 |
Case Report
Ultrasound-guided bichectomy: A case report of a novel approach
1 Department of Dental Clinics, Oral Pathology, and Oral Surgery, School of Dentistry, Federal University of Minas Gerais, Belo Horizonte, Brazil
2 Doctor of Dental Surgery, Belo Horizonte, Brazil
3 Department of Morphology, Biological Sciences Institute, Federal University of Minas Gerais, Belo Horizonte, Brazil
4 Doctor of Dental Surgery, Radiologist of the Hermes Pardini Group, Belo Horizonte, Brazil
Address correspondence to:
Alexandre Godinho Pereira
Department of Dental Clinics, Oral Pathology, and Oral Surgery, School of Dentistry, Federal University of Minas Gerais, Rua Prof. Moacir Gomes de Freitas, 688 - 31.270-901, Belo Horizonte, MG,
Brazil
Message to Corresponding Author
Article ID: 101086Z01AP2020
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Pereira AG, Napoli GF, Gomes TB, Rocha LPC, Rocha TDC, e Silva MRMA. Ultrasound-guided bichectomy: A case report of a novel approach. Int J Case Rep Images 2020;11:101086Z01AP2020.ABSTRACT
Introduction: Bichectomy promotes reduction of cheek volume by partial removal of the buccal fat pad. Like any other surgical procedure, there are inherent risks that can lead to severe complications. To minimize those risks, a novel approach using real-time ultrasonography (US) imaging during the procedure was performed on a difficult bichectomy case with anatomical variation in the buccal fat pad position.
Case Report: A 25-year-old female patient was referred for bichectomy on her left cheek. An ultrasound scan was performed and an anatomical variation in position was detected. The patient’s left buccal fat pad was located deep in the masseteric area and in close relationship with branches from the facial vein and the transverse facial artery. Since there was an increased risk to perform the surgery, a guided bichectomy was performed using real time ultrasound imaging to guide the initial incision, location, and excision. The procedure was performed without any complication and the clinical success was assessed by ultrasonography in the postoperative period.
Conclusion: The US performed during the surgery made it possible to safely access and remove the buccal extension with minimal risk for the patient. The ultrasound proved to be useful to demonstrate the relationship among the buccal fat pad and adjacent structures and to detect anatomical variation in its position, allowing a safer surgical procedure to be performed
Keywords: Adipose tissue, Case report, Face, Lipectomy, Ultrasonography
Introduction
Bichat’s ball or buccal fat pad (BFP) is a lobulated, encapsulated adipose structure consisting of a central body and four extensions: temporal, pterygopalatine, pterygoid, and buccal [1]. Its buccal extension is located in the central portion of the submalar triangle and it is considered one of the key elements of the facial contour, responsible for providing volume to the middle third of the face [1],[2].
Recently, the surgical removal of the buccal extension of the BFP for aesthetic purposes has become very popular [2]. This technique, known as bichectomy, promotes a reduction in the volume of the submalar region, emphasizing the zygomatic prominence and, thus, allowing for the triangulation of the facial profile [2],[3],[4],[5].
Generally, the excision of the BFP is performed through an intraoral incision and has low complication rate [6]. However, some severe complications are reported in the literature, such as facial asymmetry [4], parotid gland injury [7], nerve lesions [8],[9], and severe arterial bleeding [10].
With the development of high-resolution real-time portable ultrasound, the US assessment at the medical or dental office became viable, allowing healthcare professionals to assess and treat conditions simultaneously. While being assisted by real-time US, it achieves a safer and less invasive procedure [11],[12].
The present case report presents a novel approach using real-time US to safely guide the incision and removal of the BFP’s buccal extension in a patient with anatomical variation of the BFP’s position. It also highlights the benefits of US as an adjunctive diagnostic tool.
Case Report
The present article has been reported in line with the SCARE guidelines [13]. A 25-year-old female patient was referred for the bichectomy procedure on her left cheek. It was verified in the medical records that the patient had undergone a bilateral bichectomy procedure 14 days before. However, her left BFP was not located and thus not removed during the procedure. It is noteworthy that the patient reported not having systemic diseases nor taking any medications.
