 |
Case Report
Symptomatic abdominal aortic aneurysm: Radiological features and value of ultrasound screening
1 Department of Radiology, University of Abuja, Abuja, Nigeria
2 Department of Radiology, Ahmadu Bello University Teaching Hospital, Zaria, Nigeria
3 Department of Radiology, Abubakar Tafawa Balewa University Teaching Hospital (ATBUTH), Bauchi, Nigeria
Address correspondence to:
Joshua Oluwafemi Aiyekomogbon
Department of Radiology, University of Abuja, Abuja,
Nigeria
Message to Corresponding Author
Article ID: 101242Z01JA2021
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Aiyekomogbon JO, Itanyi DU, Ahmed HM, Halilu SD. Symptomatic abdominal aortic aneurysm: Radiological features and value of ultrasound screening. Int J Case Rep Images 2021;12:101242Z01JA2021.ABSTRACT
Introduction: Aneurysm is dilatation of an artery to 1.5 times its normal diameter as a result of proteolytic degradation of the protein elastin and collagen of the arterial wall. Early diagnosis is imperative to prevent aneurismal rupture which is lethal.
Case Report: An 80-year-old man presented for ultrasonography exam (US) on account of 11 month history of paraumbilical mass and pain. He was a known hypertensive who has not been regular on his anti-hypertensive medications. Physical examination revealed high blood pressure of 170/110 mmHg and thickened peripheral arterial walls. There was also abdominal tenderness and a right paraumbilical mass with a bruit heard over it on auscultation. Abdominal US demonstrated dilated infrarenal abdominal aorta of 5 cm with echogenic mural thrombus noted anteriorly at that level. Computed tomography (CT) and CT-angiography (CTA) corroborated this sonographic diagnosis. He was then slated for surgical repair of the aneurysm but he defaulted on the ground of age.
Conclusion: This case is presented to highlight the basic radiological features of aortic aneurysm and to also re-echo the need for routine US screening in high risk patients in order to prevent the lethal consequences of aneurismal rupture.
Keywords: Abdominal aortic aneurysm, Angiography, Computed tomography, Hypertension, Ultrasound screening
Introduction
Aneurysm is a localized dilation of an artery to 1.5 times its normal diameter [1]. The normal infrarenal aortic diameters in patients older than 50 years are 1.5 cm in women and 1.7 cm in men. By convention, therefore, an infrarenal aorta 3 cm in diameter or larger is considered aneurismal [1]. Proteolytic degradation of the extracellular matrix proteins elastin and collagen of the aortic wall is the primary event in the development of aortic aneurysm. Various proteolytic enzymes, including matrix metalloproteinases, are critical during the degradation and remodeling of the aortic wall [2].
The infrarenal segment of the abdominal aorta is the most common location of the arterial aneurysm [2],[3]. The risk factors include male gender, age greater than 75 years, white race, systemic hypertension, cigarette smoking, family history, and hypercholesterolemia. Commonly known to be a disease of the western world but now increasingly diagnosed in our environment and Africa as a whole [3].
The disease is five times commoner in males and the 10th leading cause of death in white men 65 to 74 years of age in the United States [4]. Ruptured aneurysm is the leading cause of death and it is preventable when US screening is done routinely for the high risk group which is a highly sensitive imaging tool, with sensitivity and specificity approaching 100% and 96%, respectively [5].
This case is presented to increase the index of suspicion among clinicians and highlights the benefits of US screening program for abdominal aortic aneurysm (AAA).
Case Report
M.S. was an 80-year-old man referred by a gastroenterologist to the ultrasound unit of Ahmadu Bello University Teaching Hospital (ABUTH) on account of paraumbilical abdominal mass and abdominal pain of 11 months duration. He was a known hypertensive, diagnosed 20 years prior to presentation. The abdominal mass was insidious in onset and gradually increased in size. It was initially painless but later became painful. The pain was in the central abdomen and occasionally radiated to the back and it did not prevent him from normal activity. There was no vomiting or alteration in bowel habit. No cardiopulmonary, genitourinary, central nervous system or musculoskeletal symptoms of note.
He has been erratic on his antihypertensive drugs since 20 years of diagnosis. He neither smoked cigarette nor drank alcohol and there was no family history of hypertension or sudden death.
