 |
Case Report
Refractory advanced osteoradionecrosis (ORN) in the mandible: Analysis of predictive factors, clinical, imaging, and therapeutic characteristics
1 Master student, Department of Radiation Oncology, A.C. Camargo Cancer Center, Sao Paulo, Brazil
2 PhD Student, Department of Radiation Oncology, A.C. Camargo Cancer Center, Sao Paulo, Brazil
3 Master candidate, Department of Radiation Oncology, A.C. Camargo Cancer Center, Sao Paulo, Brazil
4 Head and Neck & Plastic Surgeon, Department of Head and Neck Surgery & Otorhinolaryngology, A.C. Camargo Cancer Center, Sao Paulo, Brazil
5 Head and Neck Surgeon, Department of Head and Neck Surgery & Otorhinolaryngology, A.C. Camargo Cancer Center, Sao Paulo, Brazil
6 Medical resident from Department of Head and Neck Surgery & Otorhinolaryngology, A.C. Camargo Cancer Center, Sao Paulo, Brazil
7 Department of Stomatology, A.C. Camargo Cancer Center, Sao Paulo, Brazil
8 Head of Department of Radiation Oncology, A.C. Camargo Cancer Center, Sao Paulo, Brazil
Address correspondence to:
Wilber Edison Bernaola-Paredes
DDS, OMS, MSc., PhD Student, Department of Radiation Oncology, A.C. Camargo Cancer Center, Sao Paulo,
Brazil
Message to Corresponding Author
Article ID: 101308Z01VF2022
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Bella-Filho V, Bernaola-Paredes WE, Filippetti NP, Ramos LF, Rodrigues ML, Vartanian JG, Carvalho HP, Lopes RN, Pellizzon ACA. Refractory advanced osteoradionecrosis (ORN) in the mandible: Analysis of predictive factors, clinical, imaging, and therapeutic characteristics. Int J Case Rep Images 2022;13:101308Z01VF2022.ABSTRACT
Introduction: Osteoradionecrosis (ORN) of the jaws is a late, severe and difficult to manage side effect in patients who underwent radiotherapy (RT) in the head and neck region. Treatment remains controversial, especially in refractory cases that do not respond to multiple attempts with different therapies, due to their complex pathophysiology. It is based on conservative non-surgical approaches, even in large resections using free flaps. The present study aims to present and describe a clinical case of refractory ORN treated through microsurgical reconstruction and adjuvant therapies.
Case Report: A 51-year-old female patient with oncological background of oral squamous cell carcinoma (OSCC) of the floor of the mouth, previously treated with marginal mandibulectomy, and who subsequently relapsed. In a second surgical time, left hemimandibulectomy was performed, followed by microsurgical reconstruction with the fibular osteomusculocutaneous free flap, besides, dental implants were placed in the perioperative time. Radiotherapy was performed using a 3D conformal technique with a total dose of 66 Gy and after six months the patient developed infection in the treated region and it was observed partial exposure of the fibular flap and intra and extraoral purulent drainage, and after imaging analysis the diagnosis of ORN was established. Some non-surgical therapeutic attempts were performed without clinical response and a new surgical approach was performed based on sequestrectomy, the removal of the titanium plaque and dental implants with a second microsurgical reconstruction with forearm fasciocutaneous free flap to cover the soft tissue defect was done.
Conclusion: The pathophysiology of ORN remains controversial and the predictive factors for its appearance, development, and progression are still unclear. Marginal mandibulectomy could be associated with a rapid onset of ORN in patients submitted to adjuvant RT and it could be considered as a potential predictive factor. Combined therapies are reliable alternatives for local control in refractory cases and in advanced stages, and surgical removal with microsurgical reconstruction procedures are still a feasible alternative that has shown satisfactory clinical results.
Keywords: Dental implants, Free tissue flaps, Microsurgery, Oral cavity squamous cell carcinoma, Osteoradionecrosis, Radiotherapy, Segmental mandibulectomy
Introduction
Squamous cell carcinoma (SCC) is ranked the sixth most common malignant tumor worldwide and the most frequent histological subtype that affects the oral cavity (OC), representing approximately 90% of cancers in this region. Its treatment is based on a multimodal approach that includes medium or large surgical resections, radiotherapy (RT), chemotherapy (QT), and their combinations [1],[2],[3].
