 |
Case Report
The full breast ultrasonography usefulness in the diagnosis of a bicentric breast cancer – An anatomical imaging approach correlated with the pathological findings: A case report
1 Pan Med Laboratories, No 9 Calea Bucuresti Street, Bl. U1, Craiova, Dolj, Romania
2 Prima Medical Med Life, Calea Bucuresti Street, No 99, Craiova, Dolj, Romania; Former senior radiologist at the Emergency County Clinical Hospital in Craiova, Dolj, Romania
Address correspondence to:
Aristida Colan-Georges
Bibescu Street No 29, Bl. P6, Ap.4, Craiova, Dolj, 200375,
Romania
Message to Corresponding Author
Article ID: 101243Z01AC2021
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Colan-Georges A. The full breast ultrasonography usefulness in the diagnosis of a bicentric breast cancer – An anatomical imaging approach correlated with the pathological findings: A case report. Int J Case Rep Images 2021;12:101243Z01AC2021.ABSTRACT
Introduction: The classification of multiple, simultaneous, ipsilateral breast cancer after localization in arbitrarily delimited quadrants, according to BI-RADS criteria, is in disagreement with pathological and cytogenetic investigations and with the evolution of the disease. This classification is related to the non-anatomical examination in two standard mammographic projections, including tomosynthesis, and to the non-anatomical orthogonal scanning in the classical ultrasonography and magnetic resonance imaging of the breasts.
Case Report: We illustrate a case of a 69-year-old woman with multicentric breast cancer detected and characterized by a non-invasive technique of diagnosis, based on the triad: anatomical ductal radial and antiradial breast ultrasound, Doppler study and strain sonoelastography, briefly named the full breast ultrasonography.
Conclusion: The complete technique of ultrasonography has the advantages of high availability, low costs, standardization of scanning and reporting, and especially a detailed imaging illustration of the breast anatomical normal and abnormal structures correlated with the pathological findings.
Keywords: Breast cancer, Multicentric cancer, Multifocal cancer, Strain sonoelastography, Ultrasonography
Introduction
Concomitant multiple mass-type breast cancers (BCs) could be classified according to their location and composition into two categories: the multicentric cancers, either bilateral or ipsilateral but with different histological and cytogenetic compositions, and multifocal cancers when the masses/nodules are located in the ipsilateral breast and usually have the same composition, representing monoclonal tumors. Multifocal cancers are interpreted by some authors as intralobar dissemination of malignant cells following the lowest intraductal pressure, and could be considered intralobar metastases, with a larger tumor associated with smaller foci of decreasing size as the distance from the main tumor is enlarged. The pathologists consider there is very low probability that all independent foci happen to inactivate the same allele of the X-chromosome-linked phosphoglycerokinase (PGK) gene [1]; moreover, other pathologists found an association between the proximity of the foci and their likelihood that were karyotypically related [2]. In addition to the migration process, it was demonstrated that cancer cells could secret specific factors that are sufficient to induce cancerous transformation of normal epithelial mammary cells [3], and both mechanisms are favorable to develop a multifocal cancer inside a lobar ductal-lobular tree. The BC metastases are unlikely in other mammary lobes. When a different mass with malignant descriptors is found in a distant mammary lobe, the highest probability is represented by other types of cancer, i.e., by multicentric, multiclonal malignant tumors.
The precise pretherapeutic differential diagnosis of multicentric or multifocal type is important because the extension of the disease and, consequently, the staging and the treatment are different and the long-term outlook is changed. The multifocal staging is based on the size of the largest tumors, but it is considered the risk of lymph node metastases and the risk of recurrence to be greater than for unifocal cancers. Moreover, some rare cancers have multiple subtypes within the same tumor, which complicates the diagnosis and the treatment [4].
