 |
Case Report
A case report of a large odontogenic cyst treated by dental implantation with mandibular reconstruction using an iliac bone graft
1 Department of Dentistry and Oral Surgery, Tokyo Metropolitan Hospital Organization, Tokyo Metropolitan Toshima Hospital, Tokyo, Japan
Address correspondence to:
Hikaru Takahashi
Department of Dentistry and Oral Surgery, Tokyo Metropolitan Hospital Organization, Tokyo Metropolitan Toshima Hospital, 33-1 Sakaecho, Itabashi-ku, Tokyo 173-0015,
Japan
Message to Corresponding Author
Article ID: 101499Z01HT2025
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Takahashi H, Takaku Y. A case report of a large odontogenic cyst treated by dental implantation with mandibular reconstruction using an iliac bone graft. Int J Case Rep Images 2025;16(1):54–59.ABSTRACT
Odontogenic cysts are comparatively common, but large odontogenic cysts that extend into the unilateral mandible are rare. Here, we present the case of a patient with a large odontogenic cyst extending to the unilateral mandible by enucleation and mandibular reconstruction with an iliac bone graft, followed by occlusal reconstruction by dental implant treatment. The patient was a 69-year-old man who presented to a local dental clinic with swelling and increasing pain in the right mandible. Radiolucency in the right lower molar region and impacted wisdom teeth were identified, and he was referred to our department. A panoramic X-ray showed a well-defined radiolucency extending from the right angle of the mandible to the molar region, including the impacted wisdom tooth, and root resorption of the molars. Following antibiotic treatment to reduce inflammation, tooth extraction, biopsy, and fenestration were performed under general anesthesia. The histopathological diagnosis was radicular cyst. Fenestration treatment was continued, enucleation of the cyst and wisdom tooth extraction were conducted, with immediate mandibular reconstruction by iliac bone grafting. The right lower wisdom tooth was extracted, the cyst was enucleated, and an iliac bone block was grafted into the large defect in the right lower molar region of the mandible and fixed in place with a metal plate. The removed tissue was cystic. Computed tomography 18 months postoperatively showed mandibular bone formation, and the metal plate was removed under general anesthesia. Three years postoperatively, since the mandible had healed well, implants were inserted, and good occlusion was achieved.
Keywords: Iliac bone grafting, Implant treatment, Mandibular reconstruction, Odontogenic cyst
Introduction
Odontogenic cysts are comparatively common, but large odontogenic cysts that extend into the unilateral mandible are rare. Because enucleating the cyst leaves a defect in the mandible, mandibular reconstruction and occlusal reconstruction of the missing teeth must be taken into consideration when choosing a treatment method. We here present the case of a patient with a large odontogenic cyst extending to the unilateral mandible by enucleation and mandibular reconstruction with an iliac bone graft, followed by occlusal reconstruction by dental implant treatment.
Case Report
A 69-year-old man felt discomfort in his right mandible in May 2020, and in mid-June, he developed swelling and pain, so he presented to a local dental clinic. A panoramic X-ray showed radiolucency in the right lower molar region and impacted wisdom teeth, and he was referred to our department.
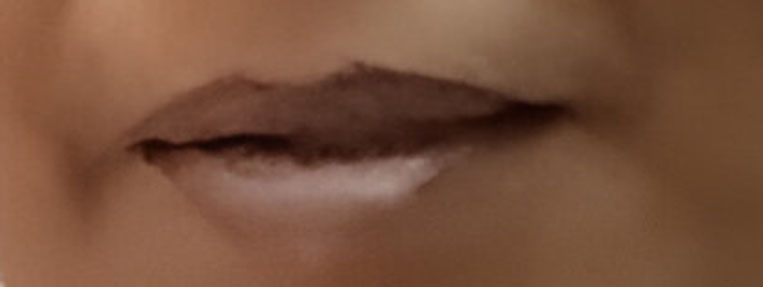
On presentation, facial examination showed pronounced swelling from below the right mandible to the neck, and mouth opening was impaired, at only 20 mm. Intraoral examination showed swelling and redness of the gingiva in the right lower molar region (Figure 1). There was no swelling of the tongue or of the floor of the mouth, but a purulent liquid discharge from the gingival sulcus was evident.