Surgical removal of tumors, using different techniques, is the primary approach to tumors in OC. For advanced lesions (T3 and T4 stage) in the region of the floor of the mouth, lower gingiva including the mandibular bone, segmental or marginal mandibulectomy, the last one which is the partial removal of compromised bone tissue in order to obtain free margins, are commonly performed, in patients who have undergone or will undergo adjuvant treatment, such as radiotherapy (RT). Marginal mandibulectomy has shown favorable results in local control of the disease; however, it is associated with a higher incidence of late side effects before or after adjuvant RT [1],[4].
Osteoradionecrosis (ORN) is a late and severe complication, which is a challenge to management, in patients undergoing head and neck RT. Osteoradionecrosis is defined as an area of exposed bone that does not heal, may result in bone and/or surrounding tissue necrosis that persists for more than 3–6 months, which could be diagnosed as late as 17 years after being submitted to RT [2],[5],[6]. Frequent symptoms of ORN are chronic pain, trismus, and in advanced stages, an orocutaneous fistulae, with consequent pathological jawbone fracture [7].
There seems to be an association between the appearance and development of ORN and tumor-related factors such as location, size, stage, and presence of bone invasion. In regard to its relationship with RT, it is primarily associated with the total dose delivered, technique and the target volume irradiated; and patient-related factors, such as the use of tobacco/alcohol, oral hygiene, tooth extractions, comorbidities, and possible systemic disorders [7]. However, few studies have described these predictive factors that could act as potential predictors of further occurrence of ORN lesions. Thus, this is based on the treatment planned for the primary tumor, time taken for reconstruction, and rehabilitation after ablative surgery in patients either irradiated previously or not, and dose delivered in cases who underwent marginal and/or segmental mandibulectomy, among other factors [1],[8].
The treatment of ORN remains controversial due to its complex pathophysiology, particularly in refractory cases. Refractory lesions are described as those resistant to multiple therapeutic attempts, whether non-surgical or surgical, the progression of which are accelerated, and their management is difficult to establish. This management will often consist of simultaneous combination of procedures adopted from both the conservative approach to extensive surgical resections with the use of microvascularized free flaps.
The aim of this study was to describe the diagnosis, the management of refractory mandibular ORN, and the potential predictive factors associated with its occurrence in a patient submitted to multimodal treatment for oral squamous cell carcinoma (OSCC).
Case Report
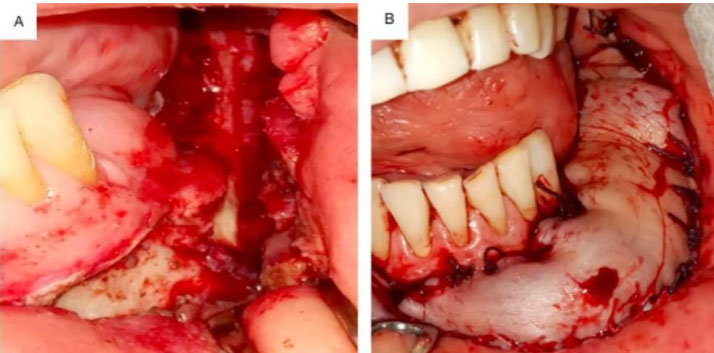
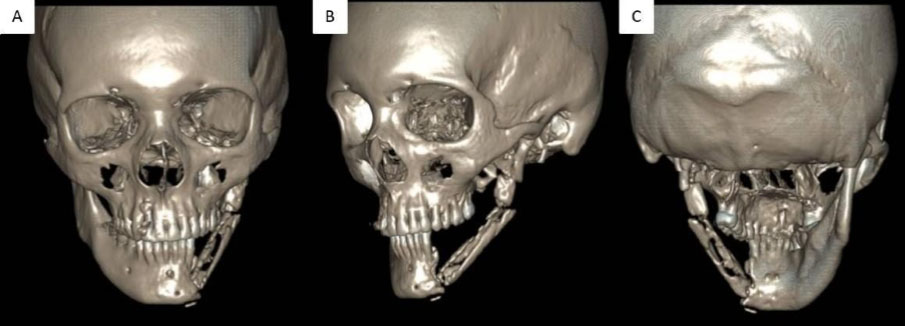
A 51-year-old woman complained of multiple relapses of ulcerated lesions in the left retromolar region, who reported that the last lesion measured approximately 1.5 cm in its major diameter. This lesion was observed on intraoral examination, painful on palpation, and found to be infiltrated into the underlying region. She was submitted to surgical resection that led to the initial diagnosis of OSCC in the lower gingiva. Treatment was based on left marginal hemimandibulectomy with unilateral dissection of SupraOmoHyoid (SOH) neck linfonodal levels (I–III), without free surgical margins, in April 2020. After a new biopsy and confirmation of local recurrence, a left segmental mandibulectomy was performed, followed by microsurgical reconstruction with a fibular osteomusculocutaneous free flap where the dental implants for further oral rehabilitation were placed during the same surgical time. Moreover, RT was performed using the 3D conformal technique with a dose of 66 Gy delivered in the tumor bed and 50 Gy in high-risk drainage regions. After six months, the patient developed an infection in the remnant tumor bed. This was treated and a partial exposure of fibular free flap, intraoral purulent drainage and orocutaneous fistulae were observed (Figure 1). Moreover, the imaging analysis showed an extensive mixed osteolytic lesion with small areas of necrotic bone sequestra that confirmed the diagnosis of advanced mandibular ORN (Figure 2). At first, the therapeutic protocol based on non-surgical therapy with a broad-spectrum antibiotic therapy was indicated after microbiological analysis, besides, the antifibrotic therapy with pentoxifylline and tocopherol (PENTO), and 30 sessions of hyperbaric oxygen therapy (HBOT) were performed.
