 |
Case Series
Lumbar spine facet joint septic arthritis: Two case reports
1 MD, Specialist Radiology, Sohar Hospital, Sohar, Oman
2 MD, Consultant Radiology, Sohar Hospital, Sohar, Oman
3 MD, Radiology OMSB resident, MOH, Muscat, Oman
4 MD, Medical officer, National University, MOH, Muscat, Oman
Address correspondence to:
Maimouna S Al-Risi
MD, Specialist Radiology, Sohar Hospital, North Al Batinah,
Oman
Message to Corresponding Author
Article ID: 101489Z01MA2025
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Al-Risi MS, Selim YAR, Al Isaii AA, Almatroushi NA. Lumbar spine facet joint septic arthritis: Two case reports. Int J Case Rep Images 2025;16(1):5–10.ABSTRACT
Introduction: Septic arthritis of the facet joint (SAFJ) is a rare spine condition. Commonly seen in older immune-compromised patients presented with acute back pain, it needs early diagnosis and intervention.
Case Series: We report two cases presented to the emergency as acute onset low back pain with fever and high inflammatory markers. In both cases, patients were admitted and diagnosed with septic arthritis of the facet joint and associated epidural abscess. In the first case, blood cultures were sent to support the diagnosis, while in the second case ultrasound-guided aspiration was done. In both cases, cultures were positive for Methicillin-resistant Staphylococcus aureus (MRSA) and diagnosis confirmed with magnetic resonance imaging (MRI) findings. Both patients were treated with intravenous antibiotics and improved clinically.
Conclusion: This case shows the importance of thinking about septic arthritis in the facet joint in older patients who present with sudden onset back pain associated with high inflammatory markers if other differentials are excluded. Magnetic resonance imaging is considered the imaging modality of choice in the diagnosis. As well, early diagnosis and management play an important role to prevent complications.
Keywords: Facet joint, MRI, Septic arthritis
Introduction
Septic arthritis of the facet joint (SAFJ) is historically a rare spinal condition. However, reported cases are increasing due to increasing median age, the increase in immune-compromised individuals for various reasons, and the increase in MRI utility [1]. It usually affects older immunocompromised patients although there are reported cases of young immunocompetent patients [2],[3]. Predisposing factors include diabetes mellitus, direct inoculation such as acupuncture, facet joint injection, epidural catheters, and spinal surgery. Hematogenous spread is the most common reported cause of SAFJ. In reviewing literature, the lumbar spine is involved in most cases [3]. The most common identified organism causing facet joint septic arthritis is Staphylococcus aureus. Magnetic resonance imaging (MRI) is the investigation of choice for lumbar spine as it is highly sensitive in diagnosing septic arthritis and demonstrating the extent of infection and its complications like epidural and paraspinal abscesses [4]. Patients with septic arthritis of the facet joint present atypically as acute back pain or acute abdomen. Since lower back pain is rarely caused by septic arthritis of the lumbar facet joint, it is important to establish the diagnosis at an early stage to start intravenous antibiotics therapy and prevent possible complications [4]. Early diagnosis of SAFJ followed by definitive therapy requires a multidisciplinary team approach.
CASE SERIES
Case 1
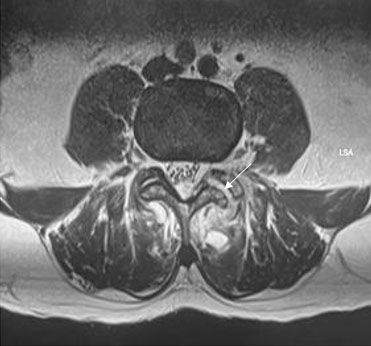
A 55-year-old male, not known to have any medical background, was admitted in secondary hospital with history of sudden onset of lower back pain, which is more in the left side, radiating to bilateral lower limbs and aggravated by movement. Back pain followed by onset of high-grade fever and malaise. No history of trauma, respiratory symptoms, neurological deficit, or urinary symptoms. Physical examination was significant for left lumbar tenderness, positive straight leg raise test (SLR), and temperature of 38°C. Laboratory tests showed C-reactive protein (CRP) of 246 mg/L, white blood count (WBC) was (7.5×109/L), and plasma glucose level was 14 mmol/L. In further investigation during admission glycated hemoglobin (HbA1C) came as 8%. Lumbosacral X-ray was not significant. Computed tomography (CT) abdomen-pelvis with intravenous (IV) contrast was done and it was normal apart from mild spondylo-degenerative changes. Blood culture came positive for Methicillin-resistant Staphylococcus aureus (MRSA). Furthermore, MRI with and without gadolinium contrast was requested and showed widening of the left facet joint at L3/L4 level with moderate effusion, eroded articular surface, and joint effusion (Figure 1). The L4 left lamina showed edematous bone marrow with thickened related intraspinal left posterolateral epidural soft tissue forming 10 mm thickness phlegmon which extend into left neural foramen and inferiorly up to L5/S1 level (Figure 2). The adjacent paraspinal muscle showed phlegmon with increased signal intensity in T2 Short Tau Inversion Recovery (STIR) (Figure 3). There was increased enhancement at T1 post-contrast images at the level of the articular surface of L3/L4, adjacent paraspinal soft tissue with evidence of bone marrow edema of the lamina (Figure 4).