The radiological-imaging diagnosis in the worldwide practice is standardized by the BI-RADS 5th edition (2013), and the multiple BCs are defined as multifocal if located in the same quadrant, and multicentric if the lesions are located in different quadrants [5]. This arbitrary assessment is illogical and inaccurate, simplified because of the mammographic standard views and of the orthogonal scanning in the classical breast ultrasonography (US) and magnetic resonance imaging (MRI) practice, but there is not a correlation with the breast anatomy, or with the pathological reports.
The incidence of the multiple BCs has a wide variation among the clinical studies because of lack of standardization [6]. Magnetic resonance imaging is considered the best technique of diagnosis of multiple BCs, which was detected in 14–30% cases [6]. However, multiple cancers were found in 40% cases diagnosed by full breast ultrasonography (FBU) of a series of 1841 examinations in 1333 patients, confirmed by other imaging techniques or after surgical treatment with histopathological examination [7]. This result is according with a pathological report of a series of 1000 cases, examined by the use of the large-pathological sections, which established by combining in situ and invasive breast tumors, three “aggregate growth patterns”: unifocal (36%), multifocal (35%), and diffuse (28%) [8].
The value of the FBU is represented by the high resolution of the radial scanning examination of the whole breast volume, following the ductal-lobular tree of the mammary lobes that are disposed radially around the nipple; this technique offers a sensitivity close to 100%, and a specificity over 95–98% [7], as a result of combining 2D ultrasound data (that illustrates both the descriptors specified by the US BI-RADS system and the intralobar ductal connection), with Doppler analysis of the salient vasculature and strain sonoelastography (SSE) [9]. The normal galactophorous ducts may be detected using actual transducers from a thin diameter of 0.4 mm, representing the atrophied ducts, up to 3.0 mm in young women or at puberty; the normal lobules have a comparable size. Thus, FBU can illustrate any abnormal ductal-lobular changes that except the aspect of the background parenchyma, and the suspect findings could be detected in their first 5 mm size.
Case Report
We present a case of a 69-year-old woman who was referred in March 2020 for diagnosis of a new painless nodule located in the upper outer quadrant of the right breast, detected by self-palpation. The patient had a history of another benign nodule in her left breast, detected for the first time 23 years earlier, that was stationary at control examinations.
We applied a FBU using an ultrasound platform E8 Expert (GE Healthcare, Tiefenbach, Austria), provided with 3D/4D, Doppler color, power and spectral, and real-time SSE. The linear transducer ML 6–13 MHz had an intermediary length of 5 cm, but with a virtual convex-trapezoid view useful for the radial scanning especially in large breasts. The Doppler sensitivity was improved by using in addition to the menu “Breast” the “Nearfield” menu that was more sensitive for detecting the vessels of lower velocities, and we completed the US BI-RADS descriptors with the incident angle of the plunging artery upon Kujiraoka et al. [10], as the most specific descriptor for malignant masses [7]. The SSE results were classified upon the Ueno/Tsukuba scoring as a complementary technique [11].
The FBU of the whole breast volume upon the clockwise notation illustrated the breasts with predominantly fatty composition of climax-type, with proportional glandular atrophy of the stroma and parenchyma in all quadrants, with the galactophorous ducts of an average diameter below 1 mm, and the lobules involved, immeasurable. The background vascularization explored by color Doppler was physiologically reduced.
