 |
Case Report
Dyke–Davidoff–Masson syndrome: A typical case of late diagnosis
1 Resident in Radiology, Department of Neuroradiology, Specialty Hospital, UHC Ibn Sina Mohamed V University, Rabat, Morocco
2 Medicine, Resident in Radiology, Department of Neuroradiology, Specialty Hospital, UHC Ibn Sina Mohamed V University, Rabat, Morocco
3 Department of Neuroradiology, Specialty Hospital, UHC Ibn Sina Mohamed V University, Rabat, Morocco
Address correspondence to:
Eric Michel Charlemagne Junior Kessi
Resident in Radiology, Department of Neuroradiology, Specialty Hospital, UHC Ibn Sina Mohamed V University, Rabat
Morocco
Message to Corresponding Author
Article ID: 101456Z01EK2024
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Junior Kessi EMC, El Amrani S, Dghoughi B, Touarsa F, Fikri M, Jiddane M, El Kettani EC. Dyke–Davidoff– Masson syndrome: A typical case of late diagnosis. Int J Case Rep Images 2024;15(1):103–106.ABSTRACT
Dyke–Davidoff–Masson syndrome, a rare clinico-radiological neurological entity generally observed in childhood, is classically characterized by epileptic seizures, facial asymmetry, contralateral hemiplegia or hemiparesis, convulsions, mental retardation, skull, and frontal sinus anomalies. It is poorly recognized and generally mistaken for ischemic lesions. We report the clinical and radiological data of a 39-year-old patient with a left-hemisphere deficit since childhood and mention of absence seizures.
Keywords: Bone hypertrophy, Cerebral hemiatrophy, Dyke–Davidoff–Masson syndrome
Introduction
Dyke–Davidoff–Masson syndrome (DDMS) or cerebral hemiatrophy is a rare disease, which can be either congenital or acquired, occurring as a result of altered cerebral perfusion during the prenatal, perinatal, or early childhood period [1],[2]. It affects both sexes, with a predominance in the male population (73.5%), and left-hemisphere involvement is the most common [3]. It manifests as hemiparesis, seizures, intellectual or learning disabilities, Psychiatric and language disorders. Diagnosis is usually made in late childhood, but can sometimes be a later discovery [4]. Imaging shows cerebral hemiatrophy and compensatory bone hypertrophy [5].
Case Report
The patient was a 39-year-old man who, since childhood, presented with a left-hemisphere deficit associated with a slight delay in psychomotor development and gait irregularity. For five years, absence seizures and cognitive disorders had appeared for which he had been put on anticonvulsant treatment and obtained a partial improvement. These disorders were sometimes accompanied by generalized tonic-clonic seizures; all without any radiological exploration. Our patient was born out of a non-consanguineous marriage. Birth history was indicative of a full-term normal delivery without any antenatal or perinatal complications.
On physical examination, facial asymmetry was observed, including an asymmetrical prominence of the frontal bone and left hemiparesis. We note a stiffness of the left extremities. Examination of the cranial nerves was unremarkable.
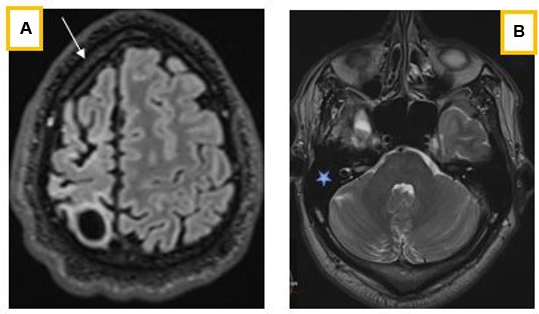
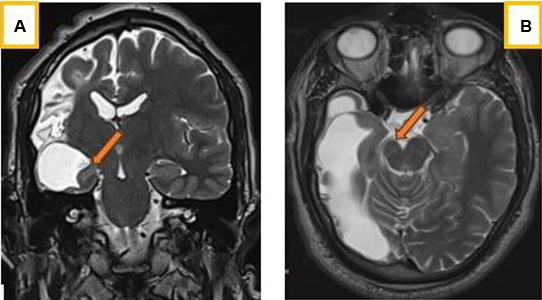
Radiologically, the cerebral hemispheres were asymmetrical, with reduced volume of the right hemisphere (Figure 1 and Figure 2), which was the site of a leukomalacia lesion with compensatory enlargement of the homolateral lateral ventricle (Figure 2). There was also widening of the homolateral cortical sulci, which was more marked opposite the leukomalacia focus, hyperpneumatization of the frontal sinuses (Figure 1) and calvarial thickening, predominantly on the lesion side (Figure 3A), but also of the mastoid cells, which had a compensatory appearance (Figure 3B). It was associated with discrete atrophy of the right cerebral peduncle (Figure 4A) and a reduction in homolateral hippocampal volume (Figure 4B).