These radiological features consistent with septic arthritis of left L3/L4 facet joint and osteomyelitis of left hemi-neural bony arch of L3, posterior epidural with mild neural compression, and localized paraspinal myositis with small abscess formation. As the patient did not have neurological deficit, no surgical treatment was indicated. The patient’s treatment with appropriate antimicrobial therapy was successful. Transesophageal echocardiogram was done and there was no evidence of vegetation. During admission he was diagnosed with type 2 diabetes mellitus.
Case 2
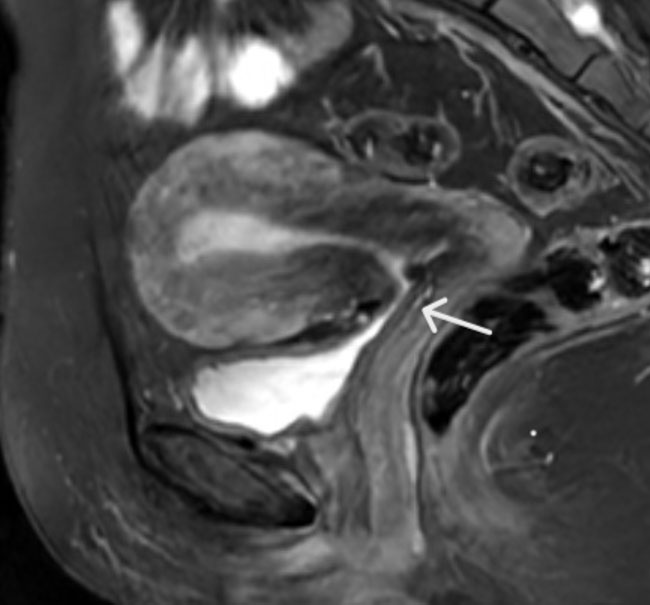
A 48-year-old male, known case of hypertension, type 2 diabetes mellitus and dyslipidemia (not compliant to treatment), with previous history of cerebellar infarction. This patient presented with complaints of sudden onset low back pain for two weeks, radiating to the right gluteal region and lower limbs, pain increase with movement, associated with bilateral lower limb numbness, on and off fever, dyspnea and palpitations. He started using non-steroidal anti-inflammatory drugs (NSAIDs) for pain relief, he noted heartburn and black colored stool, no associated nausea, vomiting or abdominal pain. No history of recent trauma, neurological deficit, or urinary symptoms were found. During the examination, the patient looked sick and pale, afebrile, with a blood pressure of (BP) 160/95 mmHg, a heart rate (HR) of 100 bpm, and saturation maintained on room air. He had significant tenderness at the right sacroiliac joint region with positive SLR test in both lower limbs. Other examinations were unremarkable. Laboratory investigation showed elevated CRP of 170 mg/dL with WBC of 13×109/L. Labs showed low hemoglobin of (5.9 g/dL). Renal function was deranged, with estimated glomerular filtration rate (eGFR) of 64 mL/min/1.73 m2 and creatinine 112 μmol/L. Lumbosacral X-ray was not significant. Lumbosacral MRI with and without gadolinium contrast done and showed widening of the right facet joint at L4/L5 level with moderate effusion. The L4 right lamina showed edematous bone marrow with thickened soft tissue forming phlegmon that extended into the right neural foramen and superiorly to L3/L4 level to form marginally enhanced abscess (Figure 5). Post-contrast, there was diffuse enhancement of the affected muscles, with evidence of cellulitis at the posterior subcutaneous soft tissue and abscess formation on the right side at L4/L5 level (Figure 6A and Figure 6B). These radiological features were consistent with septic arthritis of the right facet joint at L4/L5 level, with osteomyelitis of the right hemi-neural bony arch of L4, associated posterior enhanced phlegmon and small epidural abscess at L3/L4. There is right paraspinal myositis with multiple large multilocular abscess formation from L2 to L5 level. This patient underwent ultrasound-guided aspiration until dryness, sample sent for culture and came positive for MRSA. The patient managed with appropriate antimicrobial therapy successfully.