In order to verify the location and volume of the left BFP, and the need to perform a new bichectomy, an US assessment of the left-side middle third of the face was performed.
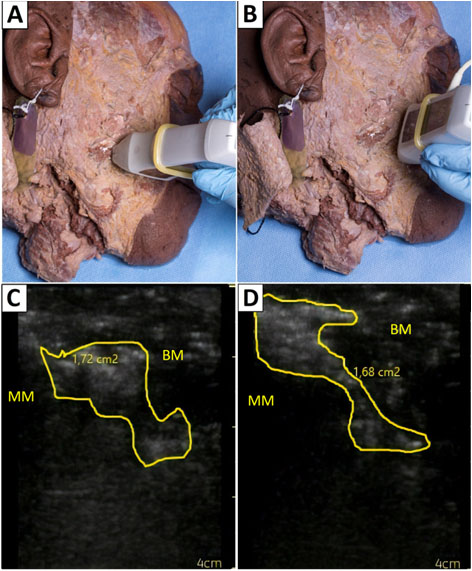
The images were obtained by an experienced radiologist through a Vscan™ Ultrasound System with Dual Probe (GE-Vingmed Ultrasound AS, Norway) 10 Volt–1.5 Ampere. The transducer was placed in both the transverse and the longitudinal directions (Figure 1A, Figure 1B) to properly determine BFP location, extent, as well as its relation to the neighboring structures.
During the US, it was verified that the BFP presented an anatomical variation in its position, situated in the posterior submalar region, deep into the masseter region, at the height level of the third upper molar (Figure 1C). Moreover, it was possible to confirm the close relationship of the BFP with other structures, such as the facial vein, the transverse facial artery, and the buccinator muscle (Figure 1C, Figure 1D).
The image assessment confirmed the need to perform the bichectomy and showed the need for a different surgical access due to the anatomical variation.
The surgical procedure was performed by a dental surgeon with experience in orofacial harmonization and having two years of specialized bichectomy training, and also assisted by a radiologist. The incision site was defined based on the BFP location assessed by US. The evaluation of the selected area was performed with colorimetric Doppler exam to ensure the absence of large blood vessels near the incision site.
The patient underwent local anesthesia using the tumescent technique with 3% lidocaine (1: 50,000). A vertical incision was made in the buccal (jugal) mucosa of the region approximately 20 mm posterior to the parotid papilla, through the buccinator muscle, with surgical scalpel blade No. 15.
Assisted by US imaging, a careful tissue dissection was made, locating the capsule of the buccal extension and it was incised for herniation of the BFP through the surgical access. The buccal extension of the BFP was clamped, carefully pulled, and excised.
The submalar region was then immediately checked with US for the assessment of the tissue condition and the remaining volume. The examination confirmed the buccal extension removal, as it can be seen through the comparison between the pre-bichectomy (Figure 1C, Figure 1D) and the post-bichectomy echographic images (Figure 2A, Figure 2B).
After the examination, the surgical access was closed with two simple interrupted sutures and the patient was medicated and instructed about the postoperative care. No complaints were related by the patient regarding the use of US prior, during, or after the surgery.
The patient was scheduled seven days after the bichectomy procedure for suture removal. At that time, no clinical evidence of edema or infection was observed, and the patient stated that the postoperative period was well tolerated and with no complications or adverse effects.
One hundred and eight days after the procedure, US was performed once again by the same radiologist and the clinical success of the procedure was determined (Figure 2C, Figure 2D). The patient also stated that she was very satisfied with the outcome.


Discussion
The use of US prior to bichectomy surgeries has been reported in the literature [2],[3]. However, in this approach, US became more than an external diagnostic tool, directly assisting in real time the execution of the surgical procedure.
During the procedure, US made it possible to locate the masseter and buccinator muscles, which are reference muscles for the determination of the BFP, as well as to avoid possible hemorrhage complications by using the colorimetric Doppler to identify potential blood vessels close to the incision site.
