 |
Case Report
Unusual ovarian vein thrombosis: A case report and review of the literature
1 Radiology Department, National Institute of Oncology, Mohamed V University, Rabat, Morocco
Address correspondence to:
Basma Taibi
Radiology Department, National Institute of Oncology, Mohamed V University, Rabat,
Morocco
Message to Corresponding Author
Article ID: 101115Z01BT2020
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Taibi B, Saoud A, Ayouche O, Omor Y, Latib R. Unusual ovarian vein thrombosis: A case report and review of the literature. Int J Case Rep Images 2020;11:101115Z01BT2020.ABSTRACT
Introduction: Ovarian vein thrombosis (OVT) is an uncommon but potentially serious clinical disorder, which mostly present in the postpartum period but can also occur with malignant and inflammatory conditions in the non-obstetrical patient. The diagnosis is mainly based on imaging techniques, in particular computed tomography (CT) and magnetic resonance, for their sensitivity and specificity.
Case Report: We present a case of a 59-year-old female who was diagnosed with endometrial carcinoma. Her abdominal contrast-enhanced CT revealed an expanded right ovarian vein with soft tissue attenuation material in its lumen extending into the inferior vena cava, reaching the right atrium and ventricle.
Conclusion: We describe this case of OVT, because, even though rare, it is a diagnosis to consider. Prompt recognition and treatment are crucial to avoid more severe outcomes.
Keywords: Cancer, Computed tomography, Ovarian vein thrombosis, Vena cava
Introduction
Ovarian vein thrombosis (OVT) is a rare but potentially lethal complication [1]. It is classically associated with postpartum (puerperal) endometritis. However, it can occur in other circumstances, such as inflammatory diseases of the pelvis, gynecological tumors, after pelvic surgery, during sepsis, hypercoagulable state, or even sometimes without an underlying cause [1]. It is usually manifested by nonspecific abdominal pain, with or without fever, and must be recognized because of its potentially serious complications (pulmonary embolism). Historically, OVT was identified during explorative laparoscopy with a reserved prognosis and a mortality of almost 50% [2]. Currently, the diagnosis is done earlier thanks to imaging techniques making the prognosis better.
Case Report
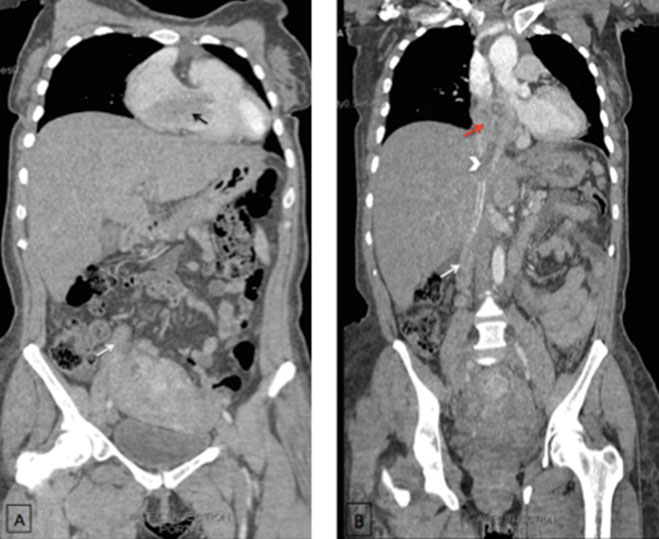
A 59-year-old woman, G0P0 diagnosed with an endometrial carcinoma FIGO stage III in good general condition. The patient underwent a contrast-enhanced abdominal CT showing an expanded right ovarian vein low-attenuation intraluminal material (Figure 1) presumably representing the thrombus. The thrombosis was reaching the inferior vena cava (IVC) and extending to the right atrium and ventricle (Figure 2). Diagnosis of venous thrombosis was highly suspected on the CT based on three criteria: venous enlargement, low-density intraluminal material, and a sharply defined enhancing wall.
