 |
Case Report
Superficial angiomyxoma of vulva: A case report
1 Resident Doctor, Department of Gynecology and Obstetrics, University Hospital of Brasília, Universidade de Brasília, Brasília, DF, Brazil
2 Surgeon, Department of Gynecology and Obstetrics, University Hospital of Brasília, Universidade de Brasília, Brasília, DF, Brazil
3 Pathologist, Integrated Center of Pathology of Brasilia, Brasilia, DF, Brazil
4 Gynecologist and Teacher, Department of Gynecology and Obstetrics, University Hospital of Brasília, Universidade de Brasília, Brasília, DF, Brazil
Address correspondence to:
Ariane Lázaro Teixeira
Department of Gynecology and Obstetrics, University of Brasilia Hospital, SGAN 604/605, Av L2 norte, Asa Norte, Brasilia, DF 70840-901,
Brazil
Message to Corresponding Author
Article ID: 101107Z01AT2020
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Teixeira AL, de Oliveira VR, de Barros Junior AP, Fidelis CR, Basílio DB, Primo WQSP. Superficial angiomyxoma of vulva: A case report. Int J Case Rep Images 2020;11:101107Z01AT2020.ABSTRACT
Introduction: Superficial angiomyxoma (SAM) is a rare, benign mesenchymal neoplasm comprised of prominent myxoid matrix and numerous blood vessels. It occurs more commonly in extragenital regions, especially the trunk, limbs, head, or neck. It is more frequent in males, with peak incidence in the fourth decade of life. The diagnosis is made by the pathologist. Only a few cases of SAM in the genital region have been reported in the literature.
Case Report: Displayed here is the case of a female patient, 24 years old, with lesions in the pubic hill and two masses, one in each of the labia minora, of slow growth, painless, not pruriginosas, and no signs of infection. The lesions were extirpated and the anatomopathological examination was compatible with SAM of vulva. The patient recovered well and keeps up.
Conclusion: The SAM is a benign tumor of soft parts, which rarely occurs in the genital region. It should be distinguished from other tumors of the vulva, especially of the aggressive angiomyxomas (AAMs). The detailed anatomopathological study and immunohistochemical staining can help to clarify the diagnosis.
Keywords: Aggressive, Angiomyxoma, Superficial, Vulva
Introduction
Superficial angiomyxoma (SAM) is a rare, benign mesenchymal neoplasm comprised of prominent myxoid matrix and numerous blood vessels [1]. It was initially described by Carney et al. in 1985, in association with the Carney complex syndrome, a rare autosomal dominant disorder characterized by neoplasm involving the heart, the central nervous system, and the endocrine organs [2]. It was recognized as an independent cutaneous tumor, without the manifestations of the Carney complex, by Allen et al. in 1998 and Calonje et al. in 1999 [1]. The SAM occurs more commonly in extragenital regions, especially the trunk, limbs, head, or neck [3]. It is more frequent in males, with peak incidence in the fourth decade of life [1]. In women, it occurs with greater frequency in reproductive age, from 11 to 39 years [4]. Clinically, they present themselves as well circumscribed lesions, nodular or multinodular, slow growing and painless, which often extend to subcutaneous tissue, and usually have more than 5 cm in diameter [3],[5]. Until 2016, only 19 cases of vulvar SAMs have been reported in the literature. Due to its rare occurrence and lack of distinct clinical characteristics, it may be misdiagnosed as a polyp, Bartholin’s cyst, cyst of duct of Gartner or a perineal hernia on clinical examination. Therefore, the diagnosis is not usually done by clinicians and, yes, by the pathologist [3],[4],[5].
Histologically, the tumor consists of lobules of fusiform tumor cells or stellated similar to fibroblasts, with plenty of myxoid stroma that contains numerous blood vessels from small to medium caliber, and inflammatory cells, especially neutrophils [3].
Case Report
A 24-year-old, unmarried, nulligravida, female patient with one white parent and one black parent, without any known previous comorbidities, without significant pathological family history, was seen in the oncologic gynecology outpatient clinic of the University Hospital of Brasilia in September 2018 referring lesions in pubic hill for about five years, of slow growth, painless, not itchy, with no inflammatory signs.
For the past two years, it has been reported the appearance of two masses, one in each of the lower lip, also painless, not pruriginosas, of progressive growth. She did not seek timely medical care due to embarrassment. On physical examination, the region of pubic hill was edematous, with the portion hyperkeratotic around the clitoris, with deep and multiple grooves, with the appearance of “Cracked Earth.” The presence of two pedicled masses was seen, each one in the anterior portion of a labia minora, measuring about 10 cm in the left side and 8 cm from the right side, not painful, without signs of inflammation, and with consistency of soft parts (Figure 1).