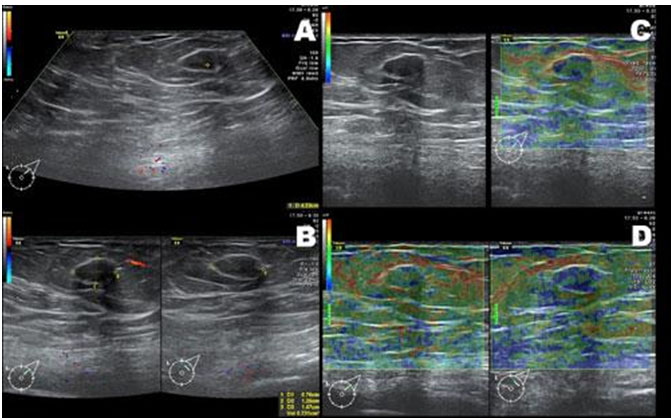
The left breast presented at 1:30 and 4 cm away from the nipple, a well-defined hypoechoic nodule, apparently developed inside a Cooper ligament which it widened, ovoid in shape, with a multi-lobulated contour, benign posterior acoustic effects, a benign peripheral vascular pole, the diameters 7.6×12.5×14.7 mm with an estimated volume 0.73 cm3, and repeated SSE score 2 and 3 Ueno within benign limits, suggesting fibroadenoma appearance (Figure 1). We identified small retroareolar ductal-ampullary ectasias within benign aspects, usually considered by pathologists as physiologic findings in postmenopausal women, with transonic appearance and sketch of summation-type blue-green-red (BGR) score. There were no other solid nodules or other suspicious lesions in the left breast. The left axillary lymph nodes presented the transverse diameter up to 8.2 mm, normal cortex and vascularization, slight changes of reactive histiocytosis in the sinus with hypoechoic aspect and SSE of score 2 Ueno.
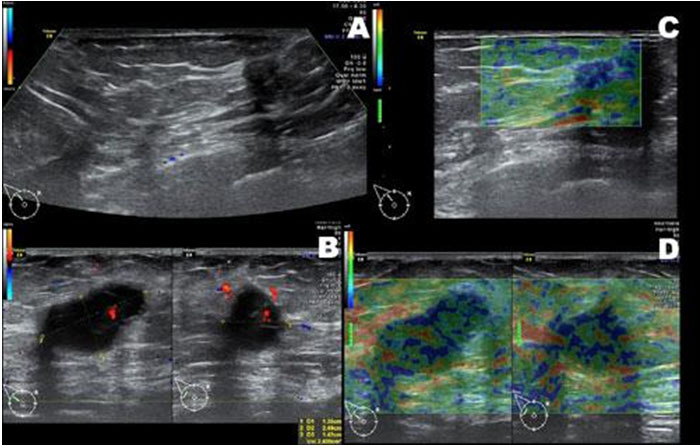
The right breast, with a similar background structure, presented at 10:00 peripherally, in the axillary extension of the gland (Spencer tail), corresponding to the new lump, an intense hypoechoic mass, well delimited, with a poly-lobulated contour, apparent transonic content with septa, benign posterior acoustic effects, of 13.5 × 24.9 × 14.0 mm size and an estimated volume of 2.5 cm3. The peripheral and internal multipolar vasculature demonstrated an incident angle of malignant type and the SSE scoring was 3–4 Ueno with some BGR areas, aspect suggesting a rare type of breast carcinoma, including a mucinous-type, an aggressive cancer with internal necrosis and without peripheral stromal reaction or an intra-cystic carcinoma. In addition, tumor vasculature with aliasing and high-resistance flow strengthened the suspicion of malignant breast lesion (Figure 2).
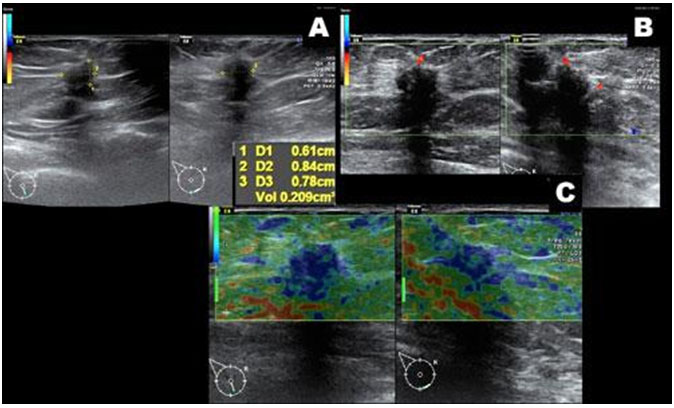
At 5:30 in the sub-mammary sulcus it was identified other unexpected, “silent” hypoechoic mass, impalpable with angular margins, located along a Cooper ligament, with acoustic shadowing, inhomogeneous, sized 6.0 × 8.4 × 7.8 mm with an estimated volume of 0.21 cm3, SSE of score 5 Ueno, and peripheral tripolar vessels with incident angle, with the appearance of a typical malignant nodule (Figure 3). The right axillary lymph nodes had transverse diameter up to 10.4 mm, with normal cortex and vasculature in hilum, associated with changes of reactive histiocytosis in the sinus and scored 2 Ueno, within benign limits. There were no lymphadenopathies along the right external thoracic artery, internal mammary arteries, and supra- or sub-clavicular fossae.