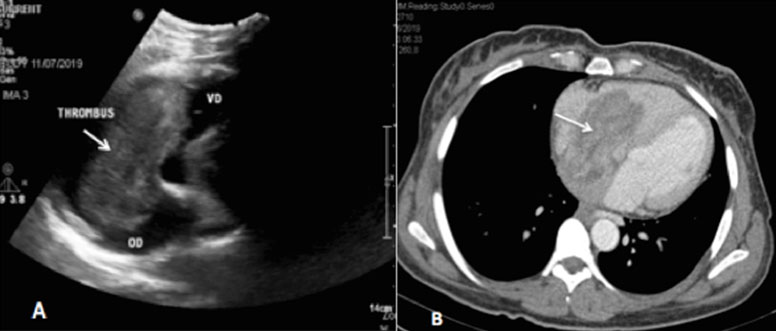
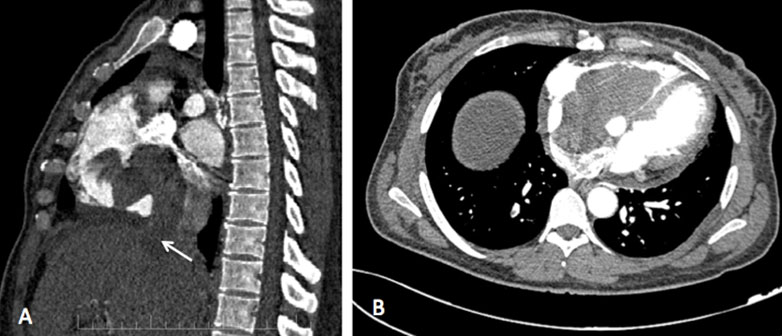
Since the timing for the acquisition of the images was not appropriate, we could not achieve uniform homogenous venous opacification. Therefore, a second look Doppler ultrasound was performed demonstrating a hypoechoic tubular paravertebral structure, between the IVC and the uterine appendices. This structure continued until the renal area where it joined the IVC, in favor of right ovarian vein thrombophlebitis. Ultrasound also identified an abnormal soft hypoechoic tissue in the IVC (Figure 3) reaching the right atrium and ventricle (Figure 4A). Anticoagulation was started immediately with enoxaparin 0.4 mL (18,000 Units) subcutaneous injection twice a day in the first week, then she was maintained on rivaroxaban 20 mg daily and the surgery was delayed. Computed tomography scan at six months showed a persistence of the tumoral OVT reaching the right atrium and ventricle (Figure 5). It also demonstrated an increase in the tumor size and the appearance of peritoneal and pericardial effusions. Rivaroxaban was maintained and chemotherapy (carboplatin-paclitaxel) was started. No follow-up study was obtained as the patient died after one month.


Discussion
Ovarian vein thrombosis is an uncommon clinical entity, most familiar to radiologists as a complication of the postpartum period with an incidence reaching 1 in 2000–3000 deliveries [3].
It can also occur with other common conditions in the non-obstetrical patient. Documented non-obstetrical etiologies include pelvic surgery, particularly for gynecologic malignancies, oncology patients with non-gynecologic malignancies, gastrointestinal tract inflammation, and some rare occurrences in complicated laparoscopic cholecystectomy [4]. Our case is important due to low incidence of tumoral extension to the right ventricle and high mortality.
The classical clinical picture is vague and includes abdominal pain, fever, nausea, vomiting, and malaise. Unlike puerperal or OVT after pelvic surgery, OVT associated with malignancy and chemotherapy can be asymptomatic as in our case.
These symptoms are inconsistent and nonspecific. It requires the combined efforts of several disciplines to establish the diagnosis. Prompt recognition and imaging are necessary to establish the diagnosis and avoid further complications.
Patients with cancer are clearly at high risk for developing venous thromboembolism (VTE). However, it varies markedly among patients regardless of the primary tumor site, stage, initial period after diagnosis, presence, number of comorbidities, and treatment modalities [5]. Moreover, the rates of VTE seem to be increasing, particularly in association with chemotherapy [5].
Virchow described the pathogenic mechanisms accounting for the development of thrombotic disorders in cancer patients more than a century ago. They include hypercoagulability due to tumor cell activation, vessel wall injuries, and stasis. Patients with malignant tumors can, therefore, be considered to be at an increased risk for developing VTE, even in the absence of chemotherapy treatment.
Before the advent of cross-sectional imaging, the diagnosis of OVT was made by surgery or heparin test. The first case diagnosed by CT was reported in 1981 [6]. Pelvic ultrasound (US) is usually used for initial investigation, and follow-up, because it is a simple and easily accessible exam, allowing for a quick exclusion of another diagnosis [7].
On US, the aspect matches that of acute venous thrombosis of other localization. However, the classic criterion of non-compressibility of the thrombosed vein is difficult to use in case of OVT, due to the deep situation of ovarian veins. A thrombosed ovarian vein is seen as an anechoic to hypoechoic tubular structure that extends superiorly from the adnexa, across the iliac vessels, and lateral to the great vessels in retroperitoneum, with lack of color-flow filling and the absent spectral waveform [8]. Sensitivity, specificity, and accuracy of color US are reported to be 55.6%, 41.2%, and 46.2%, respectively [9].
Ultrasound poor detection rates are due to visibility impairment secondary to bowel gas interposition and the inability to visualize the ovarian vein in all cases or its total extent; additionally, OVT ultrasound image may be confused with appendicitis, hydroureter, lymphadenopathy, hydrosalpinx, and inferior mesenteric vein thrombosis [9].
In case of a nonconclusive ultrasound, the CT with intravenous contrast is the imaging technique of choice to search for an OVT [10] with a 77.8–100% sensibility and a 62.5–100% specificity [7].