A panoramic X-ray showed a well-defined radiolucency extending from the right angle of the mandible to the molar region, including the impacted wisdom tooth, and root resorption of the molars (Figure 2). Computed tomography showed a well-defined hypodense area of 40 × 60 mm in the right angle of the mandible, as well as thinning of the cortical bone on the buccal and lingual sides (Figure 3A and Figure 3B). On magnetic resonance imaging (MRI), the contents were hyperintense on T2-weighted imaging (Figure 4A), and contrast-enhanced T1-weighted imaging showed a contrast-enhanced cystic lesion (Figure 4B).
Right cervical cellulitis was diagnosed, and the patient was admitted for treatment. Treatment was started with sulbactam/ampicillin 3g administered intravenously 4 times per day. The inflammatory symptoms improved, and the patient was discharged on Day 8.
In July 2020, extraction, biopsy, and fenestration were conducted under general anesthesia (Figure 5A and Figure 5B). Histopathological findings showed fibrous connective tissue with cholesterin crystal precipitation and clusters of histiocytes that had phagocytosed hemosiderin, and a cyst wall with stratified squamous epithelium and granulation tissue (Figure 6A and Figure 6B). The histopathological diagnosis was radicular cyst. With a diagnosis of odontogenic cyst of the mandible, fenestration treatment was continued, and since the size of the cystic lumen decreased (Figure 7). In March 2021, confirming that there are no inflammatory findings suspicious of infection, and enucleation of the cyst and wisdom tooth extraction were conducted under general anesthesia, and immediate mandibular reconstruction by iliac bone grafting was performed at the same time. During the procedure, the right lower wisdom tooth was extracted, the cyst was enucleated, and an iliac bone was grafted into the large defect in the right lower molar region of the mandible and fixed in place with a metal plate (Figure 8). The removed tissue was cystic (Figure 9).
The histopathological findings were the same as those of the tissue biopsy. Histologically, a cyst wall covered with nonkeratinized squamous epithelium was evident, and fibrosis, inflammatory cell infiltration mainly by lymphocytes and plasmacytes, congestion and bleeding, needle-shaped cholesterin crystals, and hemosiderin deposition were apparent within the cyst wall (Figure 10A and Figure 10B). Taken in conjunction with the clinical findings, an odontogenic cyst was diagnosed.
Computed tomography 18 months postoperatively showed mandibular bone formation (Figure 11), and in January 22, the metal plate used to fix the iliac bone graft in place was removed under general anesthesia.
In May 2023, three years postoperatively, since the mandible had healed well (Figure 12A and Figure 12B), implants were inserted, and the superstructures were fitted in September that year, successfully achieving good occlusion (Figure 13A, Figure 13B, Figure 13C, Figure 13D).













Discussion
Odontogenic cysts are encountered comparatively frequently in everyday clinical practice, but large odontogenic cysts that extend into the unilateral mandible are rare. The basic treatment strategy for odontogenic cysts are enucleation, but since the enucleation of a large odontogenic cyst leaves a large defect in the mandible, other methods include the use of fenestration to reduce the size of the cyst before enucleation [1],[2],[3], and filling of the defect with a bone graft in preparation for postoperative prosthetic treatment [4].
The advantage of fenestration is that, not only does it potentially reduce the size of the cyst, but a biopsy can also be performed at the same time. Tissue biopsy is particularly important when the differential diagnosis includes a tumor.
In the present case, since root resorption had occurred in the right lower molar region, and the lesion might have been tumor [5],[6], fenestration was performed because this enabled tissue biopsy while also potentially reducing the size of the cyst. Important considerations regarding fenestration include the fact that the cyst may take some time to contract, and there are limits to the decrease in size that can be achieved. It is therefore necessary to monitor the cyst by regular X-ray examinations or other means to determine whether it is decreasing in size, and to perform fenestration at the appropriate time after a certain amount of contraction has been achieved.
