 |
Case Report
A case of inguinal hernia with partial bladder herniation
1 MD, Resident Physician, Department of Surgery, Central Michigan University, Saginaw, MI, United States
2 Medical Student, Department of Surgery, Central Michigan University, Saginaw, MI, United States
3 MD, Assistant Professor of Surgery, Department of Surgery, Central Michigan University, Saginaw, MI, United States
Address correspondence to:
Nzi Jacques Philippe Niamien
MD, 4616 Colonial Dr, apt 2, Saginaw, MI 48603,
United States
Message to Corresponding Author
Article ID: 101448Z01NF2024
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Farooqi N, Macek S, Niamien NJP, Ireland N, Yoon Y. A case of inguinal hernia with partial bladder herniation. Int J Case Rep Images 2024;15(1):69–72.ABSTRACT
Introduction: Inguinal hernia repairs are commonly performed, and recurrence remains one of the well-known complications. In rare cases, intra-abdominal organs can become entrapped in the hernia sac, risking incarceration and subsequent strangulation if not managed promptly.
Case Report: A 78-year-old male previously underwent bilateral inguinal hernia repair presented to the hospital with acute onset abdominal distension with associated nausea and emesis. He had noticed a progressively enlarging bulge in his left groin with fluctuating abdominal pain. Prior to his presentation, he had been struggling with incomplete voiding and frequent micturition managed unsuccessfully with tamsulosin. On examination, the patient’s abdomen was soft and non-tender, but visibly distended with a large incarcerated recurrent left inguinal hernia. The patient was admitted and subsequently underwent computed tomography (CT) abdomen and pelvis examination, which demonstrated mild distension of small bowel loops and an inguinal hernia with an encased segment of urinary bladder. The patient was managed conservatively and scheduled for an outpatient open hernia repair. Intraoperatively, multiple hernia sacs comprised of bladder were visualized extending into the suprapubic region. Each hernia sac was carefully opened and reduced without damage to the urinary bladder. Postoperatively, he recovered without complications and had complete symptom resolution.
Conclusion: This case illustrates a rare complication of a common procedure that holds significant morbidity if not managed promptly. Identification of urinary bladder involvement is essential to reduce the risk of iatrogenic bladder damage during surgical repair of an inguinal hernia and to ensure complete symptom resolution for the patient.
Keywords: Bladder, Hernia, Inguinal, Urinary
Introduction
The true incidence of abdominal wall hernias is difficult to estimate, however, it has been approximated to be around 5%. Inguinal hernias are around 75% of this proportion [1]. Inguinal hernia repair is one of the most common procedures performed in the world with around 20 million performed annually [2]. A sliding inguinal hernia occurs when a portion of the hernia sac is made by an intra-abdominal organ [3]. Sliding hernias comprising urinary bladder make around 1% of all sliding hernias [4]. Prolonged herniation can risk incarceration and subsequent strangulation of the urinary bladder. Moreover, it can also lead to urinary symptoms, such as incomplete voiding along with the pain and discomfort. We present a case of symptomatic incarcerated inguinal hernia with the sac comprising urinary bladder.
Case Report
A 78-year-old male with previous history of bilateral inguinal hernia repair presented to the hospital with acute onset of abdominal distension associated with nausea and emesis and recent recurrence of his left inguinal hernia. The bulge had been increasing in size with occasional pain but no discomfort. He additionally reported a feeling of incomplete voiding and frequent micturition. He had recently started taking tamsulosin, however, his symptoms were not entirely resolved with use of this medication.
His past surgical history was significant for bilateral hernia repair many years ago. The patient could not remember if there was a mesh used for these repairs.
His past medical history was significant for chronic kidney disease (CKD), asthma, and hypertension. He was a former smoker having quit more than 20 years ago.
Objectively, his vitals were within normal limits. His body mass index (BMI) was 29.95 kg/m2. His cardiac and respiratory exams were within normal limits. His abdomen was soft and non-tender but distended. There was a large incarcerated recurrent left inguinal hernia. The remainder of his exam was unremarkable.
