 |
Case Report
A rare case of solitary optic nerve sarcoidosis mimicking an ocular tumor
1 Assistant Professor of Medicine, Department of Interdisciplinary Oncology, Moffitt Cancer Center, 12902 Magnolia Drive, Tampa, Florida, USA
2 Oncologic Surgical Pathology Fellow, Department of Pathology, Moffitt Cancer Center, 12902 Magnolia Drive, Tampa, Florida, USA
3 Chair of Medicine, Associate Professor of Medicine, Department of Interdisciplinary Oncology, Moffitt Cancer Center, 12902 Magnolia Drive, Tampa, Florida, USA
Address correspondence to:
Jacqueline Wesolow
Assistant Professor of Medicine, Department of Interdisciplinary Oncology, Moffitt Cancer Center, 12902 Magnolia Drive, Tampa, Florida 33612,
USA
Message to Corresponding Author
Article ID: 101076Z01JW2019
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Wesolow J, Allen N, Ramsakal A. A rare case of solitary optic nerve sarcoidosis mimicking an ocular tumor. Int J Case Rep Images 2019;10:101076Z01JW2019.ABSTRACT
Introduction: Sarcoidosis is often an overlooked differential diagnosis in many disease processes. It is a nonspecific inflammatory disease marked by granulomas. Being nonspecific makes it a more difficult disease to diagnose. It is a challenging diagnosis as it is a great mimicker of many other conditions and therefore missed. The finding of a granuloma is not specific for sarcoidosis as other disorders may present with granulomas. It is an important differential to keep in mind because of significant morbidity and mortality associated with this disease.
Case Report: Here we present a case of a female patient with vision loss and an intracranial mass. The mass was initially thought to be cancer and hence referred to our Cancer Center for further evaluation and workup. Upon biopsy the mass was diagnosed as sarcoidosis. She had no other systemic involvement at time of diagnosis. What makes this case of sarcoidosis rare is her solitary optic nerve involvement.
Conclusion: Sarcoidosis is a more difficult disease to diagnose than other diseases, such as coronary artery disease, hyperlipidemia, and diabetes as these diseases have very specific, easily accessible laboratory values, and imaging modalities for fairly quick and simple testing. These disorders rely on hemoglobin A1C, electrocardiograms, troponin values, cholesterol level, which, unlike sarcoidosis testing, are relatively inexpensive and disease specific. This case report highlights an unusual presentation of sarcoidosis and reminds the physician to not forget this in the differential diagnosis.
Keywords: Cancer, Granuloma, Ocular sarcoidosis, Sarcoidosis
Introduction
Sarcoidosis is an inflammatory disease characterized by the presence of noncaseating granulomas. Granulomas are the pathologic hallmark of sarcoidosis. Microscopically, granulomas are a local accumulation of inflammatory cells [1]. The disease is often multisystem and requires involvement in two or more organs for diagnosis. The finding of granulomas is not specific for sarcoidosis and other known etiologies of granulomas need to be ruled out. Other granulomatous diseases include primary biliary cirrhosis, Peyronie’s disease, Blau’s syndrome, and immune complex disease, certain mycobacterial and fungal infections, malignancy, and environmental agents, such as beryllium [2]. The clinical outcome of sarcoidosis varies, with remission occurring in over one-half of the patients within a few years of diagnosis; however, the remaining patients may develop a chronic form of the disease. Solitary ocular nerve involvement is rare as in our case report.
The etiology of sarcoidosis remains unknown although ongoing studies are being done. It is seen all around the world. The higher incidences are reported in Northern Europeans and African-Americans with the lowest in the Japanese population [1]. African-Americans typically experience a more extreme form of the disease compared to Caucasians [1]. Women are more affected than men worldwide [1]. It is usually found in young adults who are overall and otherwise healthy. Most cases are sporadic, but a familial form of the disease does exist [1].
Patients can remain asymptomatic or manifest with organ failure depending on location of disease. While sarcoidosis can affect almost every organ of the body, the lung is most commonly affected [3]. Other organs affected are the skin, liver, and eye. Direct infiltration of the optic nerve by sarcoid granulomas is a rare optic nerve manifestation of sarcoidosis.
Case Report
A 47-year-old female police officer was referred to our Neurosurgery clinic at our cancer center after a magnetic resonance imaging (MRI) brain revealed evidence of an intracranial mass involving the left optic nerve. Imaging showed a 1.8 × 1.39 cm enhancing suprasellar lesion that extended to the left optic nerve with enlargement of her optic sheath. Her symptoms began with left eye blurriness and progressed to loss of vision of her left eye. She reported migraines, taking rizatriptan for them. She was otherwise in good health. She denied shortness of breath, chest pain, cough, wheezing, abnormal balance, confusion, numbness, or tingling. Her other medical history included cervical radiculopathy and genital herpes simplex. She never smoked.