The conclusion of the examination was: “Right multicentric breast cancer with a first mass at 10:00 peripheral, of rare carcinoma type with 2.5 cm diameter and a second nodule in the sub-mammary sulcus at 5:30 of 0.8 cm diameter, with the appearance of invasive ductal carcinoma (IDC). No satellite lymphadenopathy detected, US BI-RADS assessment 5 category.”
The recommendation for oncological examination with targeted tru-cut biopsies was followed by a pathological and immunohistochemical report, which described two different types of malignancies:
- the R 10:00 mass had the diagnosis of moderate differentiate IDC (G2), ER+ over 85%, PR+ 70–75%, Her2-;
- the mass of the sub-mammary sulcus at 5:30 represented a low differentiated IDC (G3), with medullary component, ER+ 5–6%, PR-, Her2-.
The neoadjuvant chemotherapy and hormonal therapy were followed by the modified radical mastectomy type Madden after a month. The biological tests and a preoperative multidetector contrast computed tomography (CT) had not significant pathological results, except for the cancer antigen CA 15-3, in slight progression, but considered within benign limits after a surgical approach: 18.63 U/mL before the surgical treatment and 39.05 U/mL one month after mastectomy (the reference range was less 30 U/mL).
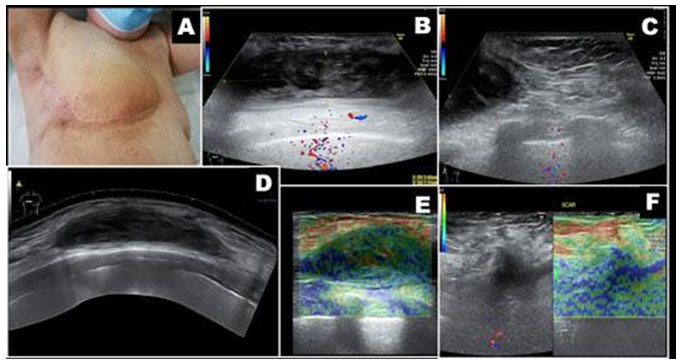
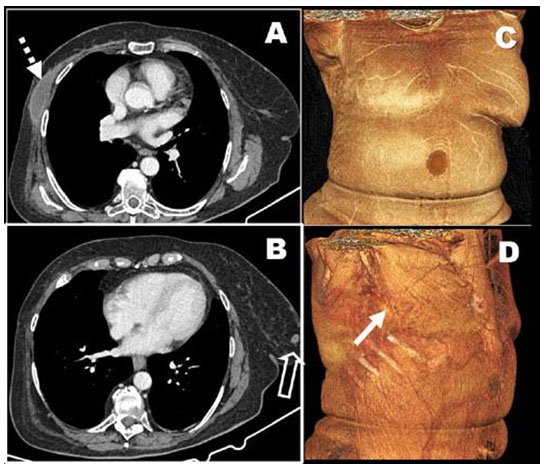
The postoperative evolution had a slow healing, marked by inflammatory phenomena and the formation of a hematoma in the area of the surgical bed, demonstrated by targeted classical US in the same surgical service. The heterogeneous collection was recurrent after puncture and drainage (insufficient) and under anti-inflammatory and antibiotic therapy. The FBU follow-up examination in our service of 6 months post-mastectomy was recommended for persistent skin redness, tenderness, and edema. The FBU illustrated a status post incomplete right mastectomy with peripheral remnant glandular tissue with specific stroma and atrophied galactophorous ducts, skin thickening around the surgical scar up to 3.6 mm (normal skin areas thickness of 2 mm), edema of the subcutaneous fatty tissue with a hyperechoic aspect as compared with the normal areas, and a chronic retro-pectoral hematoma of 24.65 cm3, unexpected, probably produced after incorrect insertion of the initial surgical drainage tube by counter-incision (a usual—and illogical!—insertion of a drain for a non-anatomical pre-existing cavity, but in the surgical practice for both conservative breast resection and radical mastectomy) (Figure 4). Due to apparent reduced initial drainage, the (inefficient) tube was early removed, with further local inflammatory changes.
