 |
Case Report
Acute febrile abdomen resistant to antibiotic therapy: A case report and review of the literature
1 Radiology Department, Mohamed the Fifth Military Instruction Hospital, Mohamed V University, Rabat, Morocco
Address correspondence to:
Neftah Camelia
Radiology Department, Mohamed the Fifth Military Instruction Hospital, Mohamed V University, Rabat,
Morocco
Message to Corresponding Author
Article ID: 101100Z01NC2020
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Camelia N, Meriem E, Ayouche O, El Bakkari A, Dieukedao F, Boumdin H. Acute febrile abdomen resistant to antibiotic therapy: A case report and review of the literature. Int J Case Rep Images 2020;11:101100Z01NC2020.ABSTRACT
Introduction: Digestive perforation can present in a variety of clinical and radiological aspects. In all cases, computed tomography (CT) scan is of urgent necessity as it can contribute to the positive diagnosis as well as etiological identification that can change therapeutic management. We have to outline the importance of the difference between surgical free peritoneal perforations and covered perforation. Covered perforation may manifest as acute febrile abdomen evolving for days resistant to probabilistic antibiotic therapy before primary consultation.
Case Report: We expose the case of a 50-year-old patient, with a history of chronic smoking, consulted in the emergency department for a subocclusive syndrome evolving for six days. An abdominal CT: The diagnosis of covered duodenal perforation was retained. Due to a development of hypovolemic shock, which did not recede with vasoactive drugs. The decision was to do a laparotomy with peritoneal lavage with suture of the anterior duodenal perforation and a drainage of the abdominal cavity. The evolution was characterized, five days after, by the death of the patient.
Conclusion: Gastroduodenal perforations in free peritoneum result in pneumoperitoneum, which is usually voluminous, especially if the lesions sit in its anterior surface. Partially covered gastroduodenal perforations result in local changes in the peritoneum corresponding to localized peritonitis. In such cases, however, the ulcerative lesion must be proven by the localized interruption of mucosal enhancement. These elements are valuable for accurate positive diagnosis, but also for therapeutic management.
Keywords: Computed tomography, Duodenum, Febrile abdomen, Perforation
Introduction
Digestive perforations are a classic cause of acute abdominal pain syndrome. Its diagnosis is an emergency. Digestive perforations are disruption of continuity of the digestive wall connecting the lumen with the peritoneal cavity or retroperitoneal spaces. A purulent or aseptic liquid can cause peritoneal irritation. Its consequence is peritonitis, which can be generalized or localized. If the liquid bathes the entire peritoneal cavity, it is a generalized peritonitis. If only a part of the abdominal cavity is interested, it is a localized peritonitis.
Perforations in the free peritoneum generally result in a pneumoperitoneum often supramesocolic or retroperitoneal depending on the site of the lesion. While the covered perforations in whole or in part are characterized by localized peritonitis with some intra or retroperitoneal bubbles having a localizing value.
Annual incidence estimates of peptic ulcer perforation were 3.8–14 per 100,000 individuals [1]. The mortality rate ranges from 8% to 25% [1]. Duodenal perforation is secondary to underlying duodenal pathology. Peptic ulcer disease is a leading cause of acute perforations of the duodenum that are estimated to occur in 2–10% of patients with ulcers [2],[3].
Duodenal perforations can also occur with various conditions, such as duodenal diverticula, duodenal ischemia, infectious disease and autoimmune conditions, tumors, chemotherapy, and impacted gallstones in the duodenum [3]. Iatrogenic perforations endoscopic or operative. Spontaneous perforations occur usually in neonates in unknown circumstances [3].
Digestive perforation can present in a variety of clinical and radiological aspects. In all cases, CT scan is of urgent necessity as it can contribute to the positive diagnosis as well as etiological identification that can change therapeutic management [4].
We have to outline the importance of the difference between surgical free peritoneal perforations and covered perforation [5]. Covered perforation may manifest as acute febrile abdomen evolving for days resistant to probabilistic antibiotic therapy before primary consultation [6].
Case Report
A 50-year-old patient, with a history of chronic smoking, consulted in the emergency department for a subocclusive syndrome evolving for six days. On admission, there was a discreet epigastric tenderness with no abdominal distension, and a free rectal bulb.