On physical exam she was alert, oriented, and her extraocular movements were intact. She had normal hearing and her lungs were clear to auscultation. Her neurologic examination revealed that her cranial nerves II through XII were intact with the exception of her left ocular findings. She had minimal pupillary response to direct testing. She had left visual field loss. The patient was only able to identify light and dark from the left side of her left eye. Her speech remained clear and coherent. Chest radiograph was clear of infiltrates.
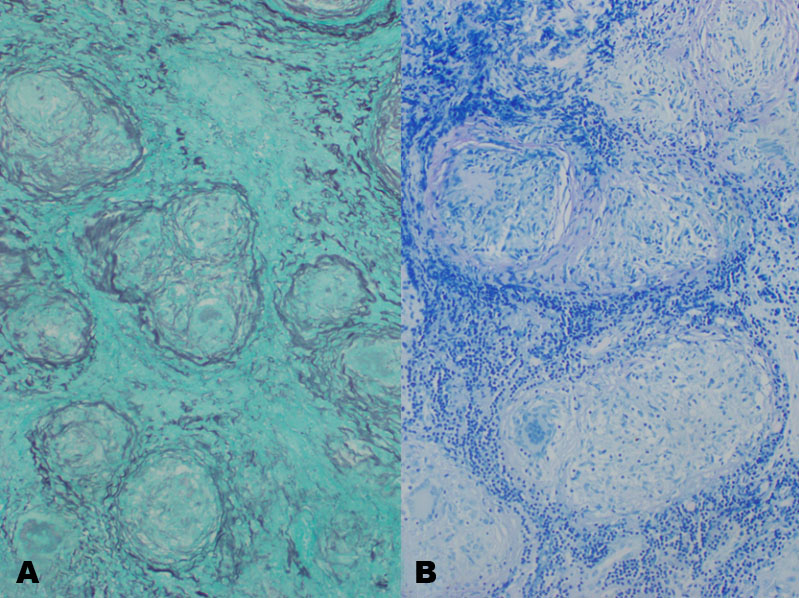
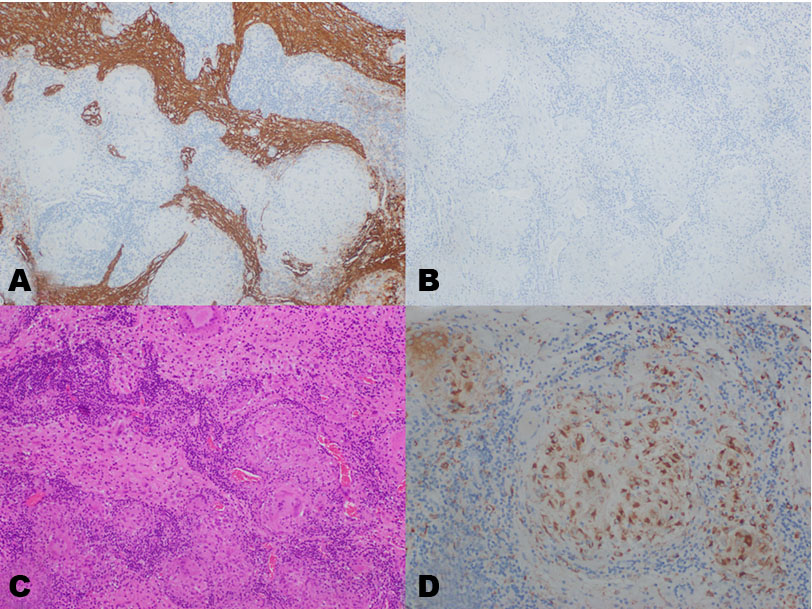
She underwent a left-sided craniotomy with open biopsy and resection of the left optic mass using stereotactic navigation and microdissection technique. Biopsy of the left optic nerve tumor revealed noncaseating granulomas favoring sarcoidosis. Figure 1 shows the biopsy H&E slides. Figure 2 shows the GMS and AFB stains are negative, supporting a noninfectious cause for the granulomas. Figure 3 shows stains for GFAP being positive within residual gliotic optic nerve. However, neurofilament is negative, indicating complete axonal loss. This is supported by the absence of myelin with an LFB stain. CD68 highlights histiocytes within the granulomas.
The patient was placed on high-dose corticosteroids. Her neurologic exam remained stable with motion lost in the left eye, no other neurologic deficits. She was started on Keppra 2000 mg tablets twice daily for seizure prophylaxis. She was discharged on postoperative day 2 in stable condition.