Discussion
Septic arthritis of the facet joint is considered a rare spinal condition with atypical challenging presentations. It can occur by hematogenous spread or by direct inoculation following spinal procedures [5],[6]. In reviewing literature, a retrospective review of reported cases concluded that SAFJ accounts for (4–20%) of cases of spinal infections. The average age of patients was (55–59) years old, and the lumbar spine was the most affected part. In a case series involved 42 patients with spontaneous facet joint septic arthritis the lumbosacral region was affected in 86% of cases. In addition, L4–L5 spinal level was involved in 40% of cases, followed by the L3–L4 level in 17% of cases [3],[7]. In our cases, the first case reported 54 years old while the second was 48 years and in both cases L3–L4 level is affected. Most reported cases in literature are caused by hematogenous spread of primary infection; however, there are multiple reported cases resulting from iatrogenic causes such as epidural catheterization or steroid injections. The pathogenesis of septic arthritis of facet joints is not clear. Degenerative changes in the facet joint may increase the risk for pyogenic arthritis [3]. Complications of septic arthritis of facet joints include epidural abscess and variant degrees of neurological deficits [8]. Facet joint articular cavity is narrow; thus, the infection can spread to the epidural region easily. The infection can spread to the paraspinal region if the abscess breaks into the dorsal aspect of the articular capsule [9]. Clinically, severe back pain is the most common presentation for patients with facet joint septic arthritis. Fever is the most common reported associated symptom [3]. Our patients presented with sudden onset severe back pain radiating to lower limbs without neurological deficit. In laboratory testing, CRP and erythrocyte sedimentation rate (ESR) were elevated in the majority of reported cases. The most common identified bacterial organism by blood cultures is Staphylococcus aureus (81%) [3]. In addition, Streptococcus and gram-negative rods are reported in some cases. In our cases, MRSA was isolated. Early radiological evaluation is necessary to diagnose facet joint septic arthritis. Plain radiographs may show features of erosive arthritis but not in the early stage of the disease. Computed tomography may be normal in the early disease course and may show nonspecific degenerative changes. On the other hand, MRI with gadolinium contrast is the imaging modality of choice and can be used as early as two days following the onset of symptoms. It shows inflammatory changes of the joint which cause narrowing of joint cavity and erosion of the intervertebral space. Also, it illustrates extra-vertebral extension of infection in epidural, paraspinal, and psoas areas. The overall prognosis of SAFJ is good. Treatment of this condition includes surgical treatment, but in most uncomplicated cases conservative treatment with antibiotics is sufficient.
Conclusion
This case series is considered challenging in which the patients present with atypical symptoms, and the diagnosis made after other differentials were excluded. Both patients presented with low back pain and fever. Further investigations done, laboratory tests show high inflammatory markers. In addition, MRI was done to confirm the diagnosis and reported as septic arthritis of the facet joint with associated epidural abscess involving L3/L4 in both cases. Eventually, both patients managed with antimicrobial therapy successfully with significant improvement.
REFERENCES
1.
Maldonado-Morán M, Muñoz JM, Matta JI, Arrieta VM, Bernal OP, Mejía JM. A rare case of septic arthritis of lumbar facet joint with epidural abscess, and bacterial meningitis caused by methicillin-sensitive Staphylococcus aureus. Indian J Neurosurg 2018;7(2):139–41. [CrossRef]

2.
Mas-Atance J, Gil-García MI, Jover-Sáenz A, et al. Septic arthritis of a posterior lumbar facet joint in an infant: A case report. Spine (Phila Pa 1976) 2009;34(13):E465–8. [CrossRef]
[Pubmed]
3.
Setoue T, Nakamura JI. A rare case of thoracic pyogenic facet joint infection. Case Rep Orthop 2019;2019:8252986. [CrossRef]
[Pubmed]
4.
Dhodapkar MM, Patel T, Rubio DR. Imaging in spinal infections: Current status and future directions. N Am Spine Soc J 2023;16:100275. [CrossRef]
[Pubmed]
5.
Doita M, Nabeshima Y, Nishida K, Fujioka H, Kurosaka M. Septic arthritis of lumbar facet joints without predisposing infection. J Spinal Disord Tech 2007;20(4):290–5. [CrossRef]
[Pubmed]
6.
Rajeev A, Choudhry N, Shaikh M, Newby M. Lumbar facet joint septic arthritis presenting atypically as acute abdomen – A case report and review of the literature. Int J Surg Case Rep 2016;25:243–5. [CrossRef]
[Pubmed]
7.
Narváez J, Nolla JM, Narváez JA, et al. Spontaneous pyogenic facet joint infection. Semin Arthritis Rheum 2006;35(5):272–83. [CrossRef]
[Pubmed]
8.
Muffoletto AJ, Ketonen LM, Mader JT, Crow WN, Hadjipavlou AG. Hematogenous pyogenic facet joint infection. Spine (Phila Pa 1976) 2001;26(14):1570–6. [CrossRef]
[Pubmed]
9.
Marson F, Cognard C, Guillem P, Sévely A, Manelfe C. Septic arthritis of a lumbar facet joint associated with epidural and paravertebral soft tissue abscess [Article in French]. J Radiol 2001;82(1):63–6.
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Maimouna S Al-Risi - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Yasser AR Selim - Conception of the work, Design of the work, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Arwa A Al Isaii - Acquisition of data, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Noura A A lmatroushi - Acquisition of data, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2025 Maimouna S Al-Risi et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}