 |
Case Report
Metastatic proximal-type epithelioid sarcoma presenting as a chest lesion with a pathological fracture of the humeral neck
1 Registrar in Radiology, Department of Radiology, Teaching Hospital Peradeniya, Peradeniya, Sri Lanka
2 Head, Consultant Radiologist, Department of Radiology, Faculty of Medicine, University of Peradeniya, Peradeniya, Sri Lanka
3 Head, Professor, Consultant Pathologist, Department of Pathology, Faculty of Medicine, University of Peradeniya, Peradeniya, Sri Lanka
4 Professor, Consultant Radiologist, Department of Radiology, Faculty of Medicine, University of Peradeniya, Peradeniya, Sri Lanka
Address correspondence to:
Rajashilpa Mulacharige Madhuwan Sasira Kasun Kumara
Karandagolla, Post Code 20738,
Sri Lanka
Message to Corresponding Author
Article ID: 101345Z01RK2022
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Kumara RMMSK, Jeevani U, Prabodini MAM, Sulochana W, Badra HP. Metastatic proximal-type epithelioid sarcoma presenting as a chest lesion with a pathological fracture of the humeral neck. Int J Case Rep Images 2022;13(2):137–141.ABSTRACT
Introduction: Proximal-type epithelioid sarcoma is a rare soft tissue neoplasm which occurs mostly in young males and is much rarer than classic distal sub type. A young male, with a known diagnosis of neurofibromatosis type 1 (NF1) presenting with metastatic proximal-type epithelioid sarcoma is reported.
Case Report: A 30-year-old male with known NF1, hypothyroidism, epilepsy, presented with a right shoulder pain of two weeks duration. Plain radiographs revealed an expansile lytic lesion, an aggressive periosteal reaction in right humeral head with an underlying pathological fracture. A well-defined extrapulmonary mass with a lobulated margin in upper zone of right hemithorax with inferior rib erosion of 3rd rib and the 3rd intercostal space widening were also observed. Contrast-enhanced computed tomography (CECT) chest and abdomen confirmed peripherally located poorly enhancing soft tissue mass with lobulated margins arising from posterior chest wall along with a subdiaphragmatic deposit. Multiple lytic lesions in right head of humerus with an underlying pathological fracture of surgical neck, T2, T6, and L3 vertebral bodies, and pelvic bones were observed too. Diagnosis of malignant peripheral nerve sheath tumor with metastases was made and ultrasound-guided biopsy of chest wall lesion was performed. Histology and immunohistochemistry (IHC) revealed a proximal type epithelioid sarcoma. The patient was managed with palliative surgery and oncological follow-up.
Conclusion: Presentation of proximal-type epithelioid sarcoma with disseminated metastases in a patient with NF1 masquerading malignant peripheral nerve sheath tumor (MPNST) and the challenges of diagnosis on clinical, radiological, and histopathology as well as IHC perspectives of this rare disease entity is highlighted.
Keywords: Epithelioid sarcoma, Metastatic, Pathological fracture, Proximal type
Introduction
Epithelioid sarcoma (ES) is a rare malignant slow-growing mesenchymal tumor of unknown etiology with multidirectional differentiation which is mainly epithelial [1]. It has a less than 1% incidence among all soft tissue sarcomas [2]. It starts mostly in the soft tissues as a small firm painless growth under the skin of a finger, hand, forearm, lower leg, or foot. However, it can grow in other areas of the body. It can be cured if detected early and treated with surgical resection, even though recurrence and metastases are well known due to its aggressive behavior [2].
Epithelioid sarcoma was first described by Enzinger in 1970 as a distinct clinicopathological disease entity [3]. World Health Organization (WHO) categorizes it under soft tissue tumors of uncertain differentiation [4]. In contrast to most soft tissue sarcomas, ES characteristically spreads via lymphatics to noncontiguous areas of skin, deep soft tissue, fascia, and bone, and it also shows direct extension [5].