In the present case, the original cyst was 40 × 60 mm, which was large enough to extend into the unilateral mandible, its enucleation was expected to cause an extensive bone defect even after its size had been reduced by fenestration; therefore, mandibular reconstruction by iliac bone grafting was carried out. There are two main methods of iliac bone grafting after enucleation of an odontogenic cyst particulate cancellous bone and marrow (PCBM) grafting, and the use of a bone block together with PCBM. In PCBM grafting, undifferentiated mesenchymal cells in PCBM promote new bone formation, which is then followed by bone resorption and formation, inducing the reconstruction of the bone to match the surrounding graft bed [7],[8]. When iliac bone grafting with PCBM is to be performed, the space from which the cyst was enucleated should still be surrounded by cortical bone, although in patients where resorption has extended into the cortical bone, the PCBM may be covered with a titanium mesh tray. But these methods are limited in their application to extensive bone defects. Although the PCBM alone can be shaped by using a titanium mesh tray, it is prone to deformation immediately after surgery due to external forces, and the PCBM may show resorption of the grafted bone over time. However, the use of iliac block bone in combination with PCBM reduces the resorption of grafted bone compared to PCBM alone, so the method of grafting iliac block bone and reconstructing with a plate is reliable for extensive jaw bone defects.
Iliac bone-block grafting entails the harvesting of the patient’s own healthy bone, but postoperative synostosis is good, and it provides highly effective reconstruction. Because implant treatment for occlusal reconstruction was planned after mandibular reconstruction, to more accurately reproduce the original shape of the mandible, iliac bone-block grafting was performed and the grafted block was fixed in place with a metal plate to prevent resorption of the grafted bone. The area around the block was packed tightly with PCBM to provide better mandibular formation and enable secure implant placement. Histological observations over time following mandibular reconstruction with PCBM have shown that active new bone formation occurs 3–5 months after grafting, and that by six months postoperatively, it has almost been replaced by mature bone tissue [9],[10]. In the present case, the plate was removed 18 months postoperatively, and implant insertion was performed three years after grafting.
Reconstructive methods for mandibular defects to enable later implant treatment include autologous block bone grafting, artificial bone grafting, and vascularized fibula grafting. In autologous block bone grafting, veneer grafts or onlay grafts of cortical or cortical cancellous bone are mainly used, but it has the disadvantages of postgrafting bone resorption and the difficulty of reproducing the horizontal and vertical shape of the alveolar ridge [11]. Many types of artificial bone grafts exist, such as hydroxyapatite (HA), β-tricalcium phosphate (β-TCP), and carbonate apatite (CA), and the range of indications is expanding. However, it is often difficult when the defect site is large. Marx et al. [12],[13] stated that, when performing mandibular reconstruction, rather than simply achieving continuity of the bone, sufficient bone must be used to extend reconstruction to the alveolar ridge to establish occlusion in the reconstructed region. In addition to the complexity of the procedure, vascularized fibula grafting is difficult to achieve a morphology that approximates the original mandible. With recent advances in dental implant treatment, there is a growing demand for mandibular reconstruction to allow for implant placement. Vascularized fibula grafting has the disadvantages of difficulty in reproducing the complex folding of the mandible and low bone volume compared to the original mandible. Based on these considerations, we decided to use a block bone graft in addition to PCBM in this case. Important factors for achieving good results from mandibular reconstruction with PCBM include: (1) the choice of a donor site containing good-quality cells; (2) securing a sufficient amount of PCBM; (3) the PCBM is tightly packed; and (4) the choice of a graft bed that is not infected and with good blood flow. The ilium is considered to be the best source of PCBM meeting factors (1) and (2). In the present case, the mandible was reconstructed with an iliac bone-block graft that provided an alveolar ridge of sufficient height and width, and the bone quality was also good, enabling implants to be inserted.
