 |
Case Report
Multimodal treatment of atypical transformation of pleomorphic adenoma (PA) of the lacrimal gland into high-grade ductal carcinoma
1 PhD Student, Department of Radiation Oncology, A.C. Camargo Cancer Center, Sao Paulo, Brazil
2 DDS, Master Candidate, Department of Radiation Oncology, A.C. Camargo Cancer Center, Sao Paulo, Brazil
3 Resident of Department of Head and Neck Surgery and Otorhinolaryngology, A.C. Camargo Cancer Center, Sao Paulo, Brazil
4 Resident of Department of Radiation Oncology, A.C. Camargo Cancer Center, Sao Paulo, Brazil
5 Resident of Department of Anatomic Pathology, A.C. Camargo Cancer Center, Sao Paulo, Brazil
6 Researcher/PhD Holder, Department of Anatomic Pathology, A.C. Camargo Cancer Center, Sao Paulo, Brazil
7 Head of Department of Radiation Oncology, A.C. Camargo Cancer Center, Sao Paulo, Brazil
Address correspondence to:
Wilber E Bernaola-Paredes
Rua Prof. Antonio Prudente 211 – Liberdade, São Paulo, ZIP Code: 01509001,
Brazil
Message to Corresponding Author
Article ID: 101232Z01WP2021
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Bernaola-Paredes WE, Filho VB, Carvalho HP, Chen FK, Dalcin JF, Costa FD, Pellizzon ACA. Multimodal treatment of atypical transformation of pleomorphic adenoma (PA) of the lacrimal gland into high-grade ductal carcinoma. Int J Case Rep Images 2021;12:101232Z01WP2021.ABSTRACT
Introduction: Pleomorphic adenoma (PA) is a tumor with a mix of components (epithelium-mesenchymal). It occurs more frequently in both the larger and smaller salivary glands, and less frequently in the lacrimal glands. The transformation of PA into high-grade Ductal carcinoma involves a series of histopathological, morphological, and molecular mechanisms, so that its occurrence is rare, nevertheless, the mortality rate is still high. Surgery in conjunction with adjuvant radiotherapy has been shown to be effective in locoregional disease control (LDS); however, the multimodal treatment indicated in the literature remains a controversial issue.
Case Report: The present case report aims to describe our experience with the multimodal treatment of an atypical presentation of transformation of PA of the lacrimal gland into a rapidly evolving high-grade ductal carcinoma, and to describe the proposed adjuvant radiation treatment.
Conclusion: Adjuvant radiotherapy is a feasible alternative for locoregional control of the disease, irrespective of the anatomopathologic characteristics of the tumor. Randomized clinical trial studies are recommended for an accurate assessment of the impact of multimodal treatment with respect to overall survival rates, locoregional survival, and disease-free survival.
Keywords: Adjuvant radiotherapy, Lacrimal gland, Malignant transformation, Mixed, Pleomorphic adenoma, Salivary gland tumor
Introduction
Pleomorphic adenoma (PA) is one of the most common neoplasms with a mixed composition (epithelial and mesenchymal) and like most epithelial neoplasms of the salivary glands; it also affects the lacrimal glands. This benign neoplasm usually appears between the third and fourth decades of life, with no gender predilection, and the rate of clinical success increases considerably after appropriate surgical treatment, resulting in lower recurrence rates and potential for malignancy. The malignant transformation of this neoplasm is rare, and when it does occur, it becomes locally aggressive and the prognosis will depend on the number of myoepithelial cells present, degree of hyalinization, and extension of the tumor beyond the capsular region of the primary PA [1],[2]. Malignant transformations of PA represent 10% of neoplasms that affect the lacrimal glands, and the clinical results will depend mainly on the type and degree of malignancy of the oncocytic tumor cells [3].
The diagnosis is usually made by means of clinical imaging methods and histopathological examination. The suspicion of malignancy in an initial PA increases when an insidious symptom is noted with development in a period of less than 10 months [1],[4]. Moreover, sensory loss, vision disorders, and painful clinical signs and symptoms are relevant clinical findings for considering the diagnosis of malignant neoplasia such as ductal carcinoma, adenoid cystic carcinoma, and mucoepidermoid carcinoma of the lacrimal glands [1].