The control multidetector contrast CT scan confirmed the location under the great pectoral muscle of the heterogeneous hypodense mass, without contrast enhancement, which could justify the slow healing (Figure 5). No remnant tumor was identified in both FBU and CT and no distant metastases were radiologically detected. The evolution was finally favorable under correct surgical drainage and anti-inflammatory treatment, in addition to chemotherapy and adjuvant hormone therapy.
Discussion
This case presented falls within the BI-RADS definition of multicentric cancer, the two lesions being located in different quadrants. However, the definition is arbitrary, because the breast glandular architecture is based on mammary lobes oriented radially around the nipple, which are morphological-functional mammary units and do not communicate (with rare exceptions) but may overlap, as demonstrated the anatomist Cooper since 1840 [12]. They are of unequal size and may be located inside a quadrant or may exceed its limits by extension into two adjacent quadrants. The actual surgical techniques in worldwide use, either conservative or radical, do not respect the lobar anatomy. The conservative techniques of multifocal cancers are simultaneous overtreatment with incomplete excision, because some segments of the healthy adjacent mammary lobes are excised and other segments of the “sick” lobe are preserved following the rule of the surgical safety margins, with high risk of recurrent malignancies. Similarly, in the radical mastectomy for the false considered multicentric breast cancers in adjacent quadrants represents an overtreatment with unnecessary mutilation and risk of surgical complications.
The usual pathological sections are small, centered on the lesion and their limits and do not allow the research of the lobar pathology, nor the relationship between the malignant foci. By consequence, the pathological reports of the multiple foci do not precise the multifocal or multicentric lesions, the extension of the disease is controversial and the interpretation of the resemblances between tumoral clones is ambiguous and with inter-authors disagreements [13]. By contrarily, the “theory of the sick lobe” (the whole lobe presents a genetic defect with benign or malignant risk) of Tot [14] and the pathological analysis of the large radial histological section (“gross section”) [15] are useful for the discrimination of the multifocal cancer (with ductal connection), from the multicentric cancer. There were large-format histological sections that detected 26% of unexpected malignancies otherwise neglected by conventional histology [16].
The best pre-surgical diagnostic technique for simultaneous multiple breast cancer is considered MRI, but it has low availability, high costs, and involves the use of gadolinium-based contrast agents that have a restricted recommendation due to their side-effects, so these contrast agents could not be used in an unlimited screening examination. However, despite the MRI sensitivity (around 81%) is higher than of mammography (60–66%) in detecting the multiple ipsilateral breast cancers, the positive predictive value is low for both techniques, around 70–80% [17], and no specific descriptors could discriminate between multifocal and multicentric cancers. Another technique proposed was the US of the whole breasts upon the classical scanning, which proved significantly increased sensitivity compared with a targeted US, but a low sensitivity of less than 60% reported to the final pathological diagnosis [18].