Unlike normal mandibular bone, grafted bone has no cancellous bone component; therefore, when implants are inserted, the entire fixture must be inserted into the hard grafted bone, necessitating caution during the application of torque on insertion. In the present case, the hardness at the insertion site appeared to be that of cortical bone until the final drilling position, but the torque and rotation speed were comparable to those of regular insertion. The shape of the gingiva at the healing cap was also corrected after implant insertion, but gingival resection around the healing cap and healing cap replacement took some time because several procedures, including fenestration, had been performed at the site where the cyst had been, and the attached gingiva was thick.
Ultimately, good occlusion was achieved, and the soft tissue around the implants healed successfully. No abnormal bone resorption occurred around the implant body, and good esthetics and restoration of occlusal function were achieved.
Conclusion
A patient with a large odontogenic cyst extending into the unilateral mandible was treated successfully by enucleation, reconstruction of the mandible with an iliac bone, and occlusal reconstruction with dental implant treatment. Mandibular reconstruction by iliac bone-block grafting may be an effective preparation for occlusal reconstruction with dental implant treatment.
REFERENCES
1.
AboulHosn M, Noujeim Z, Nader N, Berberi A. Decompression and enucleation of a mandibular radicular cyst, followed by bone regeneration and implant-supported dental restoration. Case Rep Dent 2019;2019:9584235. [CrossRef]
[Pubmed]

2.
Tolstunov L. Marsupialization catheter. J Oral Maxillofac Surg 2008;66(5):1077–9. [CrossRef]
[Pubmed]
3.
Neaverth EJ, Burg HA. Decompression of large periapical cystic lesions. J Endod 1982;8(4):175–82. [CrossRef]
[Pubmed]
4.
Mauceri R, Murgia D, Cicero O, et al. Leucocyte- and platelet-rich fibrin block: Its use for the treatment of a large cyst with implant-based rehabilitation. Medicina (Kaunas) 2021;57(2):180. [CrossRef]
[Pubmed]
5.
White SC, Pharoah MJ. Chapter 20. Cysts of the jaws. In: Oral Radiology Principles and Interpretation. 5ed. Missouri: Mosby; 2004. p. 384–409.
6.
Larheim TA, Westesson PL. Chapter 2. Jaw Cysts, Maxillofacial Imaging. Berlin: Springer; 2006. p. 21–37.
7.
Axhausen W. The osteogenetic phases of regeneration of bone; a historial and experimental study. J Bone Joint Surg Am 1956;38-A(3):593–600.
[Pubmed]
8.
Burwell RG. Studies in transplantation of bone VII. The fresh composite of homograft-autograft of cancellous bone; An analysis of factors leading to osteogenesis in marrow-containing bone grafts. J Bone Joint Surg Br 1964;46:110–40.
[Pubmed]
9.
Iino M, Shimizu H. Alveolar ridge augmentation using autogenous iliac cancellous bone graft combined with micro-titanium augmentation mesh and subsequent dental implant insertion. Asian J Oral Maxillofac Surg 2000;12:187–94.
10.
Iino M, Ishii H, Sato J, Seto K. Histological evaluation of autogenous iliac particulate cancellous bone and marrow grafted to alveolar clefts—A preliminary report of five young adult cases. Cleft Palate Craniofac J 2000;37(1):55–60. [CrossRef]
[Pubmed]
11.
Lekholm U, Wannfors K, Isaksson S, Adielsson B. Oral implants in combination with bone grafts. A 3-year retrospective multicenter study using the Brånemark implant system. Int J Oral Maxillofac Surg 1999;28(3):181–7.
[Pubmed]
12.
Marx RE, Ames JR. The use of hyperbaric oxygen therapy in bony reconstruction of the irradiated and tissue-deficient patient. J Oral Maxillofac Surg 1982;40(7):412–20. [CrossRef]
[Pubmed]
13.
Marx RE. Mandibular reconstruction. J Oral Maxillofac Surg 1993;51(5):466–79. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Hikaru Takahashi - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Yuichiro Takaku - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2025 Hikaru Takahashi et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}