Therefore, it should be used as an initial technique due to its cost-effectiveness. The thrombosed vein appears as a thick-walled, enlarged vein with rim enhancement and central hypodensity. Appropriate timing for the acquisition of the images is mandatory to achieve uniform homogenous venous opacification. Early acquisition of images on current fast helical scanners may show a non-enhanced or heterogeneously enhanced vein that may result in inconclusive interpretation or misinterpreted as thrombus [8].
Magnetic resonance imaging (MRI) is similar to CT without the need for contrast and exposure to ionizing radiation but MRI is time-consuming and less readily available than CT [3].
However, because of the superior sensitivity of MRI to flow and paramagnetic iron, differentiation between acute and subacute thrombus is possible, which make it the most reliable investigation with sensitivity as well as specificity of 100% [11],[12].
Generally, the ovarian vein clot is subacute (between one week and one month), with shortened T1 and prolonged T2 relaxation time and, therefore, is hyperintense on both weightings. Time-of-flight sequence (TOF) or contrast-enhanced magnetic resonance venography shows thrombus as filling defects [8].
Sepsis and pulmonary embolism are the two major complications of OVT, with the latter occurring in 13–25% of postpartum OVT cases.
A treatment combining, intravenous broad-spectrum antibiotics, and heparin must, therefore, be quickly started. There are no specific guidelines in place for the duration of treatment.
Some authors advocate a brief course of anticoagulants, reporting thrombus dissolution after 7–14 days; others argue that thrombosis persists with short-course treatments, recommending continuing anticoagulants for 3–6 months, until radiological confirmation of resolution.
For non-postpartum situations the treatment remains controversial, the need of a routine anticoagulation and antibiotics is not yet clear, no randomized study has yet been done in these rare situations and some studies have shown that the thrombus can resolve without complications even in the absence of any treatment [4].
Conclusion
Tumor-associated ovarian venous thrombosis is especially at risk of pulmonary embolisms. It results in morphological as well as hemodynamic changes with right heart consequences. These elements are valuable for accurate positive diagnosis, but also for therapeutic management.
REFERENCES
1.
Bennett GL, Slywotzky CM, Giovanniello G. Gynecologic causes of acute pelvic pain: Spectrum of CT findings. Radiographics 2002;22(4):785–801. [CrossRef]
[Pubmed]

2.
Meuwly JY, Kawkabani-Marchini A, Sgourdos G. Thrombose veineuse ovarienne. Forum Med Suisse 2012;12(7):144–8.
3.
Rottenstreich A, Da'as N, Kleinstern G, Spectre G, Amsalem H, Kalish Y. Pregnancy and non-pregnancy related ovarian vein thrombosis: Clinical course and outcome. Thromb Res 2016;146:84–8. [CrossRef]
[Pubmed]
4.
Jain KA, Jeffrey RB Jr. Gonadal vein thrombosis in patients with acute gastrointestinal inflammation: Diagnosis with CT. Radiology 1991;180(1):111–3. [CrossRef]
[Pubmed]
5.
Khorana A, Connolly GC. Assessing risk of venous thromboembolism in the patient with cancer. J Clin Oncol 2009;27(29):4839–47. [CrossRef]
[Pubmed]
6.
Shaffer PB, Johnson JC, Bryan D, Fabri PJ. Case report. Diagnosis of ovarian vein thrombophlebitis by computed tomography. J Comput Assist Tomogr 1981;5(3):436–9. [CrossRef]
[Pubmed]
7.
Aguilar S, Cunha V, Colaço J, Martins L, Nunes F, Kayryakova M. Ovarian vein thrombosis: A case report. International Journal of Medical Reviews and Case Reports 2019;3(8):494–8.
8.
Virmani V, Kaza R, Sadaf A, Fasih N, Fraser-Hill M. Ultrasound, computed tomography, and magnetic resonance imaging of ovarian vein thrombosis in obstetrical and nonobstetrical patients. Can Assoc Radiol J 2012;63(2):109–18. [CrossRef]
[Pubmed]
9.
Twickler DM, Setiawan AT, Evans RS, et al. Imaging of puerperal septic thrombophlebitis: Prospective comparison of MR imaging, CT, and sonography. AJR Am J Roentgenol 1997;169(4):1039–43. [CrossRef]
[Pubmed]
10.
Slam K, Duckett S, Thirumoorthi AS, Clark PM. Ovarian vein thrombosis in two postpartum women. Hospital Physician 2008;31–5.
11.
Jenayah AA, Saoudi S, Boudaya F, Bouriel I, Sfar E, Chelli D. Ovarian vein thrombosis. Pan Afr Med J 2015;21:251. [CrossRef]
[Pubmed]
12.
Kominiarek MA, Hibbard JU. Postpartum ovarian vein thrombosis: An update. Obstet Gynecol Surv 2006;61(5):337–42. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Basma Taibi - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Aida Saoud - Conception of the work, Design of the work, Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Othman Ayouche - Acquisition of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Youssef Omor - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Rachida Latib - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2020 Basma Taibi et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}