The physical examination found the following: Respiratory rate: 36 breaths per minute, pulsed oximetry: 92% with 6 L of oxygen, heart rate: 120 bpm, blood pressure: 85/40 mmHg, Glasgow score: 15, and fever: 39.5 °C.
A blood analysis was done showing an anemia 10 g/dL, leukocytosis 20,000 cells/mm3 and an elevated C-reactive protein (CRP) at 300 mg/L. His arterial blood gas test shows a severe metabolic acidosis with hyperlactatemia.
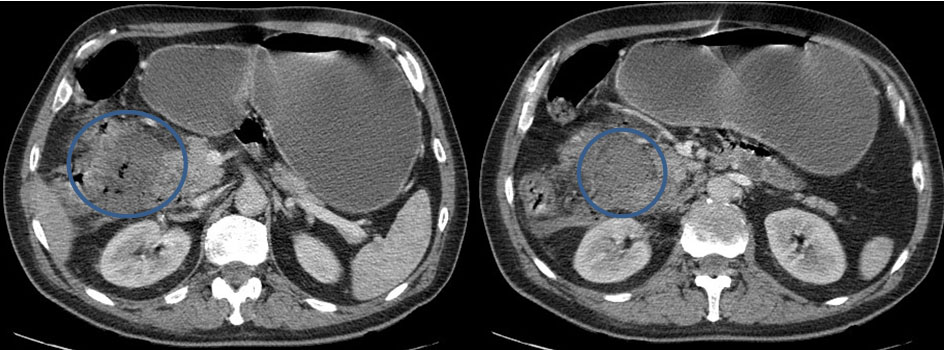
The patient was transferred to the radiology department for an abdominal CT: which has shown a right para-duodenal pseudomass with free anterior air with gastro stasis as well as an infiltration of the anterior aspect of the pancreatic head (Figure 1 and Figure 2). There was no evidence of ileal or colic distension as well as no intraperitoneal bleeding. The diagnosis of covered duodenal perforation was retained.
The patient was transferred to the intensive care unit (ICU), where his ventilation was first ensured via an oxygen mask. Upon this symptomatology, a nasogastric tube was put with aspiration of gastric content, and then a femoral vein cannula, the patient also received a blood transfusion and sodium bicarbonate in order to stabilize his blood pressure.
Due to a development of hypovolemic shock, which did not recede with vasoactive drugs. The decision was to do a laparotomy. A peritoneal lavage was done with an aspiration of the entire peritoneal effusion with collapses of the septate collections. Then a thorough and careful peritoneal lavage with warm physiological saline was performed. A suture of the anterior duodenal perforation and a drainage of the abdominal cavity were ensured by the establishment of a Redon drain. The patient was readmitted to the ICU with a good immediate evolution. But unfortunately, the patient was found dead five days later. The cause of death was attributed to a pulmonary embolism.

Discussion
The duodenum, the first part of the small intestine, extends from the pylorus to the duodenojejunal flexure, known as the Treitz ligament. It is divided into four sections: the duodenal bulb, descending part, transverse part, and ascending part.
Its first part intraperitoneal passes backward and upward toward the neck of the gallbladder [7]. The second part descends 7–8 cm, and is located entirely retroperitoneal. The transverse third part of the duodenum runs 10–12 cm to the left horizontally and is retroperitoneal located in front of the inferior vena cava, lumbar spine, and aorta. The ascending fourth part of the duodenum runs 2–3 cm retroperitoneal and upward to the left. The superior mesenteric vessels run downward over the anterior surface of the third portion of the duodenum [8].
Infectious processes in the duodenum are rarely diagnosed prospectively from CT scans. Most infectious processes result in inflammation of the duodenum and secondary duodenal wall edema.
The most common infectious cause of duodenitis is Helicobacter pylori. The findings tend to be nonspecific, such as wall thickening and luminal dilatation. Correlation with clinical history is helpful in diagnosis.
For the exploration of duodenal pathology, it is preferable to obtain CT scans with the use of radiopaque oral contrast material or negative contrast material (water) to delineate the gastrointestinal tract.