Discussion
The most common ocular manifestations of sarcoidosis are uveitis, dry eye, and conjunctival nodules. Anterior uveitis being much more common in comparison to posterior uveitis [4]. Other clinical manifestations include episcleritis, scleritis, retinitis, retinal vasculitis, macular edema, and cataract formation. Anterior chamber inflammation is one of the most clinical signs of sarcoid uveitis. It was detected in >90% patients with biopsy-proven sarcoid uveitis in one study [5]. Typical clinical presentations in patients with anterior chamber inflammation can include pain, erythema, and worsening vision [6].
Management of ocular sarcoidosis includes corticosteroids, systemic immunosuppressive agents, biologic agents, and surgery [7]. Injectable and topical corticosteroids are the first line treatment for ocular sarcoidosis [7]. Injectionables include subconjunctival, periocular, and intravitreal types. Topical treatments include prednisolone acetate and difluprednate and used mainly for treatment of anterior uveitis. In patients who do not tolerate or have poor results from topical corticosteroids or suffer from posterior uveitis can be treated with injectables. Dexamethasone or a sustained-release fluocinolone acetonide implant can also be considered for these patients. In patients who poorly respond to corticosteroid therapy, systemic immunosuppressive, or biologic agents are an option. The immunosuppressive agents include methotrexate, azathioprine, cyclosporine, and tacrolimus. Biologics include infliximab, adalimumab, etanercept, and certolizumab. Biologic agents are last resort as there have not been well documented long-term safety effects on them. Surgery can be used in cases resistant to abovementioned medications [7].
In comparison of other case report studies of ocular sarcoidosis most case reports reviewed, patients usually presented with ocular pain. In one of the case reports of a 54-year-old woman, she presented with decreased vision, photophobia, and eye pain for one month [8]. Our patient had loss of vision as well in the effected eye. In her case, therapy included prednisone as well as methotrexate. Both ocular and systemic symptoms improved with treatment [8]. In another case report, a 27-year-old woman presented with headache, fevers, and bilateral painful upper eyelid edema for two months. She also had bilateral ocular pain for seven days [5]. In addition to ocular manifestation of sarcoidosis, this patient also had pulmonary involvement as do most patients in case reports. This is unlike our patient who presented with unique and rare solitary optic nerve sarcoidosis. This patient was treated successfully with prednisone and methotrexate.
Conclusion
Solitary optic nerve involvement of sarcoidosis is rare. It prevents a diagnostic challenge solvable only by biopsy as in our patient who presented with progressive visual loss and eye pain. It can be mistaken for a tumor as was initially thought in our patient and hence her referral to our Cancer Center. Sarcoidosis should be considered and kept in the differential in these patients, especially ones who present with uveitis or ocular pain. Anterior uveitis is the most common ocular manifestation. In comparison to other case reports, our patient was similar in that she presented with eye pain. Our case was unique however in that she had a rare isolated solitary optic nerve sarcoid tumor mimicking cancer without any other systemic manifestations.
REFERENCES
1.
Jayakrishnan B, Al-Busaidi N, Al-Mubaihsi S, Al-Rawas OA. Sarcoidosis in the Middle East. Ann Thorac Med 2019;14(2):106–15. [CrossRef]
[Pubmed]

2.
James DG. A clinicopathological classification of granulomatous disorders. Postgrad Med J 2000;76(898):457–65. [CrossRef]
[Pubmed]
3.
Swigris JJ, Olson AL, Huie TJ, et al. Sarcoidosis-related mortality in the United States from 1988 to 2007. Am J Respir Crit Care Med 2011;183(11):1524–30. [CrossRef]
[Pubmed]
4.
Moschos MM, Guex-Crosier Y. Anterior segment granuloma and optic nerve involvement as the presenting signs of systemic sarcoidosis. Clin Ophthalmol 2008;2(4):951–3. [CrossRef]
[Pubmed]
5.
Hickman SJ, Quhill F, Pepper IM. The evolution of an optic nerve head granuloma due to sarcoidosis. Neuroophthalmology 2016;40(2):59–68. [CrossRef]
[Pubmed]
6.
Peres MB, Sousa JM, Nascimento H. Ocular sarcoidosis masked by positive IgM for toxoplasmosis. Arq Bras Oftalmol 2017;80(2):125–7. [CrossRef]
[Pubmed]
7.
Yang SJ, Salek S, Rosenbaum JT. Ocular sarcoidosis: New diagnostic modalities and treatment. Curr Opin Pulm Med 2017;23(5):458–67. [CrossRef]
[Pubmed]
8.
You C, Ma L, Anesi SD. Bilateral papillitis and vitritis as the initial ophthalmologic finding in a patient with complex medical history, leading to diagnosis of multisystem sarcoidosis. Am J Ophthalmol Case Rep 2018;13:122–6. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Jacqueline Wesolow - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Nichole Allen - Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Asha Ramsakal - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2019 Jacqueline Wesolow et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}