On physical examination, he was hypertensive with a blood pressure of 170/110 mmHg and had a thickened peripheral arterial wall. The pulse rate was however normal (80 beats/minute, regular and good volume). There was abdominal tenderness and a right paraumbilical mass with a bruit heard over it. Musculoskeletal system was preserved, and there was no peripheral ulcer or gangrene noted.
A clinical assessment of vascular abdominal mass was made and urgent abdominal US was requested. Ultrasonography revealed a dilated infrarenal abdominal aorta measuring 5.0 cm in maximum anterior-posterior (AP) diameter. The wall was thickened and an echogenic mural thrombus was noted anteriorly, reducing the caliber of the true lumen significantly (Figure 1). There was no ascites or free extraluminal fluid collection seen that could suggest hemoperitoneum. The ultrasound findings necessitated CT-angiography of the thoracic and abdominal aorta.
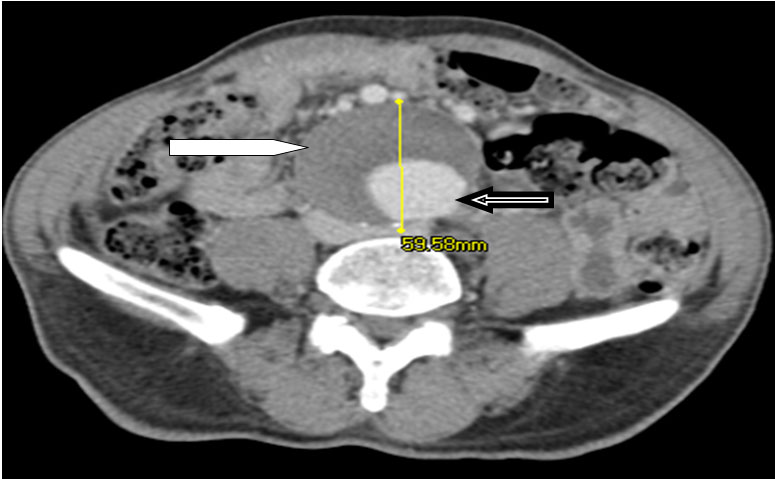
The chest CT-scanogram revealed moderate cardiomegaly of left ventricular preponderance (CTR = 0.66), and the aorta was elongated with prominence of the knuckle but the lung fields were clear (Figure 2). The computed tomography (CT) and CT-angiography of the abdominal aorta revealed a fusiform dilatation of the infrarenal aorta and the right common iliac artery. Hypodense mural thrombus was noted anteriorly (Figure 3), confirming the US findings. Multiple hyperdense lesions of varying sizes and shapes, connoting calcifications, were noted on the walls of the aorta and the common iliac arteries (Figure 4). No aortic dissection or free peritoneal fluid collection was noted.
Radiological diagnosis of infrarenal abdominal aortic aneurysm with hypertensive heart disease was made.
The management of abdominal aortic aneurysm requires multi-disciplinary approach, involving interventional radiologist, cardiologist, and cardiopulmonary surgeons. The management of the index case was planned along this line but he refused surgical management on account of his age while he complied fully with medical care. All attempts made at persuading him for possible surgical management proved abortive, aimed at averting aneurysm rupture.



Discussion
Abdominal aortic aneurysm (AAA) may not be symptomatic prior to the occurrence of a life-threatening event [4],[5]. The aorta is elastic, which allows it to be filled with blood under high pressure and when it becomes weakened and distended, aneurysm can easily develop [4],[5].
Approximately 90% of abdominal aortic aneurysms are located infrarenally which was our observation in our study, but they can also be pararenal (at the levels of the kidneys) or suprarenal in location [6].
Most cases of aneurysms are asymptomatic but some can become painful with associated pulsating sensation particularly when they are large. Such pains could be experienced in the chest, lower back and scrotum in patients with AAA [7]. Some may present with hypovoleamic shock if the aneurysm ruptures. Abdominal mass and vague abdominal pains were the presenting symptoms in this 80-year-old man. The complications include rupture, peripheral embolization, acute aortic occlusion, and aortocaval or aortoduodenal fistulae [4],[5],[6] but none of these complications were noted in the index patient.
