 |
Case Report
Systemic air embolism during endoscopic retrograde cholangiopancreatography with myocardial and cerebral ischemia
1 MD, Department of Internal Medicine, University Hospital Osijek, Osijek, Croatia
2 Faculty of Medicine, University J.J. Strossmayera Osijek, Osijek, Croatia
3 MD and PhD, Department of Internal Medicine, University Hospital Osijek, Osijek, Croatia
Address correspondence to:
Lana Maričić
Department of Internal Medicine, University Hospital Osijek, J. Huttlera 4, Osijek,
Croatia
Message to Corresponding Author
Article ID: 101075Z01DM2019
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Mihić D, Marićič L, Loinjak D. Systemic air embolism during endoscopic retrograde cholangiopancreatography with myocardial and cerebral ischemia. Int J Case Rep Images 2019;10:101075Z01DM2019.ABSTRACT
Introduction: Endoscopic retrograde cholangiopancreatography (ERCP) has become the primary tool for the treatment of biliary and pancreatic stone diseases. Systemic air embolisms are a rare, but often a fatal complication of ERCP.
Case Report: We present a 56-year-old woman, who was hospitalized for routine, elective ERCP due to recurrent cholangitis. The procedure complicated by development systemic air embolism with myocardial and cerebral ischemia. A transesophageal ultrasound was confirmed patent foramen ovale (PFO). Magnetic resonance imaging (MRI) of brain was done and it showed numerous zones of relatively fresh ischemic lesions through both hemispheres of the brain. The patient has survived but with serious consequences. One year after the incident, the patient presented with paresis of the right hand, walking with the assistance.
Conclusion: Systemic air embolism presents a rare, but lifethreatening complication, particularly with persons at an increased risk, that is, with a left-to-right shunt.
Keywords: Air embolism, Cerebral ischemia, Endoscopic retrograde cholangiopancreatography, Myocardial infarction
Introduction
Endoscopic retrograde cholangiopancreatography has become the primary tool for the treatment of biliary and pancreatic stone diseases. It is essential for the endoscopist carrying out the ERCP to have a thorough understanding of the potential adverse events. Systemic air embolisms are a rare, but often a fatal complication of ERCP. Risk factors associated with air embolisms in this setting include situations where the mucosa is damaged or where high pressure is generated in the gastrointestinal tract [1]. In the systematic review in the PubMed database, air embolism after endoscopy is found in 60% of patients who underwent ERCP. In 46% of documented echocardiography, a PFO has been confirmed as the mechanism of paradoxical air embolism. Only 55% of patients survived systemic air embolism [2].
Case Report
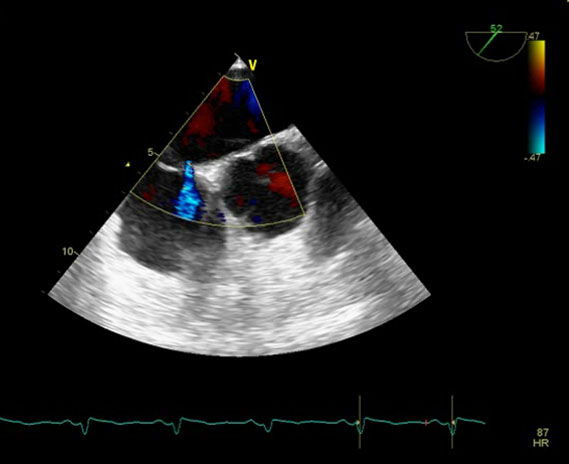
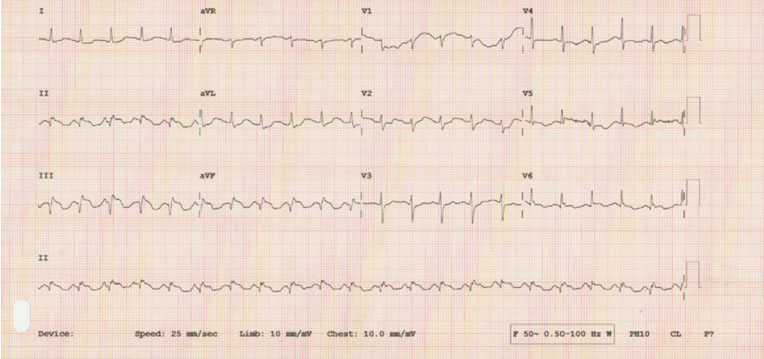