When there is suspicion of a duodenal lesion, several techniques can be used to optimize imaging of this commonly overlooked structure. Oral contrast material is helpful in duodenum opacification [9]. If a mucosal abnormality is suspected, low-attenuation oral contrast agents, such as water or whole milk, can be used [10].
These agents create excellent contrast with the duodenal wall, particularly when intravenous contrast material is injected at 4 mL/s during a dynamic helical acquisition. It is preferable to obtain thinner-collimation images 2.5 mm for the detection of subtle parietal anomalies [4].
Multiplane reconstructions, sagittal and coronal planes are necessary for a complete analysis. Dynamic administration of intravenous contrast material is useful in the identification of vascular structures and the enhancement pattern of lesions within and adjacent to the duodenum [4].
Pancreatic inflammation is the most common inflammatory process to affect the duodenal wall that is adjacent to the pancreatic head. Its main manifestation is wall thickening, which can obstruct the gastric tract, but the severity of the inflammatory state can cause ischemic wall perforation.
In addition, severe pancreatitis can cause an intramural hematoma from disruption of the intramural vasculature by the elastase present in pancreatic enzymes [11]. In Crohn’s disease duodenal perforations are often secondary to fistulous complications from adjacent bowel or from primary duodenal involvement due to parietal ulcerations [12],[13].
The duodenal bulb is the main location of ulcerative diseases. Its perforation can be diagnosed by CT upon detection of free intraperitoneal or retroperitoneal air or duodenal wall thickening [6]. Postbulbar ulcers are rare, and often secondary to Crohn’s disease and Zollinger–Ellison syndrome [4].
Most tumors or gastric inflammatory lesions can be complicated by perforations. Computed tomography is the most sensitive examination for detecting small amounts of extraluminal air, signifying perforation. The air can be perigastric or periduodenal, intraperitoneal, along the gastric ligaments, rarely mesenteric [6].
In duodenal perforations, air is often retroperitoneal or in the right anterior pararenal space [14]. Localized infiltration of peridigestive fat or focal thickening of the gastric or duodenal wall may be a sign of orientation to the origin of the perforation.
Abdominal febrile abdominal pain evolving for several days, which leads fairly quickly in an adult to the realization of a CT scan in search of an etiology. The most frequently observed manifestations are either localized peritonitis in the immediate vicinity of the site of perforation, or more distant manifestations, particularly collections of the superior mesocolic space (subphrenic perihepatic), in the perforations of the bulbar region around the left or perisplenic hepatic lobe, in the perforation cases of the large tuberosity or the body of the stomach [6].
It is of course necessary to continue the exploration up to the perineal plane because it is not exceptional that a perforation of the superior mesocolic space causes the formation of pelvic collections. In subphrenic abscesses, a pleural liquid reaction with passive atelectasis of the overlying lower lobe of the lung is observed, whereas in the deep abdominopelvic collections, reflex ileus may be observed. Intestinal, which can make differential diagnosis problems with organic occlusive syndrome difficult [4],[6].
In recent perforations, air bubbles can be observed even within the peritoneal reaction images, which have a localizing value. In old lesions, we can observe infiltrations of adjacent structures (Glisson capsule and hepatic parenchyma, hepatic pedicle, with possible biliary repercussion, internal digestive fistula) [4],[6].
Perforated ulcers of the posterior surface of the duodenal bulb result in parietal edematous thickening, within an inflammatory infiltration of the duodenopancreatic sulcus region that may be associated with regional gas bubbles and, possibly, with a low pneumoperitoneum. Abundance due to a “blanket” that is still present due to the anatomical situation, but may be incomplete [4],[6].
In such a situation, it is particularly important to search for direct sign of perforation that is the segmental interruption of the mucosa enhanced on the injected images. Recall that these ulcers of the posterior surface of the duodenal bulb can be complicated by a retropneumoperitoneum (which can predominate or be limited to the perirenal lodge, realizing the Valentino syndrome. Perforation can occur in the hepatoduodenal ligament and its contents, including the main bile duct, or in the inferior vena cava [15].
In all doubtful cases, and whatever the location of the suspected lesion, it may be judicious to specify the perforation location, by a digestive tract opacification, which allows to evaluate for potential evolutionary risks, as well as operational difficulties.