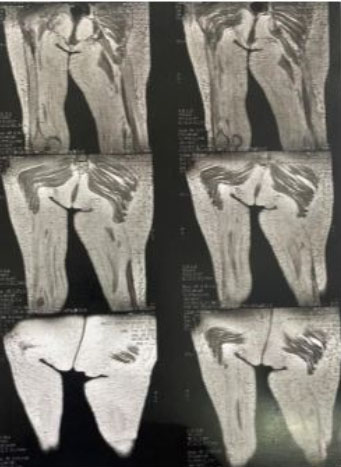
In view of the persistent and refractory clinical behavior with greater bone exposure and loss of surrounding soft tissue, confirming the failure of the above-mentioned therapies, the proposal was to remove the dental implants, titanium plate, devitalized bone, and compromised fibular free flap. Finally, the new microsurgical reconstruction was performed using a forearm free flap (Figure 3 and Figure 4). Seven days and three months of follow-up showed a clinical stability of the flap assessed by intraoral and imaging evaluations as shown in Figure 5 and Figure 6 respectively.




Discussion
Several hypotheses have been proposed for a better understanding of the pathophysiology of ORN. The most accepted theory was proposed by Marx, in 1983, with regard to hypoxia, hypocellularity, and hypovascularity in the bone microenvironment as being the primary etiological factors for development of ORN. The mandible is more affected when compared with the maxilla and other bone structures in the head and neck region, such as the hyoid, temporal bone, among others [5].
A recent study published by Iqbal et al. found that there was a high risk of developing ORN after a mean radiation dose of 57.3 Gy delivered in patients who had undergone head and neck RT. This finding was similar to the results shown by Shaw et al., who associated a mean radiation dose of 57.4 Gy received in this region with the occurrence of this late side effect of RT [8].
More sophisticated RT techniques such as intensity modulated radiotherapy (IMRT) or volumetric arc therapy (VMAT) have shown a lower incidence of ORN compared with traditional techniques such as 3D conformal technique. The difference between techniques lies in the ability to concentrate the high dose of radiation around the primary tumor and away from the mandible and salivary glands, with less exposure of these structures to ionizing radiation. It was demonstrated that the limitation of doses delivered to salivary glands has been demonstrated to be a fact that would lead to a decrease in the rates of xerostomia—as an immediate side effect—and subsequent development of ORN [2],[8].
Regarding the surgical technique used in the primary approach to the tumor involving the mandibular bone, marginal mandibulectomy could be associated with greater damage to the blood supply. This would cause direct side effect on the normal flow of the inferior alveolar artery, and indirectly by removal of the periosteum that interferes with the blood supply of the anterior facial artery. Furthermore, ischemic necrosis also results from radiation-induced obliteration of the inferior alveolar artery [1]. In this case, several local and external factors are associated, which would be considered predictive for the progression of ORN lesions in a narrow period of time. Among these are the primary surgical technique performed with marginal mandibulectomy in the jawbone that would later be irradiated, with a dose greater than 50 Gy, and the placement of dental implants in the perioperative time during the reconstructive microsurgery. Although there is still no consensus in the literature about the better time for dental implants to be placed after RT, the recommendation has been to wait for intervals of 6–12 months after RT [9],[10].
The case presented in this report has shown the refractory behavior of ORN with reference to multiple therapies, and even their association with the first time of primary treatment. In fact, it is a challenge to understand the pathophysiology of ORN and the best option for management. The non-surgical management was established with antifibrotic therapies such as the PENTO protocol and HBOT sessions associated with a superficial debridement of the lesion that did not lead to complete or partial resolution of the clinical condition. The removal of implants and a new microsurgical reconstruction were mandatory for control of the local infection and to prevent further complications such as pathological jawbone fracture.