According to the histopathological assessment and immunohistochemistry analyses, recent studies have shown variations in the genes associated with carcinogenesis and tumor progression, such as overexpression of HER2, p53, p40, p63, Cytokeratin 7, among others. Primary detection of these genetic variations is considered relevant with regard to the treatment and prognosis of the lesion, since the highly aggressive local behavior can lead to immediate recurrence and the death of patients suffering from this condition [3],[5].
Surgery involving complete removal of the lesion with enlarged margins, which can be performed by using various surgical techniques. Included among these are: lateral orbitotomy and its recently modified approach, cranio-orbital resection, pterional craniotomy, and macroscopic eye-preserving tumor excision [6],[7] and adjuvant radiotherapy, which are the therapeutic modalities of choice for decreasing recurrence rates, increasing overall survival (OS), disease-free survival (DFS), and local disease control (LDC). The majority of cases can be treated with eye-sparing surgery and radiation unless a tumor that extends into the skull base is present [7]. Regular cycles of chemotherapy have been used in order to reinforce the results obtained with both therapies mentioned, when indicated [1],[7].
We present this case report with the aim of describing our experience in the multimodal treatment of an atypical presentation of transformation of PA of the lacrimal gland into a rapidly developing high-grade ductal carcinoma and describe the proposed adjuvant radiation treatment.
Case Report
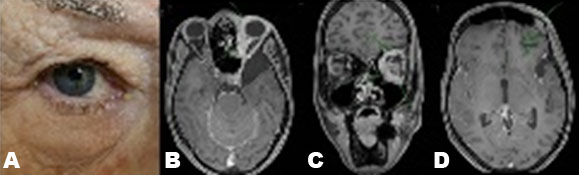
A 74-year-old woman presented to our institution complaining about insidious symptoms that had started nine months previously. She reported painless changes in the vision of the right eye compatible with proptosis and diplopia. In addition, her medical data included systemic impairment due to diabetes mellitus (DM), systemic arterial hypertension (SAH), hepatitis C, and chronic cardiac arrhythmia as systemic disorders that were under treatment at present.
In the computed tomography (TC) imaging examination, an expansive osteolytic lesion was seen in the region of the medial orbital wall, and magnetic resonance imaging (MRI) showed a multilocular region with hematic content in the lacrimal gland region, which was initially considered a vascular lesion, as shown in Figure 1.
