 |
Case Report
Giant vesical calculus associated with staghorn calculus
1 Urology service at Getúlio Vargas University Hospital (HUGV), 4 Apurinã Avenue, Praça 14 de Janeiro, Manaus, Amazonas, Brazil
2 Faculty of Medicine of the Federal University of Amazonas (UFAM), 1053 Afonso Pena St, Praça 14 de Janeiro, Manaus, Amazonas, Brazil
3 Urology service at Ribeirão Preto’s Santa Casa de Misericórdia Hospital, São Paulo, 456 Saudade Av, Campos Elíseos, Ribeirão Preto, Brazil
Address correspondence to:
Igor Ferreira de Souza
9999 Buriti Av, Eliza Miranda Condo, Block B, Apt 103, Manaus, AM 69075-000,
Brazil
Message to Corresponding Author
Article ID: 101387Z01IS2023
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
de Souza IF, de Castro GL, da Silva Barroso FM, Vasquez VAV, de Souza PM, da Costa Teixeira Neto AM. Giant vesical calculus associated with staghorn calculus. Int J Case Rep Images 2023;14(1):75–79.ABSTRACT
Introduction: Large vesical calculi are rare conditions in urology due to the advancement of image exams in the last decade. Urinary bladder stones represent 5% of all urinary tract calculi and large calculi are defined as weighing more than 100 grams.
Case Report: We report the case of a 56-year-old man with large vesical calculus measuring 17 × 13 × 16 cm (weight of 2730 g) in association with renal exclusion due to staghorn calculus in the right kidney and bilateral uretero-hydronephrosis due to bladder obstruction.
Conclusion: Computed tomography stands as the exam of choice to diagnose and delimit any urinary calculi. Open surgery is preferred for large vesical stones and bladder outlet obstruction must be investigated, especially in men to exclude prostate increase.
Keywords: Calculus, Cystolithotomy, Staghorn calculus, Urinary bladder, Vesical stone
Introduction
Giant vesical calculus is uncommon in modern urology practice. It is defined as urinary bladder stone weighing more than 100 g. Bladder stones usually occur due to urinary tract infection (UTI) or obstruction or enlargement of the prostate gland in men and are responsible for 5% of all urolithiasis [1],[2],[3],[4].
Urinary bladder stones can be classified as primary or secondary. The primary stones are common in children with low protein diet, while secondary stones are associated with urinary obstruction, neurogenic bladder, or bladder diverticulum [5].
Bladder stones may evolve asymptomatic or symptomatic. Patients with clinical manifestations may present urinary tract infection symptoms such as dysuria, pollakiuria and hematuria. Severe symptoms as urinary retention or hydronephrosis can also be present [1],[3].
The largest vesical calculus reported in literature weighed 6294 g [6]. We report a case of giant vesical calculus measuring 17 × 13 × 16 cm and weighing 2730 g, associated with staghorn calculus in right kidney.
Case Report
A 56-year-old Brazilian man was admitted in our urgent urology service with chief complaint of dysuria and progressive decrease in urinary volume associated with painful mass in low abdomen. He also reported asthenia, hiccups, and vomiting for the last couple of weeks before admission. He had no significant past surgical history, comorbidities, or drug allergy. The patient reported palpable mass growth in low abdomen for the last 10 years with intense weight loss of almost 20 kg.
At first examination, the patient was stable, afebrile, acyanotic, anicteric, dehydrated, and vital signs in normal values. He currently weighed 50 kg and there were no respiratory or cardiac abnormal findings in physical examination. The abdomen was plan, with painful hardened hypogastric protrusion, well delimited in a circumferential form, without any sings of peritoneal irritation (Figure 1).
Admission laboratory tests showed leukocytosis with white blood cells of 16.160 [reference value (RV): 5.2–12.4), severe anemia with hemoglobin value of 6.6 (RV: 12–18), urea of 313 (RV: 10–40), creatinine of 8.43 (RV: 0.5–1.3) and glucose level of 124 mg/dL. He was submitted to blood transfusion and dialysis due to uremic state. Hemoglobin level increased for 9.5 after transfusion. COVID-19 test was negative. Urine culture was not performed due to the temporarily unavailable facility in our public service.
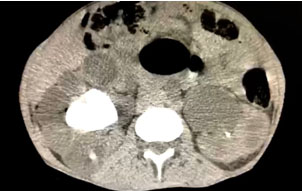
The patient was submitted to an abdominal computed tomography (CT) scan that revealed giant vesical calculus measuring 17.0 × 13.0 × 16.0 cm and volume of 1838 cm3 (Figure 2). Computed tomography also revealed staghorn calculus in the right kidney with 1297 Hounsfield unity (HU) density and intense hydronephrosis and loss of corticomedullary relation and the left kidney with non-obstructive 1.4 cm calculi and moderate hydronephrosis due to vesical obstruction (Figure 3).