Since the BFP is close to several important anatomical structures [14],[15], it can be speculated that a surgical exploration without the assistance of US has the potential to lead to serious complications [6],[10],[16]. This can be verified in the literature, which shows that the rate of complications reported during bichectomy surgeries is approximately 8.45% [6]. Among these complications, the most common are over-resection [16], parotid gland injury [7], trismus [4], facial asymmetry [4], lesion of the buccal and zygomatic branches of the facial nerve [8],[9] severe bleeding of the buccal [7], and maxillary arteries [10].
In this context, lesions in any of the structures adjacent to the BFP can have extremely harmful effects, compromising the success of the procedure and, ultimately, leading to the need for emergency medical care to solve the most serious complications that can be life-threatening [10].
Ultrasonography has extensive benefits because it is a fast, affordable exam, without contraindications [17]. It is a well-established diagnostic method for soft tissue analysis [3]. Furthermore, the US also proved to be helpful during the preoperative and postoperative phases.
In the preoperative phase, US allowed the verification of the large volume of the BFP buccal extension and the presence of anatomical variation in its position. The buccal extension was located deep into the masseter region in the posterior submalar region, and not between the masseter and buccinator muscles as it is generally found [1].
In order to exemplify, US was performed in an anatomical piece from the Human Anatomy laboratory of the Department of Morphology of the Institute of Biological Sciences of the Federal University of Minas Gerais (ICB/UFMG). It was possible to observe the normal position of the BFP (Figure 3C, Figure 3D) in comparison with the anatomical variation from the present case report (Figure 1C, Figure 1D). It is important to note that this procedure did not require approval from the institutional ethics committee, since the available material was used for scientific purposes, while respecting human cadavers and ethical principles [18],[19],[20].
The determination for the need for bichectomy can be challenging, since the excessive volume of the facial profile may be due to a masseteric hypertrophy, to individual skeletal anatomy or even due to pathological conditions [2],[5]. Therefore, the clinical analysis alone may not be able to fully evaluate the characteristics of the superficial and deep structures for an adequate diagnosis. Thus, the use of a complementary imaging diagnostic tool, such as the US, proves to be useful [2],[3].
In the postoperative period—immediately after the surgery and afterward—the US allowed the verification of the remaining adipose tissue extent and of the adjacent tissue conditions, thus determining the clinical success of the procedure.
Conclusion
The bichectomy assisted by real time ultrasonography presented many advantages, being particularly useful in locating the BFP and its relationship with neighboring structures, assisting in surgical decision-making, guiding the surgical procedure and performing immediate and long-term postoperative assessment. Therefore, the present case report emphasizes the importance of US as an adjunctive diagnostic tool and highlights its great potential for reducing complications during the bichectomy. It is suggested that this examination should be part of the surgical protocol.
REFERENCES
1.
Loukas M, Kapos T, Louis RG Jr, Wartman C, Jones A, Hallner B. Gross anatomical, CT and MRI analyses of the buccal fat pad with special emphasis on volumetric variations. Surg Radiol Anat 2006;28(3):254–60. [CrossRef]
[Pubmed]

2.
Sezgin B, Tatar S, Boge M, Ozmen S, Yavuzer R. The excision of the buccal fat pad for cheek refinement: Volumetric considerations. Aesthetic Surg J 2019;39(6):585–92. [CrossRef]
[Pubmed]
3.
Jaeger F, Castro CHBC, Pinheiro GM, et al. A novel preoperative ultrasonography protocol for prediction of bichectomy procedure. Arq Bras Odontol 2016;12(2):7–12.
4.
Benjamin M, Reish RG. Buccal fat pad excision: Proceed with caution. Plast Reconstr Surg Glob Open 2018;6(10):e1970. [CrossRef]
[Pubmed]
5.
Tarallo M, Fallico N, Maccioni F, et al. Clinical significance of the buccal fat pad: how to determine the correct surgical indications based on preoperative analysis. Int Surg J 2018;5(4):1192–4. [CrossRef]
6.
Hwang K, Cho HJ, Battuvshin D, Chung IH, Hwang SH. Interrelated buccal fat pad with facial buccal branches and parotid duct. J Craniofac Surg 2005;16(4):658–60. [CrossRef]
[Pubmed]
7.