Epithelioid sarcoma is mainly divided into two types. The commoner one is distal or classic sub type. It usually found in the distal extremities mostly affecting the volar surfaces of hand and fingers [4]. Proximal-type epithelioid sarcoma (PES) is a rare soft tissue neoplasm which occurs more often in young males [3]. It is usually found in proximal extremity or axial location [2],[5]. Proximal-type epithelioid sarcoma usually arises in deep soft tissues of the pelvis, perineal, genital, inguinal regions, chest wall as well as gluteal region, and hip. It can extend along tendon sheaths and/or fascia [3]. Histologically PES has divergent differentiation and the cells can have epithelioid and rhabdoid morphology with significant cellular pleomorphism. Necrosis may or may not be present. The classic or distal and PES variants of ES are characterized by co-expression of cytokeratin and vimentin and loss of integrase interactor-1 (INI1) staining. However, the tumor subtype shows significant molecular heterogeneity [5],[6],[7].
Differential diagnosis for an ES usually includes epithelioid type of malignant peripheral nerve sheath tumor (MPNST), rhabdomyosarcoma, angiosarcoma, synovial sarcoma, and undifferentiated carcinoma [2],[5].
Treatment options of both classic and PES types are surgical resection, amputation, radiotherapy, and chemotherapy. However, PES shows poorer prognosis compared to the classic form [5].
Owing to its rarity, aggressive behavior, we report a case of young male, with known NF1, presented with a pathological fracture of the right humerus and a large right chest wall soft tissue lesion finally diagnosed as metastatic proximal-type epithelioid sarcoma.
Case Report
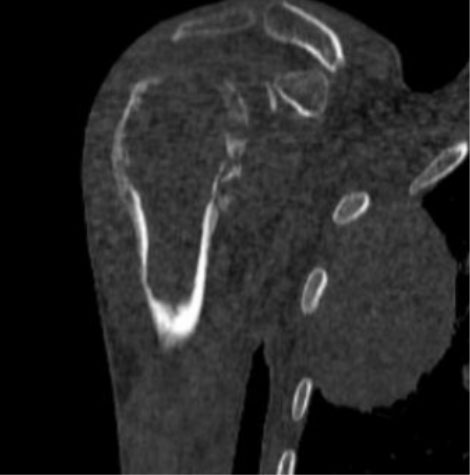
A 30-year-old male patient with multiple clinical problems such as neurofibromatosis type 1 (NF1), hypothyroidism, epilepsy, depression and who was investigated for gigantism in the childhood presented with a history of right shoulder pain of two weeks duration. Antero-posterior (AP) radiograph of right shoulder revealed an expansile lytic lesion with an aggressive type of periosteal reaction in right humeral head region with an underlying pathological fracture of the surgical neck (Figure 1). In addition, there was a well-defined radio-dense extrapulmonary lesion with a lobulated margin in upper zone of the right hemithorax on the AP shoulder radiograph (Figure 1). Subsequent postero-anterior (PA) chest radiograph confirmed a radio-dense well-defined chest wall lesion with lobulated margins in the upper zone of the right hemithorax. Inferior rib erosion was observed in posterior aspect of the 3rd rib with widening of intercostal space between the 3rd and 4th ribs (Figure 2). Rest of the right and left lung fields were normal and there were no pulmonary nodules, pleural effusions, or mediastinal or hila lymphadenopathy.