In view of these clinical and radiological signs, the diagnosis of Dyke–Davidoff–Masson syndrome was evoked.


Discussion
Dyke–Davidoff–Masson syndrome (DDMS) was first described in 1933 as cerebral hemiatrophy or hypoplasia with ipsilateral enlargement of the skull and sinuses in a series of nine patients with hemiplegia and presenting with changes in simple skull X-ray (Dyke et al., 1933) [1],[6]. It is secondary to cerebral attack and usually occurs during the fetal period or early childhood [7]. Vascular attacks occur most frequently. However, the natural course of this disease in adults has not been described in detail due to the rarity of cases, and the pathogenesis of this syndrome remains debated. Some authors have suggested a link with in utero or postnatal brain damage. These lesions may be related to congenital malformation, infection, vascular injury, birth trauma, anoxia, hypoxia, or intracranial hemorrhage during the perinatal period [6],[7]. The cause of symptoms is usually congenital, and the underlying etiological factor is unknown when symptoms appear in young age or during pregnancy [8]. Due to its rarity, this syndrome is often underdiagnosed by the untrained eye despite its many clinical manifestations. Symptoms mainly include facial asymmetry, hemiparesis or hemiplegia, seizures, cognitive and psychiatric symptoms, all of which depend on the extent of the lesions [6],[7],[9]. Convulsions do not always appear in early childhood and can occur years after hemiparesis, and may be focal or generalized [5]. Psychiatric disorders can be observed and are consecutive to the loss of cerebral volume, the dilation of the lateral ventricle and the striatum. Unilateral focal atrophy may also be observed in the cerebral peduncles and the thalamic, cerebellar, pons, and para-hippocampal regions [3]. Patients with unilateral right brain injury may present euphoric and depressive states after unilateral left injury [7].
Computed tomography (CT) imaging, especially magnetic resonance imaging (MRI), is therefore essential for accurate diagnosis, assessment of severity and appropriate management [9],[10]. It classically describes cerebral hemiatrophy, usually accompanied by ipsilateral compensatory bone hypertrophy, such as thickening of the ipsilateral calvaria, hyperpneumatization of the frontal sinuses and mastoid cells, and elevation of the orbital roof and petrous ridge and contralateral hemiparesis [7],[11]. This asymmetry in the prominent development of the frontal sinus may be accompanied by an increase in the thickness of the diploe of the frontal bone on this side. It may be associated with mesencephalic and/or hippocampal atrophy [8], as was the case in our patient.
Differential diagnoses include Sturge–Weber syndrome, Rasmussen encephalitis, Fishman syndrome, and Silver–Russell syndrome.
Sturge–Weber syndrome is characterized by classic facial cutaneous vascular malformations, seizures, mental retardation, and intracranial vascular anomalies. There is no ipsilateral hyperpneumatization of the frontal sinus [8],[11].
Rasmussen’s encephalitis is a chronic progressive immune-mediated disease affecting children aged 6–8 years, characterized by episodes of refractory epilepsy with hemiparesis; imaging shows cortical hemiatrophy; there is also no hyperpneumatization of the frontal sinus [3].