Ethnicity and racial influence are major issues to consider in AAA. In the United Kingdom, for instance, the prevalence of AAA in Caucasian men older than 65 years is about 4.7% while it is 0.45% in Asian men with similar demographics [8]. It is also uncommon in individuals of African heritage [3]. But in the United States, 15,000 deaths from AAA are recorded yearly, being one of the countries with the highest prevalence [9].
The diagnosis is usually made by physical examination, ultrasound, and CT scan [10]. Abdominal masses should be examined clinically to look for bruit or pulsation, as AAA can present as an abdominal mass. Plain radiograph may show the outline of an aneurysm when its walls are calcified. However, this is the case in less than half of all aneurysms [10] and plain radiograph done in the index case did not reveal this. Ultrasonography which is readily available and patient’s friendly is therefore used to screen for aneurysm and to determine its size if present and many clinicians in our setting have not appreciated its relevance in this regards [8],[10]. The sensitivity of CT scan in the detection of AAA is nearly 100% and it is also useful in preoperative planning for endovascular repair [10]. Alternative less often used methods for visualization of AAA include magnetic resonance imaging (MRI) and angiography.
The abdominal aorta normally tapers as it extends distally. Any increase in diameter is therefore considered aneurysmal. The dimension, wall thickening, and mural thrombus are well appreciated on US. The echogenicity of the mural thrombus depends largely on its chronicity. In this patient the mural thrombus was echogenic, as it is probably a long standing thrombus.
Pre-contrast CT scanning accurately demonstrates dilation of the aorta and involvement of major branch vessels proximally and distally. Hyperdense patchy lesions with Hounsfield unit ranging from 200 to 400, connoting calcifications, may be noted on the walls of the aorta and iliac vessels, which was our observation in the index case. The location and number of the renal arteries, caliber of the aneurysms, and presence of mural thrombus are readily assessed. Computed tomography angiography allows multiplanar assessment of the aneurysm and associated relevant vessels (visceral arteries, iliac and femoral arteries). The relationship of the aneurysmal segment of the aorta to the renal arteries is usually well demonstrated. Three-dimensional reconstruction of state-of-the-art, multidetector-row, helical CT scans can help in preoperative planning and may replace preoperative diagnostic angiography. In view of all the enumerated advantages of CT scan, it has emerged as the diagnostic imaging standard for the evaluation of abdominal aortic aneurysm, with an accuracy that approaches 100% [10]. That explained why the diagnosis of AAA was easily confirmed on CT in the index case.
Conventional angiography enables better longitudinal measurements of aneurysms. The reason is that catheters that are used to make these measurements are radio-opaque and follow the contour of the vessels and therefore allows better determination of the length of the aneurysm, as opposed to linear measurements obtained with CT [11]. This information is not an issue in open surgical repair; however, it is important in endovascular repair. This attribute is important for endograft placement, and may not be clear from CT and CTA [11]. Angiography is often linked to embolization of the internal iliac artery in a patient in whom the procedure is necessary prior to endovascular repair [11].
Asymptomatic AAA is managed conservatively in the first instance. For symptomatic cases; however, close surveillance with a view of eventual repair is advocated. Open aneurysm repair (OR) and endovascular aneurysm repair (EVAR) are the possible modes of such repairs. A radiological intervention is usually recommended if the growth rate exceeds 1 cm per year or the aneurysm is bigger than 5.5 cm [11]. No medical therapy has been found effective at decreasing the growth rate of asymptomatic AAAs [11]. However, blood pressure and lipids should be treated like any atherosclerotic condition [12]. Treatment with angiotensin converting enzyme inhibitors, beta-blockers, and statin has been advocated but this plays limited roles in the definitive management of AAAs [12].
Treatment of hypertension, smoking cessation, low-fat diet and screening abdominal US for men older than 65 years are measures taken to prevent AAAs. Patients with an aortic diameter of 3.0–4.4 cm should be assessed sonographically at yearly intervals, whereas those with an aortic diameter of 4.5–5.4 cm should be rescanned at 3-monthly intervals [13],[14],[15]. In the United Kingdom, screening is expected to be offered to all men in England in their 65th year. Analysis of the 10 year Multicenter Aneurysm Screening Study data shows that the AAA US screening program will prevent significant numbers of AAA ruptures and AAA deaths [13]. This policy should be adopted in Nigeria and Africa as a whole, as the incidence of aortic aneurysm is on the increase here.