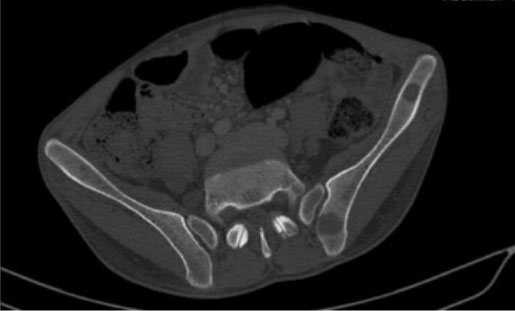
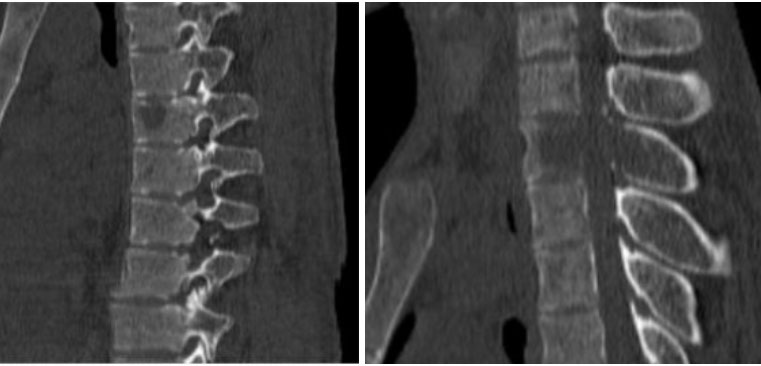
Contrast-enhanced computed tomography (CECT) chest and abdomen too confirmed the peripherally located poorly enhancing extrapleural soft tissue density mass, with lobulated margins arising from the posterior chest wall along with a subdiaphragmatic deposit (Figure 3 and Figure 4). Multiple lytic lesions were seen in right head of humerus with a pathological fracture of surgical neck, T2, T6, ad L3 vertebral bodies, as well as pelvic bones (Figure 5, Figure 6, Figure 7). Radiological diagnosis of MPNST with metastases was made and the patient was subjected to ultrasound-guided biopsy of the right chest wall lesion.
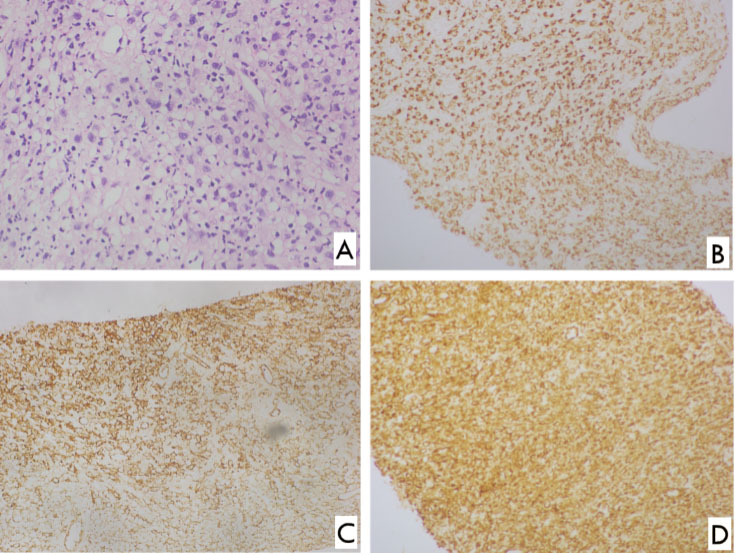
Histology revealed a tumor composed of sheets of cells with epithelioid morphology. Nuclei were moderately pleomorphic with scattered highly pleomorphic cells. Cytoplasm was pale eosinophilic and abundant. Rhabdomyoblastic differentiation was not evident. There was no perivascular accentuation of cellularity. There was extensive geographic necrosis and scattered neutrophils in the background. Pan-cytokeratin, vimentin, and CD 34 revealed strong diffuse positivity in cells. Cytokeratin 19 showed multifocal positivity. S-100 showed weak focal nuclear positivity. Smooth muscle actin, desmin, epithelial membrane antigen (EMA), cytokeratin 7, CD 31, and TTF-1 were negative. Ki-67 proliferative index was about 25%. The overall appearance was consistent with a proximal type epithelioid sarcoma (Figure 8). Finally, the patient was subjected to palliative surgery and oncological management. However, the patient succumbed to death within a short period of six months.




Discussion
In the indexed case the patient presented with a history of right-sided shoulder pain in a background of neurofibromatosis type 1 (NF1). In this clinical context of radiographic and CECT features of chest wall lesion with inferior rib erosion, intercostal widening, and pathological fracture of right humerus, and multifocal lytic bone lesions, diagnosis of malignant peripheral nerve sheath tumor (MPNST) with metastases was made. Radiological features described are non-specific, thus one has to consider proximal type of epithelioid sarcoma in the differentials, particularly in the presence of metastatic disease as concluded in a similar case report in Tokyo, Japan [8].
In the histological assessment, the differential diagnosis was an MPNST with epithelioid differentiation versus PES. Strong diffuse positivity for cytokeratin favored an epithelioid sarcoma. Furthermore, cytokeratin 19 and CD 34 are also frequently present in 72% of epithelioid sarcoma, not in MPNST [6]. Furthermore, expression of neural markers including S-100 has been reported in some cases of PES [6].
