscope 2004;114(9):1522–4. [CrossRef]
[Pubmed]
6.
McNellis EL, Hoang KG. Immunosuppression and systemic lupus erythematosus predisposing to laryngeal abscess. Otolaryngol Head Neck Surg 1997;116(1):107–9. [CrossRef]
[Pubmed]
7.
Friedman M, Baim H, Shelton V, et al. Laryngeal injuries secondary to nasogastric tubes. Ann Otol Rhinol Laryngol 1981;90(5 Pt 1):469–74. [CrossRef]
[Pubmed]
8.
Sofferman RA, Hubbell RN. Laryngeal complications of nasogastric tubes. Ann Otol Rhinol Laryngol 1981;90(5 Pt 1):465–8. [CrossRef]
[Pubmed]
9.
Vanhille DL, Blumin JH. Laryngeal abscess formation in an immunosuppressed patient: A case report. Laryngoscope 2017;127(12):2827–9. [CrossRef]
[Pubmed]
10.
Lapointe A, Parke RB, Kearney DL, Morriss MC, Krance RA, Friedman EM. Laryngectomy for fungal abscesses of the larynx. Otolaryngol Head Neck Surg 2004;131(6):1007–8. [CrossRef]
[Pubmed]
11.
Gehrke T, Scherzad A, Hagen R, Hackenberg S. Deep neck infections with and without mediastinal involvement: Treatment and outcome in 218 patients. Eur Arch Otorhinolaryngol 2022;279(3):1585–92. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Acknowledgments
The authors would like to thank Dr. Takashi Kojima for his support of treatment.
Author ContributionsKentaro Nishi - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Manabu Yamada - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Takeshi Karube - Conception of the work, Design of the work, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Shunsuke Ochiai - Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Seiji Asoda - Conception of the work, Design of the work, Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Kenichiro Suga - Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2023 Kentaro Nishi et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}