On admission, his white blood cell count was 8 × 109/L, hemoglobin 14.8 g/dL, platelet count 156/µL. His creatine was 1.2 mg/dL which was his baseline and lactate was 2.1 mmol/L.
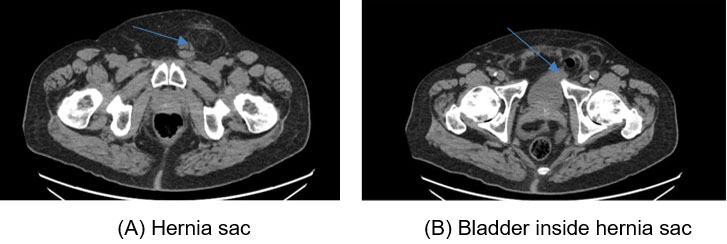
His CT scan demonstrated mild distension of small bowel loops suggesting small bowel obstruction from adhesive disease. He was also found to have a left inguinal hernia with a segment of the urinary bladder in the hernia sac (Figure 1 and Figure 2).
He was initially managed conservatively for small bowel obstruction with fluid resuscitation and nasogastric tube decompression. Gastrografin challenge was performed with evidence of contrast in the colon on abdominal series. The patient had evidence of return of bowel function. The patient preferred to be discharged home and follow-up for elective repair of his left recurrent hernia.
After discussion with the patient regarding his risk factors and high risk of injuries due to history of bilateral herniorrhaphy, we proceeded with an open repair of the left inguinal hernia. Intraoperatively, we noted significant scar tissue from previous repair. He had a large recurrent direct hernia and multiple small, incarcerated hernias extending into the suprapubic region. After dissection, it was all found to be a common hernia sac with bladder component found medially. The hernia sac was carefully opened and reduced without injury to the urinary bladder. There was no evidence of hematuria in the urinary catheter collecting bag. The conjoined tendon was sutured to the shelving edge of the inguinal ligament. A Prolene based mesh was placed over the suture line in accordance with the Lichtenstein technique. Postoperatively, he recovered without complications and was discharged home.
On postoperative follow-up, it was noted that he recovered well from the surgery. His urinary symptoms had resolved.

Discussion
Inguinal hernias are relatively common with a lifetime risk of 27% in men and 3% in women [5]. As discussed earlier, bladder herniation forms a very small percentage of all sliding hernias, and it is more common among men aged 30–70 [6]. As discussed by Bendavid, sliding hernias are of 3 types; type I refers to the hernia sac consisting of a part of the viscus, type II refers to the sac containing the mesentery of the retroperitoneal organ, and type III refers to the sac containing the entire viscus with or without the peritoneal sac [7].
Sliding bladder hernias can be symptomatic depending on their size and chronicity. Small bladder hernias can be asymptomatic and incidentally found on inguinal hernia repair. Large bladder hernias can present with urinary tract symptoms of dysuria, nocturia, hematuria, and 2 stage micturition. The first stage involves spontaneous voiding followed by manual compression of the hernia sac for evacuation [8].
Factors predisposing to developing sliding bladder hernias include old age, obesity, and loss of bladder tone with weakness of pelvic muscular structures with increasing age [9].
Our patient was in his 70s predisposing him to development of the hernia. Moreover, previous history of inguinal hernia suggests weak abdominal wall musculature.
A high index of suspicion for bladder herniation should be maintained in patient with an inguinal hernia associated with urinary symptoms. Diagnostic studies such as CT as well as cystography can be used for diagnosis in patients with high suspicion. Computed tomography also helps with evaluation for hydronephrosis secondary to urinary retention and bladder outlet obstruction [10].
There have been reports of patients presenting with bilateral sliding inguinal hernias with bladder component. Nasser et al. have reported a similar case in the literature. They managed the patient surgically with bilateral open Lichtenstein tension free repair with a successful outcome [11].
There have been reports of successful surgical management of the sliding inguinovesical hernia using open, laparoscopic, and robotic approaches.