The radial and antiradial scanning in FBU reassures the non-invasive research of the whole breast anatomy, which includes the age, gender, physiological condition, breast implant, or other previous surgery. The findings are described in anatomical terms, the high resolution allowing a magnification of 3× that could be interpreted according to the “gross pathological section” mentioned above. As a consequence, some conservative surgical techniques were developed, based on the armpit (sentinel) node(s) excision followed by a “précised mammary lobectomy” [19], with esthetical best results, without any mandatory drainage and with reduced risk of tumor recurrences, reported as 0.3% [20], while the 10-years recurrence rate after conservative surgery in early stages of invasive BC is described up to 10–20% [21].
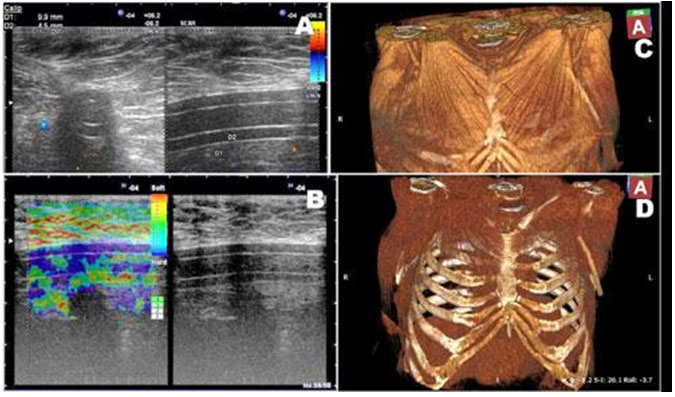
In this case report, post-surgical FBU précised the size and the unexpected location of the heterogeneous collection behind the great pectoral muscle, allowing a correct drainage. In other cases, the FBU technique detected other various post-surgical complications, such as seromas, suture granulomas, remnant breast tumors or remnant normal or pathological axillary lymph nodes, or even a drain tube “forgotten” and partially migrated behind the great pectoral muscle, probably related to its insertion by counter-incision (Figure 6).
Conclusion
The importance of this case report is to illustrate the usefulness of the non-invasive but anatomical FBU in the detection and characterization of multiple ipsilateral breast cancer that presented different descriptors correlated with the grade of cellular differentiation. The late initial presentation of the patient was favored by the absence of an official national screening program of breast cancer in our country, and by the evolution of the case during the first year of Covid-19 pandemic, which disturbed the medical system in most countries. The relatively new method of diagnosis represented by FBU, with high availability in any medical situation, could be helpful as first screening technique for the countries or any population with reduced resources.
REFERENCES
1.
Noguchi S, Aihara T, Koyama H, Motomura K, Inaji H, Imaoka S. Discrimination between multicentric and multifocal carcinomas of the breast through clonal analysis. Cancer 1994;74(3):872–7.
[Pubmed]

2.
Teixeira MR, Pandis N, Bardi G, et al. Discrimination between multicentric and multifocal breast carcinoma by cytogenetic investigation of macroscopically distinct ipsilateral lesions. Genes Chromosomes Cancer 1997;18(3):170–4. [CrossRef]
[Pubmed]
3.
Song L, Jie Z, Hongying W, et al. Oncogenic transformation of normal breast epithelial cells cocultured with cancer cells. Cell Cycle 2018;17(16):202–40. [CrossRef]
[Pubmed]
4.
Yeo SK, Guan JL. Breast cancer: Multiple subtypes within a tumor? Trends Cancer 2017;3(11):753–60. [CrossRef]
[Pubmed]
5.
D'orsi CJ, Sickles CJEA, Mendelson EB, et al. ACR BI-RADS Atlas, Breast Imaging Reporting and Data System. Reston, VA: American College of Radiology; 2013.
6.
Milulescu A, Di Marino L, Peradze N, Toesca A. Management of multifocal-multicentric breast cancer: Current perspective. Chirurgia (Bucur) 2017;112(1):12–7. [CrossRef]
[Pubmed]
7.