A 56-year-old woman was hospitalized for routine, elective ERCP due to recurrent cholangitis. The patient in question had previously undergone cholecystectomy and had been subjected to ERCP two times because of repeated episodes of cholelithiasis, the last time was two years ago. Preoperative assessment was done neatly, and as an introduction to anesthesia the patient was given premedication (fentanyl, propofol, and rocuronium). Fifteen minutes after the beginning of the procedure, a sudden drop of blood pressure occurs and the saturation of arterial blood with oxygen decreases to 65%, the end-tidal carbon dioxide (CO2) drops, accompanied by the loss of peripheral and central pulsations. Cardiopulmonary reanimation according to the Advanced Life Support (ALS) protocol was initiated, after which palpable peripheral pulses were achieved, accompanied by vasoactive support. A computed tomography (CT) of the brain and a CT pulmonary angiography were done at once. During the procedure, the blood pressure dropped again and cardiopulmonary reanimation was conducted again. After 10 minutes, there was a pulse rate of about 100/min, the patient was hemodynamically stable and the O2 saturation of 90% was restored. The CT angiography showed a considerable amount of gas within the right atrium and the ventricles, a minimal amount inside the pulmonary trunk, and a somewhat smaller amount inside the ascending aorta. The CT of the brain confirmed, along the left hemisphere of the brain, primarily subdural, clusters of gas content (Figure 1). Immediately, a central vein catheter was placed into the right internal jugular vein and an air aspiration under the ultrasound control is attempted. During the following course of hospitalization, the patient was placed into the intensive care unit. All the time, she was ventilated with 100% oxygen, held in left lateral position together with Trendelenburg position. The patient underwent transthoracic cardiac ultrasound which confirmed preserved systolic function left ventricular ejection fraction (LV EF) 60%, aneurysm of interatrial septum, which expanded to the right atrium. A transesophageal ultrasound of the heart was made and hereby a PFO was detected (Figure 2). An electrocardiography was showed ST elevation in inferolateral leads (Figure 3), also cardiac enzyme levels were noted (CK 6285 U/L, CK-MB 571 U/L, troponin I 647.262 μg/L). Coronarography did not confirm significant stenosis of epicardial arteries. The following day, an MRI of brain was done and it showed numerous zones of relatively fresh ischemic lesions through both hemispheres of the cerebellum, through both hemispheres of the brain, as well as in the area of basal ganglia on the left side (Figure 4). The distribution of the lesions was dominantly cortical. During the next few days, the patient was unconscious, mechanically ventilated in volume controlled-synchronized intermittent mandatory ventilation (VC-SIMV) mode, treated with the vasoactive and anti-edematous therapy. On the ninth day of the hospitalization, the patient was removed from the mechanical ventilation. Gradually, the recovery of the patient and the level of consciousness were monitored, followed by considerable psycho-organic changes. The further treatment of the patient was continued by carrying out neurorehabilitation, and after two months there was a remaining tetraplegia, with a mild motoric dysphasia. The patient was still undergoing a neurorehabilitation treatment in a specialized institution. One year after the incident, the patient presented with paresis of the right hand, walking with the assistance.