Vieira GM, Jorge FD, Franco EJ, Dias LDC, Guimarães MCDM, Oliveira LA. Lesions of the parotid gland and buccal artery after buccal fat pad reduction. J Craniofac Surg 2019;30(3):790–2. [CrossRef]
[Pubmed]
8.
Tapia A, Ruiz-de-Erenchun R, Rengifo M. Combined approach for facial contour restoration: Treatment of malar and cheek areas during rhytidectomy. Plast Reconstr Surg 2006;118(2):491–7. [CrossRef]
[Pubmed]
9.
Klüppel L, Marcos RB, Shimizu IA, da Silva MAD, da Silva RD. Complications associated with the bichectomy surgery. RGO - Rev Gaúch Odontol 2018;66(3):278–84. [CrossRef]
10.
Engdahl R, Nassiri N, Mina B, Drury J, Rosen R. Superselective microcatheter embolization of hemorrhage after buccal lipectomy. Aesthetic Plast Surg 2012;36(3):742–5. [CrossRef]
[Pubmed]
11.
Pilecki Z, Koczy B, Mielnik M, Pilecki G, Dzielicki J, Jakubowski W. Basic dissecting techniques in ultrasound-guided surgery. J Ultrason 2014;14(57):171–8. [CrossRef]
[Pubmed]
12.
Yusa H, Yoshida H, Ueno E, Onizawa K, Yanagawa T. Ultrasound-guided surgical drainage of face and neck abscesses. Int J Oral Maxillofac Surg 2002;31(3):327–9. [CrossRef]
[Pubmed]
13.
Agha RA, Borrelli MR, Farwana R, Koshy K, Fowler A, Orgill DP, SCARE Group. The SCARE 2018 statement: Updating consensus surgical case report (SCARE) guidelines. Int J Surg 2018;60:132–6. [CrossRef]
[Pubmed]
14.
Custodio AL, Silva MR, Abreu MH, Araújo LR, de Oliveira LJ. Styloid process of the temporal bone: Morphometric analysis and clinical implications. Biomed Res Int 2016;2016:8792725. [CrossRef]
[Pubmed]
15.
Martins-Júnior PA, Rodrigues CP, Da Maria ML, Nogueira LM, Silva JH, Silva MR. Analysis of anatomical characteristics and morphometric aspects of infraorbital and accessory infraorbital foramina. J Craniofac Surg 2017;28(2):528–33. [CrossRef]
[Pubmed]
16.
Coutinho DCO, Martins-Júnior PA, Campos I, Custódio ALN, Silva MRMAE. Zygomaticofacial, zygomaticoorbital, and zygomaticotemporal foramina. J Craniofac Surg 2018;29(6):1583–7. [CrossRef]
[Pubmed]
17.
Robinson TM. Basic principles of ultrasound. In: Lemoigne Y, Caner A, Rahal G, editors. Physics for Medical Imaging Applications. NATO Science Series, Volume 240. Dordrecht: Springer; 2007. p. 101–10.
18.
Yousuf S, Tubbs RS, Wartmann CT, Kapos T, Cohen-Gadol AA, Loukas M. A review of the gross anatomy, functions, pathology, and clinical uses of the buccal fat pad. Surg Radiol Anat 2010;32(5):427–36. [CrossRef]
[Pubmed]
19.
Zhang HM, Yan YP, Qi KM, Wang JQ, Liu ZF. Anatomical structure of the buccal fat pad its clinical adaptations. Plast Reconstr Surg 2002;109(7):2509–18. [CrossRef]
[Pubmed]
20.
Matarasso A. Managing the buccal fat pad. Aesthet Surg J 2006;26(3):330–6. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Alexandre Godinho Pereira - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Gregory Fernandes Napoli - Acquisition of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Thiago Bissoli Gomes - Acquisition of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Luiz Paulo Carvalho Rocha - Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Tânia de Carvalho Rocha - Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Micena Roberta Miran Alves e Silva - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2020 Alexandre Godinho Pereira et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}