Colan-Georges A. Improvements of the US BI-RADS assessment – A necessity for a non-invasive positive and differential diagnosis of breast cancer. Application of the new full breast ultrasonography concept. European Journal of Medical and Health Sciences 2020;2(6). [CrossRef]
8.
Tot T. The role of large-format histopathology in assessing subgross morphological prognostic parameters: A single institution report of 1000 consecutive breast cancer cases. Int J Breast Cancer 2012;2012:395–415. [CrossRef]
[Pubmed]
9.
Colan-Georges A. Sonoelastography in addition to Doppler ductal echography: Full breast ultrasonography. In: Colan-Georges A, editor. Atlas of Full Breast Ultrasonography. 1ed. Switzerland: Springer International Publishing; 2016. p. 53– 65. [Available at: https://www.springer.com/gp/book/9783319314174]
10.
Kujiraoka Y, Ueno E, Tohno E, Morishima I, Tsunoda H. Incident angle of the penetrating artery of breast tumors. In: Ueno E, Shiina T, Kubota M, Sawai K, editors. Research and Development in Breast Ultrasound. Tokyo: Springer-Verlag; 2005. p. 72–5.
11.
Itoh A, Ueno E, Tohno E, et al. Breast disease: Clinical application of US elastography for diagnosis. Radiology 2006;239(2):341–50. [CrossRef]
[Pubmed]
12.
Cooper, Sir Astley Paston. On the anatomy of the breast – Structure of the breast in the human female. In: Sir Astley Paston Cooper. On the Anatomy of the Breast; 1840. Paper 6. [Available at: https://jdc.jefferson.edu/cooper/6]
13.
Wu JM, Turashvili G. A survey of breast pathologists’ practice in staging multiple foci of invasive carcinoma. Clin Breast Cancer 2020;S1526-8209(20)30327-X. [CrossRef]
[Pubmed]
14.
Tot T. The theory of the sick lobe. In: Tot T, editor. Breast Cancer. London: Springer; 2010.
15.
Tot T. Clinical relevance of the distribution of the lesions in 500 consecutive breast cancer cases documented in large-format histologic sections. Cancer 2007;110(11):2551–60. [CrossRef]
[Pubmed]
16.
Foster MR, Harris L, Biesemier KW. Large format histology may aid in the detection of unsuspected pathologic findings of potential clinical significance: A prospective multiyear single institution study. Int J Breast Cancer 2012;2012:532547. [CrossRef]
[Pubmed]
17.
Sardanelli F, Giuseppetti GM, Panizza P, et al. Sensitivity of MRI versus mammography for detecting foci of multifocal, multicentric breast cancer in fatty and dense breasts using the whole-breast pathologic examination as a gold standard. AJR Am J Roentgenol 2004;183(4):1149–57. [CrossRef]
[Pubmed]
18.
Wilkinson LS, Given-Wilson R, Hall T, Potts H, Sharma AK, Smith E. Increasing the diagnosis of multifocal primary breast cancer by the use of bilateral whole-breast ultrasound. Clin Radiol 2005;60(5):573–8. [CrossRef]
[Pubmed]
19.
Dolfin G. The surgical approach of the “Sick Lobe”. In: Francescatti DS, Silverstein MJ, editors. Breast Cancer: A New Era in Management. New York: Springer Science+Business Media; 2014. p. 113–32.
20.
Dolfin G, Botta G. Lobar surgery and pathological correlation. In: Amy D, editor. Lobar Approach to Breast Ultrasound. Cham: Springer; 2018.
21.
Belkacemi Y, Hanna NE, Besnard C, Majdoul S, Gligorov J. Local and regional breast cancer recurrences: Salvage therapy options in the new era of molecular subtypes. Front Oncol 2018;8:112. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Acknowledgments
The author thanks the managers of affiliated private institutions who provided the valuable equipment and offered ongoing encouragement for the conduct of scientific research that was completed through this study.
Author ContributionsAristida Colan-Georges - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthor declares no conflict of interest.
Copyright© 2021 Aristida Colan-Georges. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}