Discussion
We presented a case of systematic air embolism, which affects arterial and venous system, with an ensuing development of cerebral ischemia and acute myocardial infarction in a patient with a previously unknown PFO, who was subjected to ERCP. Until now, around 30 cases have been published in which air embolism occurred as an ERCP complication. Half of the described cases ended with a fatal outcome [3],[4]. The cases which dealt primarily with air embolism that affects cerebral arteries have been described and in one case it was a massive one, with a simultaneous development of cerebral and cardiac ischemia [5]. Unlike our case, the patient did not undergo an echocardiographic treatment, nor was the PFO confirmed. Based on the described cases, the age and the attached comorbidity of the ill person did not pose a significant risk factor for developing air embolism, but the existence of a left-to-right shunt, that is, the arteriovenous junction, is definitely a very important risk factor. The concurrent entrainment of the arteriovenous circulation is almost impossible, unless there is a left-to-right junction. Considering the severe consequences of the systemic air embolism, which in a large number of cases can be fatal, it can be concluded that the prevention and the preparation for the procedure might reduce mortality to a certain extent. Patent foramen ovale is found in 20% of general population, and it is in these patients that the risk of fatal outcome and serious consequences is greatest [6]. So, the question arises whether, as a part of the preparation for an EPRC, a transesophageal ultrasound of the heart should be done in order to detect the existence of a left-to-right shunt [7]. The American Society for Gastrointestinal Endoscopy issued a recommendation for the application of CO2 with the purpose of insufflation instead of air, especially concerning persons at an increased risk for air embolism and perforation [8].
Conclusion
Systemic air embolism presents a rare, but life-threatening complication, particularly with persons at an increased risk, that is, with a left-to-right shunt.
REFERENCES
1.
Bechi A, Nucera MP, Olivotto I, Manetti R, Fabbri LP. Complete neurological recovery after systemic air embolism during endoscopic retrograde cholangiopancreatography. Minerva Anestesiol 2012;78(5):622–5.
[Pubmed]

2.
Voigt P, Schob S, Gottschling S, Kahn T, Surov A. Systemic air embolism after endoscopy without vessel injury – A summary of reported cases. J Neurol Sci 2017;376:93–96. [CrossRef]
[Pubmed]
3.
Donepudi S, Chavalitdhamrong D, Pu L, Draganov PV. Air embolism complicating gastrointestinal endoscopy: A systematic review. World J Gastrointest Endosc 2013;5(8):359–65. [CrossRef]
[Pubmed]
4.
Park S, Ahn JY, Ahn YE, et al. Two cases of cerebral air embolism that occurred during esophageal ballooning and endoscopic retrograde cholangiopancreatography. Clin Endosc 2016;49(2):191–6. [CrossRef]
[Pubmed]
5.
van Boxel GI, Hommers CE, Dash I, Goodman AJ, Green J, Orme RM. Myocardial and cerebral infarction due to massive air embolism folllowing endoscopic retrograde cholangiopancreatography (ERCP). Endoscopy 2010;42 Suppl 2:E80–1. [CrossRef]
[Pubmed]
6.
Wills-Sanin B, Cárdenas YR, Polanco L, Rivero O, Suarez S, Buitrago AF. Air embolism after endoscopic retrograde cholangiopancreatography in a patient with budd Chiari syndrome. Case Rep Crit Care 2014;2014:205081. [CrossRef]
[Pubmed]
7.
Bastovansky A, Stöllberger C, Finsterer J. Fatal cerebral air embolism due to a patent foramen ovale during endoscopic retrograde cholangiopancreatography. Clin Endosc 2014;47(3):275–80. [CrossRef]
[Pubmed]
8.
Gómez C, Cuyàs B, Bazaga S, Iborra G, Murzi M. Endoscopic retrograde cholangiopancreatography-related air embolism in a patient with an unknown biliary – venous fistula and patent foramen ovale: A case report. Ann Clin Case Rep 2016;1:1118.
SUPPORTING INFORMATION
Author Contributions
Damir Mihić - Conception of the work, Design of the work, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Lana Maričić - Conception of the work, Design of the work, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Domagoj Loinjak - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2019 Damir Mihić et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}