After the initial evaluation with general laboratory examinations and serologic tests for sexually transmitted infections (STIs), the patient underwent a transvaginal ultrasound, magnetic resonance imaging of the pelvis with contrast and computed tomography scan of the total abdomen, all without significant changes. She was then submitted to excisional biopsy of lesions in the labia minora and incisional biopsy of lesion in pubic hill, total three fragments.
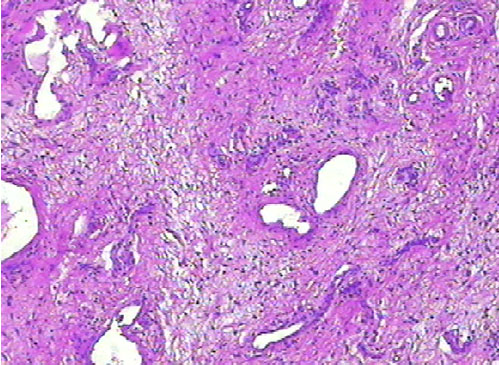
The result of the anatomopathological examination was pedicled lesion, coated by stratified squamous epithelium, keratinized, displaying vessels of various shapes, coated by a prominent endothelium, interspersed with elongated cells, sometimes fusocellular sometimes stellated, in the midst of the stroma sometimes fibrous sometimes myxoid. Occasional lymphocytes and neutrophils were noticed. There were no mitotic figures (Figure 2).
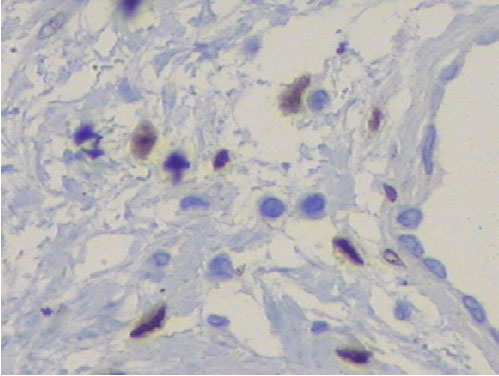
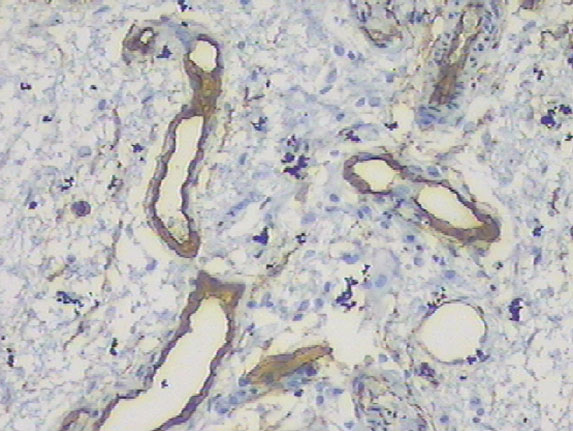
The immunohistochemistry (IHC) showed positivity for hormonal receptors of estrogen and progesterone (Figure 3 and Figure 4), as well as positivity for vimentin and smooth muscle actin (Figure 5 and Figure 6). The vessels marked for CD34 and desmin (Figure 7 and Figure 8). There was negativity for S100. The histology and IHC were compatible with SAM of vulva.
The treatment was the complete excision of the lesions (Figure 9). The anatomopathological results of the operative part confirmed the diagnosis of SAM of vulva. The patient recovered well and keeps up uneventfully (Figure 10).







Discussion
As occurs in our patient, the SAMs described earlier in women occurred in the vulva, groin, or pubic hill, with sizes ranging from 0.6 to 12.5 cm [1]. The lesions are well-delineated and appear as cutaneous nodules multilobular of soft consistency, painless, slow growth, which often extend to the subcutaneous fat. They are usually larger than 5 cm in diameter [5]. Its surface can be grayish white, translucent, and gelatin, with occasional hemorrhagic content. The duration of symptoms can vary from 10 months to 2 years [3],[4]. In this case, the lesions of the labia minora presented themselves as a pedicled mass, with gelatinous surface, without hemorrhagic content. Since the lesions in pubic hill were multinodular, hyperkeratotic, with hardened consistency.
Histologically, the tumor consists of lobules of fusiform tumor cells or stellated similar to fibroblasts, with plenty of myxoid stroma that contains numerous blood vessels from small to medium caliber, and inflammatory cells, especially neutrophils. These characteristics corroborate with the histopathological findings of the case presented. Furthermore, 25–30% of the SAMs contain an epithelial component, a finding that is also present in this case, generally in the form of cysts lined with stratified squamous epithelium, shoots of basaloid cells, or beads of squamous epithelium [3]. Scattered inflammatory cells, especially stromal neutrophils, are always present, this being a useful histological track, particularly in the absence of necrosis or ulceration [6]. Nuclear pleomorphisms and mitosis are uncommon [1],[6].