Conclusion
In conclusion, therefore, a case of abdominal aortic aneurysm diagnosed by US, CT, and CTA has been presented. The radiological features and the need for routine US screening have also been stressed, aimed at preventing unwarranted complication of aneurysm rupture which is lethal.
REFERENCES
1.
Lederle FA, Johnson GR, Wilson SE, et al. Relationship of age, gender, race, and body size to infrarenal aortic diameter. The Aneurysm Detection And Management (Adam) Veterans Affairs Cooperative Study Investigators. J Vasc Surg 1997;26(4):595–601. [CrossRef]
[Pubmed]

2.
Wassef M, Baxter BT, Chisholin RL, et al. Pathogenesis of abdominal aortic aneurysms: A multidisciplinary research program supported by the National Heart, Lung, and Blood Institute. J Vasc Surg 2001;34(4):730–8. [CrossRef]
[Pubmed]
3.
Akinola RA, Soeze PO. Aortic aneurysm in a young Nigerian man. Niger Postgrad Med J 2007;14(3):269–71.
[Pubmed]
4.
Anderson RN. Deaths: Leading causes for 2000. Natl Vital Stat Rep 2002;50(16):1–85.
[Pubmed]
5.
Kent KC, Zwolak RM, Jaff MR, et al. Screening for abdominal aortic aneurysm: A consensus statement. J Vasc Surg 2004;39(1):267–9. [CrossRef]
[Pubmed]
6.
Upchurch GR Jr, Schaub TA. Abdominal aortic aneurysm. Am Fam Physician 2006;73(7):1198–204.
[Pubmed]
7.
Creager MA, Loscalzo J. Chapter 274. Diseases of the aorta. In: Jameson JL, Fauci AS, Kasper DL, Hauser SL, Longo DL, Loscalzo J, editors. Harrison’s Principles of Internal Medicine. 20ed. USA: McGraw-Hill Professional; 2018.
8.
Salem MK, Rayt HS, Hussey G, et al. Should Asian men be included in abdominal aortic aneurysm screening programmes? Eur J Vasc Endovasc Surg 2009;38(6):748–9. [CrossRef]
[Pubmed]
9.
Creager MA, Halpern JL, Whittemore AD. Aneurysmal disease of the aorta and its branches. In: Loscalzo J, Creager MA, Dzau VJ, editors. Vascular Medicine. New York: Little Brown; 1996. p. 901.
10.
Tan W, Powell S, Nanjundappa A. Abdominal aortic aneurysm rupture imaging. In: Lin EC, Coombs BD, Gay SB, editors. Medscape Reference. Updated March 31, 2016.
11.
Ballard DJ, Filardo G, Fowkes G, Powell JT. Surgery for small asymptomatic abdominal aortic aneurysms. Cochrane Database Syst Rev 2008;4:1835-7. [CrossRef]
[Pubmed]
12.
Hackam DG, Thiruchelvam D, Redelmeier DA. Angiotensin-converting enzyme inhibitors and aortic rupture: A population-based case-control study. Lancet 2006;368(9536);659–65. [CrossRef]
[Pubmed]
13.
Thompson SG, Ashton HA, Gao L, Scott RAP; Multicentre Aneurysm Screening Study Group. Screening men for abdominal aortic aneurysym: 10 year mortality and cost effectiveness results from the randomized multicentre aneurysm screening study. BMJ 2009;338:b2307. [CrossRef]
[Pubmed]
14.
Kent KC. Clinical practice. Abdominal aortic aneurysms. N Engl J Med 2014;371(22):2101–8. [CrossRef]
[Pubmed]
15.
Abdominal Aortic Aneurysms (AAA). In: Clinical Guidelines: Vascular Arterial Disease (PVD) Imaging Guidelines. Version 1.0. January 2021. eviCore healthcare, SC, p. 28.
SUPPORTING INFORMATION
Author Contributions
Joshua Oluwafemi Aiyekomogbon - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Dorothy Ukamaka Itanyi - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Hamza Mustapha Ahmed - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Solomon Daniel Halilu - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2021 Joshua Oluwafemi Aiyekomogbon et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}