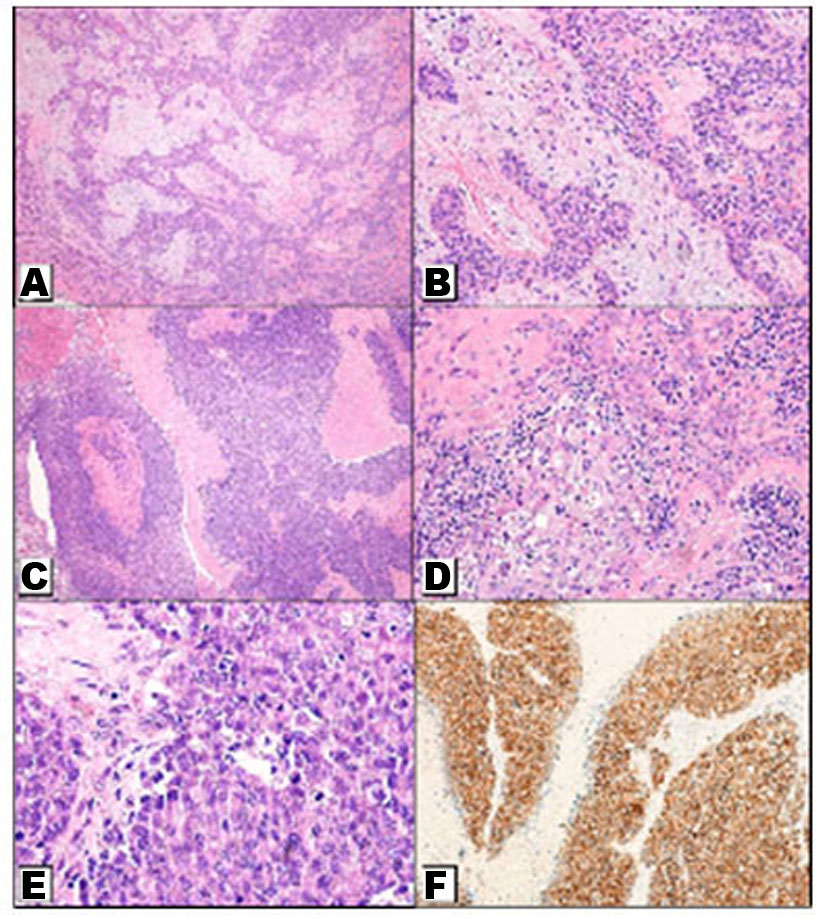
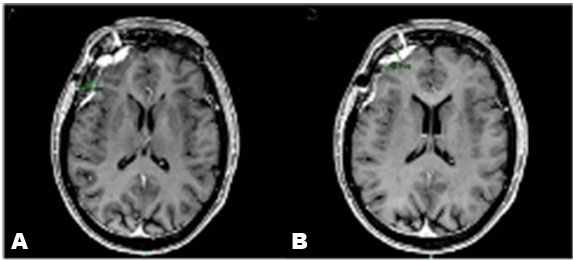
Although the patient was considered ASA III according to the American Society of Anesthesiologists (ASA) – physical status, surgery was proposed using the pterional craniotomy technique and the histopathological assessment confirmed the diagnosis of carcinoma ex-pleomorphic adenoma (Ca ex PA), which showed characteristics of a high-grade ductal carcinoma similar to that described for salivary glands (Figure 2A, Figure 2B, Figure 2C, Figure 2D, Figure 2E). Moreover, immunohistochemistry analysis showed that tumor had overexpression of the HER2 gene (after quantification) and was negative for changes in the TRK gene (Figure 2F). Finally, MRI was performed after surgical removal postoperatively for assessment of disease control as observed in Figure 3.
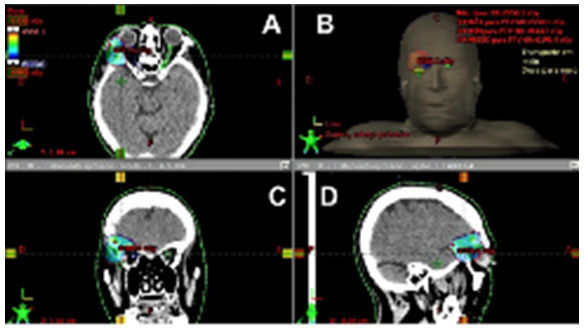
Regarding the adjuvant treatment to be performed, our team opted for radiotherapy (RT) without concomitant chemotherapy due to the patient's clinical comorbidities. Two months after surgery, the patient started planning for RT using intensity modulated radiation therapy (IMRT) 60 Gy in the tumor bed, in daily fractions of 2 Gy, limiting the total dose to the right optic nerve to 54 Gy as shown in Figure 4 and Figure 5.
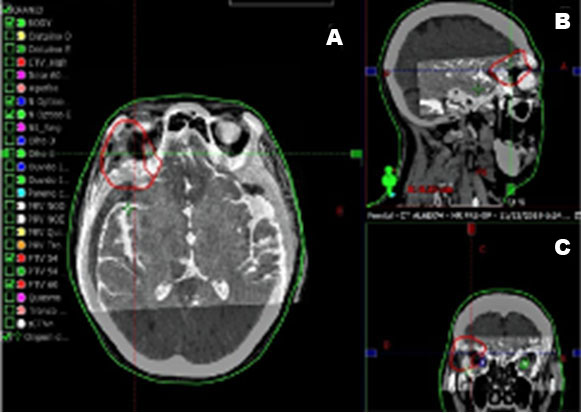
At present, the patient finished RT treatment and is in the sixth month of follow-up. During RT course, slight pain was referred when swallowing while feeding, associated with mild xerophthalmia. On clinical and imaging examinations, there has been no evidence of local recurrence of the tumor as observed in Figure 6.

Discussion
To reduce the risk of recurrence and malignant transformation, studies have suggested that the PAs of the lacrimal gland should be removed intact, without extravasation of the intracapsular content, and without previous biopsy [1],[2]. The recommended surgical approach is a lateral orbitotomy that has been modified during the years. This approach can also be used for tumors located in the lateral, upper, and lower orbital compartments. Recent modifications of this technique have shown satisfactory clinical results due to adequate exposure, acceptable cosmetic results, and by providing an easy and direct access to the tumor in a bloodless environment. Thus the operator has been able to completely remove the tumor, when compared with or as opposed to other approaches [6].