Fishman’s syndrome or encephalo-cranio-cutaneous lipomatosis is a congenital neuro-cutaneous syndrome comprising a unilateral cranial lipoma and a lipodermoid of the eye usually presenting with epileptic seizures; imaging shows dilatation of lateral ventricle, porencephalic cavity, calcified cortex and hemiatrophy; no ipsilateral hyperpneumatization of frontal sinus [3],[8].
Silver–Russell syndrome is manifested by growth retardation, calvarial hypertrophy with a pseudohydrocephalic appearance, intelligence is preserved; there is no sinus hyperpneumatization or bone hypertrophy [11].
Patients with intrauterine or perinatal lesions appear to have more frequent calvarial enlargement and hyperpneumatization [1]. Early identification and treatment are important for these patients, as they can improve their prognosis and quality of life.
Conclusion
Dyke–Davidoff–Masson syndrome is rare and can sometimes be underdiagnosed as an ischemic lesion in the presence of a motor deficit. It should be considered in any patient presenting with classic neurological features and brain imaging showing cerebral hemiatrophy associated with bone hypertrophy, in order to ensure correct diagnosis and appropriate management. The prognosis is better when hemiparesis appears after the age of two years and in the absence of recurrent and prolonged epilepsy.
REFERENCES
1.
Duncan M, Vázquez-Flores S, Chávez-Lluévanos EB, Cantú-Salinas AC, León-Flores LD, Villarreal-Velázquez HJ. Dyke-Davidoff-Masson syndrome: A case study. Medicina Universitaria 2014;16(63):71–3.

2.
El Bahri-Ben Mrad F, Mrabet H, Ben Sghaier R, Mrabet A. Dyke-Davidoff-Masson syndrome: A report of two cases. [Article in French]. J Neuroradiol 2005;32(1):50–3. [CrossRef]
[Pubmed]
3.
Ayele BA, Zewde YZ. Dyke-Davidoff-Masson syndrome – A rare cause of cerebral hemiatrophy in a 17-years-old Ethiopian patient: A case report. Ethiop J Health Sci 2019;29(2):287–90. [CrossRef]
[Pubmed]
4.
Behera MR, Patnaik S, Mohanty AK. Dyke-Davidoff-Masson syndrome. J Neurosci Rural Pract 2012;3(3):411–3. [CrossRef]
[Pubmed]
5.
Lina B, Zaynab EH, Amina K, et al. Dyke Davidoff Masson syndrome: Typical aspect. Int J Clin Med Imaging 2022;9:845.
6.
Stoevesandt D, Stock K, Spielmann RP, Heine HJ, Paulsen F, Bräuer L. Postmortal diagnosis of a Dyke-Davidoff-Masson syndrome in a 75-year-old woman—A case report. Ann Anat 2009;191(2):225–7. [CrossRef]
[Pubmed]
7.
Hamza N, Hdiji O, Haj Kacem H, et al. Dyke Davidoff Masson syndrome a rare cause of schizoaffective disorder: A case report and review of the literature. Encephale 2019;45(3):274–5. [CrossRef]
[Pubmed]
8.
Duarte ACB, Camporeze B, Buainain RP. Dyke-Davidoff-Masson syndrome: An unusual case of late diagnosis. Neurol Sci 2018;39(9):1603–5. [CrossRef]
[Pubmed]
9.
Sarikaya B, Sarikaya S. Dyke-Davidoff-Masson syndrome revisited: A didactic case with interesting imaging findings. Australas Radiol 2007;51 Spec No.:B10–3. [CrossRef]
[Pubmed]
10.
Abdul Rashid AM, Md Noh MSF. Dyke-Davidoff-Masson syndrome: A case report. BMC Neurol 2018;18(1):76. [CrossRef]
[Pubmed]
11.
Roy U, Panwar A, Mukherjee A, Biswas D. Adult presentation of Dyke-Davidoff-Masson syndrome: A Case Report. Case Rep Neurol 2016;8(1):20–6.
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Eric Michel Charlemagne Junior Kessi - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Soukaina El Amrani - Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Basma Dghoughi - Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Firdaous Touarsa - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Meriem Fikri - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Mohamed Jiddane - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Ech-Cherif El Kettani - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2024 Eric Michel Charlemagne Junior Kessi et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}