Finally, the scanner is a very valuable tool for etiological diagnosis of duodenal perforations related to unusual lesions: ischemic, traumatic, tumors. The main concern of the surgeon in case of complete or incomplete coverture of duodenal perforation is the identification of a tumor etiology as it can completely change its management.
Conclusion
Gastroduodenal perforations in free peritoneum result in pneumoperitoneum, which is usually voluminous, especially if the lesions sit in its anterior surface. Partially covered gastroduodenal perforations result in local changes in the peritoneum corresponding to localized peritonitis. In such cases, however, the ulcerative lesion must be objectified by the localized interruption of mucosal enhancement. These elements are valuable for accurate positive diagnosis, but also for therapeutic management.
REFERENCES
1.
Lau JY, Sung J, Hill C, Henderson C, Howden CW, Metz DC. Systematic review of the epidemiology of complicated peptic ulcer disease: Incidence, recurrence, risk factors and mortality. Digestion 2011;84(2):102–13. [CrossRef]
[Pubmed]

2.
Behrman SW. Management of complicated peptic ulcer disease. Arch Surg 2005;140(2):201–8. [CrossRef]
[Pubmed]
3.
Ansari D, Torén W, Lindberg S, Pyrhönen HS, Andersson R. Diagnosis and management of duodenal perforations: A narrative review. Scand J Gastroenterol 2019;54(8):939–44. [CrossRef]
[Pubmed]
4.
Jayaraman MV, Mayo-Smith WW, Movson JS, Dupuy DE, Wallach MT. CT of the duodenum: An overlooked segment gets its due. Radiographics 2001;21(Suppl 1):S147–60. [CrossRef]
[Pubmed]
5.
Guillem P. Radiologic pneumoperitoneum without perforation of a hollow viscus. [Article in French]. J Chir (Paris) 2002;139(1):5–15.
[Pubmed]
6.
Regent D, Balaj C, Jausset F, Oliver A, Sellal-Aubriot C, Croise-Laurent V. Perforations du tube digestif. Feuillets de Radiologie 2014;54(1):9–31. [CrossRef]
7.
Venkatesh SK, Wan JM. CT of blunt pancreatic trauma: A pictorial essay. Eur J Radiol 2008;67(2):311–20. [CrossRef]
[Pubmed]
8.
Linsenmaier U, Wirth S, Reiser M, Körner M. Diagnosis and classification of pancreatic and duodenal injuries in emergency radiology. Radiographics 2008;28(6):1591–602. [CrossRef]
[Pubmed]
9.
Raptopoulos V. Technical principles in CT evaluation of the gut. Radiol Clin North Am 1989;27(4):631–51.
[Pubmed]
10.
Thompson SE, Raptopoulos V, Sheiman RL, McNicholas MM, Prassopoulos P. Abdominal helical CT: Milk as a low-attenuation oral contrast agent. Radiology 1999;211(3):870–5. [CrossRef]
[Pubmed]
11.
Bellens L, Van Ree H, Vanderstighelen Y, Vanderputte S. Intramural duodenal hematoma of pancreatic origin. Hepatogastroenterology 1999;46(26):930–2.
[Pubmed]
12.
Reynolds HL Jr, Stellato TA. Crohn's disease of the foregut. Surg Clin North Am 2001;81(1):117–35. [CrossRef]
[Pubmed]
13.
Poggioli G, Stocchi L, Laureti S, et al. Duodenal involvement of Crohn's disease: Three different clinicopathologic patterns. Dis Colon Rectum 1997;40(2):179–83. [CrossRef]
[Pubmed]
14.
Hsu CC, Liu YP, Lien WC, Lai TI, Wang HP. A pregnant woman presenting to the ED with Valentino's syndrome. Am J Emerg Med 2005;23(2):217–8. [CrossRef]
[Pubmed]
15.
Choné L, Régent D, Maurer P, Bigard MA. Duodenocaval fistula: A rare complication of a duodenal ulcer. [Article in French]. Gastroenterol Clin Biol 2006;30(3):489–91. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Neftah Camelia - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Edderai Meriem - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Othman Ayouche - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Asaad El Bakkari - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Fabrice Dieukedao - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Fabrice Dieukedao - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Hassan Boumdin - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2020 2020 Neftah Camelia et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}