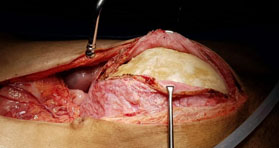
Due to suspicion of urinary sepsis secondary staghorn calculus and possibility of renal abscess, the right nephrectomy was opted as treatment to remove possible infectious focus. He was approached through supra- and infra-umbilical median incision under general anesthesia. Vesical catheterization was installed after anesthesia and cystolithotomy was first performed by two urologists. Large calculus was identified without any adherence with bladder wall and it was easily removed from inside of the urinary bladder (Figure 4). Urinary bladder was close in one layer due thinning wall with vicryl 2-0. Cattell-Braasch maneuver was executed with lobulated hydronephrotic right kidney identified and the right nephrectomy was performed (Figure 5). Intensive care unit (ICU) was requested for post-operative.
In third post-operative day, the patient evolved unstable and mechanical ventilation with orotracheal tube was installed. Urinary sepsis and severe metabolic acidosis [pH 6.9 (RV: 7.35–7.45) and bicarbonate of 5.4 (RV: 22–26)] were diagnosed. Unfortunately, efforts to reverse his clinical condition failed and outcome was unfavorable with obit.



Discussion
Giant vesical calculus is unusual and defined as weighing more 100 g, with only few cases reported of more than 1000 g. Urinary bladder calculi represent 5% of all calculi in urinary tract and are more common in males. Etiology is related with urinary retention, bladder obstruction and infection, neurogenic bladder, and prolonged catheterization. Most cases of vesical calculus are composed of triple phosphate, calcium carbonate, and calcium oxalate, although this analysis was not possible in our case once this service was currently unavailable [1],[2],[3],[7].
Patients with vesical calculi can present recurrent urinary tract infection, urinary retention, and hematuria. Bladder calculi are also associated with bladder cancer due to chronic irritation and inflammation. In cases of large vesical calculus as ours, hydronephrosis can be observed due to ureteral obstruction associated with suprapubic tenderness [4],[8],[9].
Vesical calculi are frequently multilayered and diagnosed through image exams. Most cases are detected by radiography; nonetheless, non-contrast-enhanced CT is considered for standard investigation. In cases of kidney stones or ureteral obstruction by large calculus, CT provides anatomic enhancement [2],[3].
Open cystolithotomy is the procedure of choice to remove large vesical calculus due to better surgical view and possibility of adherences in vesical wall. Endoscopic surgery is preferred for small or moderate calculi and can be combined with surgical procedures for bladder outlet obstruction [1],[3],[7],[8],[9]. Our patient was managed with supra- and infra-umbilical median incision due to extreme large vesical calculus of 17.0 × 13.0 × 16.0 cm and also renal exclusion due to staghorn calculus. Cystolithotomy and right nephrectomy was performed.
Unfortunately, in our case outcome was not favorable which can be associated with the patient’s critical condition in admission due to extended progression of the case to renal failure.
Conclusion
Large vesical calculi are extremely uncommon in current urology practice and can be diagnosed through image exams, with CT as standard investigation. Bladder outlet obstruction must be excluded, especially in men. Open surgical treatment is preferred for large calculi and outcome is generally favorable.
REFERENCES
1.
Aliyu S, Ali N, Ibrahim AG. Giant vesical calculus. Niger J Med 2013;22(2):148–50.
[Pubmed]

2.
Joseph S, Nathwani P, Lamba RS, Joshi N, Pujari N. Giant vesical calculus: A rare case report. Int J Sci Stud 2016;4(1):304–6.
3.
Otieno W, Otieno FA, Omondi T. Giant urinary bladder calculus: Case report. East African Medical Journal 2015;92(9):465–7.
4.
Gangwar P, Singh P, Reena, Agrawal S. Giant vesical calculus with its complications: The first case to be reported in an adolescent female. Indian J Case Reports 2020;6(2):76–7.
5.
Schwartz BF, Stoller ML. The vesical calculus. Urol Clin North Am 2000;27(2):333–46. [CrossRef]
[Pubmed]
6.
Arthure H. A large abdominal calculus. J Obstet Gynaecol Br Emp 1953;60(3):416. [CrossRef]
[Pubmed]
7.
Hussain Hela A, Wani M, Mohammad Khandwaw H, Jyoti D. Giant multiple vesical calculi: A case report. Urol Case Rep 2020;33:101264. [CrossRef]
[Pubmed]
8.
Garg V, Awasthi RC, Jain G, Pandey S, Maheshwari MK. Giant vesical calculus. Int J Med and Dent Sci 2016;5:1265–8.
9.
Ma C, Lu B, Sun E. Giant bladder stone in a male patient: A case report. Medicine (Baltimore) 2016;95(30):e4323.
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Igor Ferreira de Souza - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Gustavo Lopes de Castro - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Francisco Marcos da Silva Barroso - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Victor Alfonso Vela Vasquez - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Paloma Menezes de Souza - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Algenor Maria da Costa Teixeira Neto - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2023 Igor Ferreira de Souza et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}