Moreover, the modified surgical approach for removing tumors of the orbital lobe, with section of the isthmus between the orbital and eyelid lobes (and their preservation) has led to a significant reduction in changes in the corneal surface. In fact, preservation of the palpebral lobe of the gland, as suggested by Rose and Wright, has reduced some complications inherent to the procedure, such as the incidence of dry eye in the postoperative period and upper eyelid deformation.
In the present case report, the patient underwent surgical treatment via right pterional craniotomy, initially described by Yasargil et al. in 1975, including the upper lateral orbital rim. Afterwards, under microscopy, an expansive lesion was identified and resected in the topography of the lacrimal gland. The surgical specimen was fragmented and sent to the laboratory in frozen sections, confirming the diagnosis of Ca ex PA of the right lacrimal gland.
With regard to the morphological features of the tumor, better prognosis has been found for intracapsular (non-invasive) and minimal extracapsular extension (<5 mm), which are considered early Ca ex PA. Moreover, the immunohistochemical overexpression of HER-2, p53 protein, and Mib-1 proliferation markers may be useful markers to identify malignant areas in PA [8]. In our immunohistochemistry analysis, the patient showed an overexpression of HER-2 protein as mentioned above. Moreover, patients with non-invasive or minimally invasive Ca ex PA have better prognosis than patients with invasive Ca ex PA (>6 mm) [8],[9].
Adjuvant radiotherapy (RT) is indicated after surgery for high-risk patients to reduce locoregional recurrence. Initial studies have shown that adjuvant RT improves locoregional control (LDS) and OS, irrespective of the HER2 overexpression status [9]. Although no randomized clinical trial was found, observational data have indicated that adjuvant RT improved both local control and survival for selected patients. A study conducted by Mahmood in 2011 showed that patients who underwent adjuvant RT showed improved OS (HR 0.76, 95% CI 0.65–0.89).
Tumors arising in anatomical sites not suitable for complete resection and advanced-stage tumors (T2 and greater), positive surgical margins, and skin and/or nerve invasion all require post-operative RT. Moreover, the usual dose of adjuvant radiation used lies between 60 and 66 Gy, at about 2 Gy per fraction. It may be necessary to include regional lymph nodes and/or neural pathways to the skull base, when individuals have larger tumor volumes, high grade of multiple recurrences, and in cases of supernumerary nodal metastases (SNM) as described at present [9],[10].
An analysis of more than 2000 patients from the National Cancer Database demonstrated no improvement in OS with the addition of chemotherapy to RT compared with post-operative RT alone.
For patients with unresectable lesions, definitive radiation therapy (RT) is an option. This can be delivered with photons and electrons, but usually by IMRT. If a patient considered for RT has been classified with a good performance status, concomitant chemotherapy, platinum-based, should be considered [7],[10]. In our case, the patient had several systemic disorders; therefore, chemotherapy was avoided. Finally, the complications of RT vary depending on the anatomic site of the tumor and the dose applied.
Acute side effects of RT may negatively affect its application, but these are usually resolved in a period of weeks or months after conclusion of RT. Many of the late effects occur progressively over the course of time, and may eventually have an adverse effect on patients’ quality of life. In the head and neck region, several acute reactions described have been, especially, in the oral and maxillofacial region due to side effects on surrounding tissues such as jawbones, auricular regions, bones closer to the orbital region, salivary glands such as the parotid type. There are several immediate complications caused by radiation such as hearing loss, dermatological-radiation impairments, and late effects such as local bone necrosis areas. In the context of modern treatment scenarios, in many patients the damage caused by radiation is further aggravated by the administration of concurrent systemic cytotoxic agents [11],[12].