A variety of immunohistochemical studies were conducted to distinguish from other similar tumors or to explore the origin of the tumor cells. According to a study done by Calonje et al. in 1999, the tumor cells were positive for vimentin, but negative for CD34, α-smooth muscle actin, HHF-35, S-100 protein, cytokeratin and desmin, and glial fibrillary acidic protein. However, Fetsch et al. reported that the SAM could be positive for desmin and smooth muscle actin [7]. In the case of this patient, the IHC was coincident with the data available in the literature so far, being positive for vimentin and smooth muscle actin and desmin, but also showed positivity for estrogen and progesterone receptor, these being more common in cases of aggressive angiomyxoma.
As the immunohistochemical characteristics of the neoplasia were not established, some researchers mention that they are not useful for the differential diagnosis of myxoid tumors. Additional analyzes will be needed to characterize clinically and immunohistochemically the SAM [7].
Although there are no reports of metastasis or malignant transformation, the lesion must be completely cut off with a disease-free margin, whenever possible, since studies of the long-term follow-up revealed local recurrence of the tumor. The recurrence rate is approximately 30–40% and is associated with the inadequate resection [1][3] [4],[5],[6],[7].
When SAM occurs in the vulva, it is important for the differential diagnosis with aggressive angiomyxoma (AAM). The latter occurs most commonly in the tissues of the pelvic and perineal region of the female sex [1],[5],[8], with diameters ranging from 2 to 60 cm and with a greater tendency to local recurrence [5],[9]. In addition, there are two reports in the literature of AAMS with metastases, whereas there are no reported cases of metastases in SAMs [3]. In general, the AAM is a deeper lesion, with infiltrative margin and a tumor in growth that retains fat, nerves, and blood vessels in the resection margin, contrasting with the growth pattern of well-demarcated multinodular of SAMs [3]. In comparison with the vessels of thin walls of SAMs, the blood vessels in the AAMs are more variable, usually with thicker walls. Mitotic activity and nuclear atypia are missing [1],[5],[8]. Generally, they present positivity for desmin, smooth muscle actin, estrogen receptor, and progesterone receptor [4],[8],[9].
Conclusion
The SAM is a benign tumor of soft parts, which rarely occurs in the genital region. It may be an independent tumor or be associated with Carney complex. It should be distinguished from other tumors of the vulva, especially of the AAMs, which have local infiltration and high risk of recurrence. The detailed anatomopathological study and, in some cases, immunohistochemical staining, can help to clarify the diagnosis.
REFERENCES
1.
Lee CC, Chen YL, Liau JY, Chen CA, Cheng WF. Superficial angiomyxoma on the vulva of an adolescent. Taiwan J Obstet Gynecol 2014;53(1):104–6. [CrossRef]
[Pubmed]

2.
Abarzúa-Araya A, Lallas A, Piana S, Longo C, Moscarella E, Argenziano G. Superficial angiomyxoma of the skin. Dermatol Pract Concept 2016;6(3):47–9.
[Pubmed]
3.
Kim HS, Kim GY, Lim SJ, Ki KD, Kim HC. Giant superficial angiomyxoma of the vulva: A case report and review of the literature. J Cutan Pathol 2010;37(6):672–7. [CrossRef]
[Pubmed]
4.
Lee SH, Cho YJ, Han M, et al. Superficial angiomyxoma of the vulva in the postmenopausal woman: A case report and review of literature. J Menopausal Med 2016;22(3):180–3. [CrossRef]
[Pubmed]
5.
Ozdemir M, Uzun I, Karahasanoglu A, Ceylan C. A case of vulvar superficial angiomyxoma: A rare clinical entity. J Obstet Gynaecol 2016;36(5):683–4. [CrossRef]
[Pubmed]
6.
Nucci MR, Fletcher CD. Vulvovaginal soft tissue tumours: Update and review. Histopathology 2000;36(2):97–108. [CrossRef]
[Pubmed]
7.
Yamamoto K, Kondo A, Iwashita K, et al. A case of superficial angiomyxoma. Tokai J Exp Clin Med 2006;31(2):53–5.
[Pubmed]
8.
Basak S, Rogers S, Solomonsz AF. superficial angiomyxoma of the vulva: A case report of a rare cutaneous tumour. J Obstet Gynaecol 2011;31(4):360–1. [CrossRef]
[Pubmed]
9.
Xie Y, Qian Y, Zou B. A giant aggressive angiomyxoma of vulva in a young woman: A case report. Medicine (Baltimore) 2019;98(2):e13860. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Acknowledgments
The consent was obtained in writing from the patient for the publishing of this case report with attached pictures.
Author ContributionsAriane Lázaro Teixeira - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Viviane Rezende de Oliveira - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Amário Pires de Barros Junior - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Cecília Ramos Fidelis - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Dunya Bachour Basílio - Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Walquíria Quida Salles Pereira Primo - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2020 Ariane Lázaro Teixeira et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}