There is only one case report on PES associated with NF1 published to our knowledge, in which the patient presented with a posterior neck mass [9]. There are a few case reports with proximal type of epithelioid sarcoma in different locations [10],[11],[12].
Indexed case differs from above, as this is in a more central location and presented with more advanced state with disseminated metastatic disease, in a background of NF1.
This case report highlights the importance of considering proximal type epithelioid sarcoma as a differential for a chest wall soft tissue mass lesion with disseminated metastases in a young patient although it is rare.
Conclusion
Presentation of proximal-type epithelioid sarcoma with disseminated metastases in a patient with NF1 masquerading MPNST and the challenges of diagnosis on clinical, radiological, and histopathology as well as immunohistochemistry perspectives of this rare disease entity is highlighted in this case report. Association with NF1 needs further work-up as this is the second case report found in the literature. Early detection of proximal type epithelioid sarcoma may facilitate radical surgical excision which would be crucial to provide a chance of a cure in this rare disease.
REFERENCES
1.
Chase DR, Enzinger FM. Epithelioid sarcoma. Diagnosis, prognostic indicators, and treatment. Am J Surg Pathol 1985;9(4):241–63.
[Pubmed]

2.
Needs T, Fillman EP. Epithelioid Sarcoma. 2022 Apr 30. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2022.
[Pubmed]
3.
Enzinger FM. Epithelioid sarcoma. A sarcoma simulating a granuloma or a carcinoma. Cancer 1970;26(5):1029–41. [CrossRef]
[Pubmed]
4.
Bansal A, Goyal S, Goyal A, Jana M. WHO classification of soft tissue tumours 2020: An update and simplified approach for radiologists. Eur J Radiol 2021;143:109937. [CrossRef]
[Pubmed]
5.
Armah HB, Parwani AV. Epitheleoid sarcoma. Arch Pathol Lab Med 2009;133(5):814–9. [CrossRef]
[Pubmed]
6.
Hasegawa T, Matsuno Y, Shimoda T, Umeda T, Yokoyama R, Hirohashi S. Proximal-type epithelioid sarcoma: A clinicopathologic study of 20 cases. Mod Pathol 2001;14(7):655–63. [CrossRef]
[Pubmed]
7.
Thway K, Jones RL, Noujaim J, Fisher C. Epithelioid sarcoma: Diagnostic features and genetics. Adv Anat Pathol 2016;23(1):41–9. [CrossRef]
[Pubmed]
8.
Tateishi U, Hasegawa T, Kusumoto M, Yokoyama R, Moriyama N. Radiologic manifestations of proximal-type epithelioid sarcoma of the soft tissues. AJR Am J Roentgenol 2002;179(4):973–7. [CrossRef]
[Pubmed]
9.
Hwang SO, Lee SH, Lee HB. Epithelioid sarcoma associated with neurofibromatosis type I. Arch Craniofac Surg 2020;21(1):41–4. [CrossRef]
[Pubmed]
10.
Echchaoui A, Sadrati Y, Elbir Y, et al. Proximal-type epithelioid sarcoma: A new case report and literature review. Pan Afr Med J 2016;14:238. [CrossRef]
[Pubmed]
11.
Poisson JL, Rubinase TC. Proximal-type epithelioid sarcoma. Laboratory Medicine 2010;41(8):467–70. [CrossRef]
12.
Feger J. Epithelioid sarcoma. Radiopaedia 2022.
SUPPORTING INFORMATION
Acknowledgments
The authors thank staff of the Department of Radiology, Teaching Hospital Peradeniya and Department of Pathology, Faculty of Medicine, University of Peradeniya, those who supported in the establishment of the diagnosis of this case report.
Author ContributionsRajashilpa Mulacharige Madhuwan Sasira Kasun Kumara - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Udupihille Jeevani - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Mathara Arachchige Madusha Prabodini - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Wijetunge Sulochana - Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Hewavithana Padma Badra - Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2022 Rajashilpa Mulacharige Madhuwan Sasira Kasun Kumar. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}