With no consensus in literature, further studies are necessary to elucidate risk and predictive factors such as the type of surgical technique in primary OSCC tumors, local agents, the time for dental implant placements, and enhanced reconstructive surgery.
Conclusion
The pathophysiology of ORN continues to be controversial and the potential predictive factors for its occurrence, development, and progression are still unclear. Marginal mandibulectomy performed as primary surgical technique should be evaluated in order to clarify its role as potential risk factor of occurrence of this condition in patients that will undergo RT. Combined therapies appeared to be a reliable alternative for local control in refractory cases and in advanced stages, and surgical removal with microsurgical reconstruction procedures are still a feasible alternative that has shown satisfactory clinical results.
REFERENCES
1.
Gou L, Yang W, Qiao X, et al. Marginal or segmental mandibulectomy: Treatment modality selection for oral cancer: A systematic review and meta-analysis. Int J Oral Maxillofac Surg 2018;47(1):1–10. [CrossRef]
[Pubmed]

2.
Yang JY, Hwang DS, Kim UK. Sequential treatment from mandibulectomy to reconstruction on mandibular oral cancer – Case review II: Mandibular anterior and the floor of the mouth lesion of basaloid squamous cell carcinoma and clear cell odontogenic carcinoma. J Korean Assoc Oral Maxillofac Surg 2021;47(3):216–23. [CrossRef]
[Pubmed]
3.
Farhoud Z, Bozorgchenani S. The role of immunotherapy in eliminating high-risk treatments for pediatric cancer. Journal of Current Biomedical Reports 2021;2(2):51–5. [CrossRef]
4.
Wang CC, Cheng MH, Hao SP, Wu CC, Huang SS. Osteoradionecrosis with combined mandibulotomy and marginal mandibulectomy. Laryngoscope 2005;115(11):1963–7. [CrossRef]
[Pubmed]
5.
Haroun K, Coblens OM. Reconstruction of the mandible for osteoradionecrosis. Curr Opin Otolaryngol Head Neck Surg 2019;27(5):401–6. [CrossRef]
[Pubmed]
6.
Bernaola-Paredes WE, Veronese HRM, Filho VB, Martins IS, Pellizzon ACA. Conservative management of advanced mandibular osteoradionecrosis with mild clinical presentation after 17 years of oncological treatment: A case report. Int J Case Rep Images 2021;12:101206Z01WP2021. [CrossRef]
7.
Renda L, Tsai TY, Huang JJ, et al. A nomogram to predict osteoradionecrosis in oral cancer after marginal mandibulectomy and radiotherapy. Laryngoscope 2020;130(1):101–7. [CrossRef]
[Pubmed]
8.
Iqbal Z, Kyzas P. Analysis of the critical dose of radiation therapy in the incidence of osteoradionecrosis in head and neck cancer patients: A case series. BDJ Open 2020;6:18. [CrossRef]
[Pubmed]
9.
Fernández E, Morillo V, Salvador M, et al. Hyperbaric oxygen and radiation therapy: A review. Clin Transl Oncol 2021;23(6):1047–53. [CrossRef]
[Pubmed]
10.
Ettl T, Weindler J, Gosau M, et al. Impact of radiotherapy on implant-based prosthetic rehabilitation in patients with head and neck cancer: A prospective observational study on implant survival and quality of life—Preliminary results. J Craniomaxillofac Surg 2016;44(9):1453–62. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Acknowledgments
The authors thank D.M.C. Company, NUPEN Research Institute and Professor Luciana Almeida from Sao Carlos, Sao Paulo, Brazil and their teams who supported this work with full resources for applying photobiomodulation and antimicrobial Photodynamic Therapy (aPDT). Wilber E. Bernaola-Paredes is a student fellow and supported with a scholarship provided by the National Council for Scientific and Technological Development of Brazil (CNPq), Sao Paulo, Brazil (140071/2019-9).
Author ContributionsValdener Bella-Filho - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Wilber Edison Bernaola-Paredes - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Nicholas Pascuotte Filippetti - Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Leonardo Faria Ramos - Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Monica Lucia Rodrigues - Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
José Guilherme Vartanian - Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Henrique Perez Carvalho - Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Rodrigo Nascimento Lopes - Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Antonio Cassio Assis Pellizzon - Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2022 Valdener Bella-Filho et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}