Conclusion
Malignant tumors of the lacrimal gland are rare and the chance of transformation of PA into high-grade ductal carcinoma, with higher morbidity and mortality, remains uncertain. A correct clinical diagnosis starting with anamnesis in order to obtain complete data on the development of the disease until an appropriate surgical technique performed, in order to achieve complete removal of the lesion, are factors that may guarantee a favorable prognosis for this type of lesion. When adjuvant therapy is indicated, radiotherapy is the treatment of choice, because of increasing LDS and OS, irrespective of the presence of histopathological variations. The patient's systemic condition is a factor to be taken into account when considering additional chemotherapy. Prospective randomized studies are still lacking and must be conducted because they are relevant for an accurate assessment of the efficiency of multimodal treatment in managing the disease.
REFERENCES
1.
Harrison W, Pittman P, Cummings T. Pleomorphic adenoma of the lacrimal gland: A review with updates on malignant transformation and molecular genetics. Saudi J Ophthalmol 2018;32(1):13–6.

2.
Ashok Kumar P, Paulraj S, Mirchia K, Hahn SS, Sivapiragasam A. Ductal adenocarcinoma ex pleomorphic adenoma of the lacrimal gland: A rare and morbid malignancy. Case Rep Oncol Med 2020;2020:1790106 [CrossRef]
[Pubmed]
3.
Garakani R, Kersten R, Pekmezci M. Intracapsular high-grade ductal carcinoma in-situ ex pleomorphic adenoma of the lacrimal gland. Ophthalmic Plast Reconstr Surg 2020;36(1):e1–3.
[Pubmed]
4.
Larbcharoensub N, Pangpunyakulchai D, Aroonroch R, Tuntiyatorn L, Mahaisavariya P. Lacrimal myoepithelial carcinoma ex recurrent pleomorphic adenoma: A clinicopathological report and review of the literature. Mol Clin Oncol 2018;8(1):209–13. [CrossRef]
[Pubmed]
5.
Zhang P, Tang LJ, Gao HH, Zhang WX, Lin JX, Yang HS. Immunohistochemical features of carcinoma ex pleomorphic adenoma and pleomorphic adenoma in the lacrimal gland. Int J Ophthalmol 2019;12(8):1238–42. [CrossRef]
[Pubmed]
6.
Rose GE, Gore SK, Plowman NP. Cranio-orbital resection does not appear to improve survival of patients with lacrimal gland carcinoma. Ophthalmic Plast Reconstr Surg 2019;35(1):77–84. [CrossRef]
[Pubmed]
7.
Tom A, Bell D, Ford JR, et al. Malignant mixed tumor (carcinoma ex pleomorphic adenoma) of the lacrimal gland. Ophthalmic Plast Reconstr Surg 2020;36(5):497–502.
[Pubmed]
8.
Di Palma S. Carcinoma ex pleomorphic adenoma, with particular emphasis on early lesions. Head Neck Pathol 2013;7(Suppl 1):S68–76. [CrossRef]
[Pubmed]
9.
Haderlein M, Scherl C, Semrau S, et al. Impact of postoperative radiotherapy and HER2/new overexpression in salivary duct carcinoma: A monocentric clinicopathologic analysis. Strahlenther Onkol 2017;193(11):961–70. [CrossRef]
[Pubmed]
10.
Ampil FL, Dela Cruz N, Richards TA, Nathan CAO, Chang B. Successful tri-modality treatment of atypical carcinoma ex-pleomorphic adenoma with more than 50 nodal metastases. Int J Radiat Oncol Biol Phys 2020;106(5):1157. [CrossRef]
11.
Wang Y, Tu W, Tang Y, Zhang S. Prevention and treatment for radiation-induced skin injury during radiotherapy. Radiat Med Prot 2020;1(2):60–8.
12.
Azzam P, Mroueh M, Francis M, Daher AA, Zeidan YH. Radiation-induced neuropathies in head and neck cancer: Prevention and treatment modalities. Ecancermedicalscience 2020;14:1133. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Acknowledgments
The co-author Wilber E Bernaola-Paredes is student fellow and supported with a scholarship provided by the National Council for Scientific and Technological Development of Brazil (CNPq), Sao Paulo, Brazil (140071/2019-9).
Author ContributionsWilber E Bernaola-Paredes - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Valdener Bella Filho - Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Henrique Perez Carvalho - Acquisition of data, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Felipe Ko Chen - Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
José Francisco Dalcin - Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Felipe D'Almeida Costa - Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Antonio Cassio Assis Pellizzon - Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2021 Wilber E Bernaola-Paredes et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}