Branchu et al. have reported in their systematic review that open repair is the most common technique adopted for repair [10]. Kim et al. have described a successful Lichtenstein repair in a 64-year-old patient with an inguinovesical hernia [12].
Kawaguchi et al. have reported successful treatment of right inguinovesical hernia laparoscopically [13]. There has been reports of successful treatment with the robotic approach as well [14].
The choice of procedure depends on the expertise of the surgeon and appropriate risk stratification of the patient to ensure a safe procedure.
Conclusion
Sliding bladder hernia is rare but can present a significant source of morbidity for the patient if not identified promptly. Surgical management is curative. Whether an open, laparoscopic, or robotic approach is chosen for repair depends on the patient’s unique characteristics and available surgical expertise.
REFERENCES
1.
Malangoni MA, Rosen MJ. Hernias. In: Courtney M, Townsend JR, Beauchamp RD, Evers BM, Mattox K, editors. Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice. 20ed. Philadelphia, Pennsylvania: Elsevier; 2017. p. 1092–3.

2.
Kingsnorth A. Treating inguinal hernias. BMJ 2004;328(7431):59–60. [CrossRef]
[Pubmed]
3.
Gaspar MR, Joergenson EJ, Woolley MM. Sliding indirect inguinal hernia. Calif Med 1956;85(5):330–4.
[Pubmed]
4.
Shepherd FJ. XIII. Hernia of the bladder complicating inguinal hernia. Ann Surg 1904;40(6):921–8. [CrossRef]
[Pubmed]
5.
Primatesta P, Goldacre MJ. Inguinal hernia repair: Incidence of elective and emergency surgery, readmission and mortality. Int J Epidemiol 1996;25(4):835–9. [CrossRef]
[Pubmed]
6.
Conde Sánchez JM, Espinosa Olmedo J, Salazar Murillo R, et al. Giant inguino-scrotal hernia of the bladder. Clinical case and review of the literature. Actas Urol Esp 2001;25(4):315–9. [CrossRef]
[Pubmed]
7.
Bendavid R. Sliding hernias. Hernia 2002;6(3):137–40. [CrossRef]
[Pubmed]
8.
Zihni I, Duran A, Soysal V. A rare cause of inguinal hernia: Scrotal cystocele. Ulus Cerrahi Derg 2014;32(2):137–9. [CrossRef]
[Pubmed]
9.
Huang TY, Shields RE, Huang JT, Postel GC, Abaskaron MA. Scrotal herniation of the bladder secondary to prostate enlargement. J Urol 1999;162(2):488–9.
[Pubmed]
10.
Branchu B, Renard Y, Larre S, Leon P. Diagnosis and treatment of inguinal hernia of the bladder: A systematic review of the past 10 years. Turk J Urol 2018;44(5):384–8. [CrossRef]
[Pubmed]
11.
AlMohaya N, Alabdrabalameer MNE, AlAnazi K, AlMuhsin AM, Eltomy H. Bilateral inguinal bladder hernia following unilateral transabdominal preperitoneal repair. A case report and review of the literature. Ann Med Surg (Lond) 2019;46:23–6. [CrossRef]
[Pubmed]
12.
Kim KH, Kim MU, Jeong WJ, et al. Incidentally detected inguinoscrotal bladder hernia. Korean J Urol 2011;52(1):71–3. [CrossRef]
[Pubmed]
13.
Kawaguchi T, Itoh T, Yoshii K, Otsuji E. Laparoscopic repair of a bilateral internal inguinal hernia with supravesical hernia – A case report. Int J Surg Case Rep 2015;14:108–11.
[Pubmed]
14.
Cetrulo LN, Harmon J, Ortiz J, Canter D, Joshi ART. Case report of a robotic-assisted laparoscopic repair of a giant incarcerated recurrent inguinal hernia containing bladder and ureters. Int J Med Robot 2015;11(1):15–7. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Najiha Farooqi - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Sarah Macek - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Nzi Jacques Philippe Niamien - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Nicole Ireland - Conception of the work, Design of the work, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Yong Yoon - Conception of the work, Design of the work, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2024 Nahija Farooqi et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}