 |
Case Report
An unusual presentation of small bowel volvulus: A case report
1 Department of Surgery, Faculty of Medicine, Umm Al-Qura University, Makkah, Saudi Arabia
Address correspondence to:
Ghassan Almaimani
Assistant Professor, Department of Surgery, Faculty of Medicine, Umm Al-Qura University, Al Abdeyah, PO Box 7607, Makkah,
Saudi Arabia
Message to Corresponding Author
Article ID: 101438Z01AR2024
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Almaimani G. An unusual presentation of small bowel volvulus: A case report. Int J Case Rep Images 2024;15(1):22–26.ABSTRACT
Introduction: Small bowel volvulus (SBV) is a surgical emergency that requires prompt diagnosis and treatment. Although sudden onset acute abdominal pain is the most common presenting symptom, the clinical presentation of SBV can be misleading. Early diagnosis and treatment are therefore crucial for a good outcome.
Case Report: A 49-year-old woman presented with a 5-hour history of nausea as her only symptom. Six hours after admission, she developed multiple episodes of vomiting, but without abdominal pain. An urgent CT of the abdomen revealed a pathognomonic “whirl” pattern highly suggestive of SBV, and emergency laparoscopy revealed ileal volvulus without any identifiable pathoetiological factors. She underwent simple devolvulation and made a rapid recovery without recurrence at 12 months.
Conclusion: This case highlights that the preoperative clinical diagnosis of small bowel volvulus can be challenging, emphasizing the importance of preoperative imaging and maintaining a high index of suspicion to avoid missing this important diagnosis. A laparoscopic approach can be used successfully to treat SBV.
Keywords: Computed tomography, Diagnosis, Small bowel volvulus, Whirl sign
Introduction
Small bowel volvulus (SBV), although uncommon in adults, can lead to intestinal obstruction, venous engorgement, gangrene, and perforation [1]. Small bowel volvulus can be either primary or secondary, depending on the etiology [2]: primary SBV occurs when there is no identifiable cause for torsion of the mesenteric root, while secondary SBV is associated with various anatomical and acquired factors [1],[3]. The preoperative diagnosis of SBV can be challenging, as it lacks specific symptoms, signs, and laboratory findings. Moreover, abdominal imaging may not always provide sufficient information to confirm the diagnosis, leading to a delay in treatment that can be fatal [4]. Early detection and prompt surgical intervention are essential to prevent ischemic necrosis of the small bowel, which carries a high morbidity and mortality rate. Hence, clinicians should be aware of this rare but potentially lethal condition to ensure timely diagnosis and treatment to provide optimal care for their patients [5].
Case Report
A 49-year-old woman, with no prior medical or surgical history, presented to the emergency department with a 5-hour history of nausea but without vomiting or abdominal pain. Her nausea had developed after eating a large meal following a 16-hour period of fasting for religious reasons. She had taken a metoclopramide tablet at home, which helped to alleviate her nausea for a short time. Her bowel movements were regular, with the last one/two days ago. She was not taking any medications. On examination, her vital signs were within normal limits, and there was no fever.
On examination, her abdomen was slightly distended, but it was soft and non-tender. Bowel sounds were present. A digital rectal examination revealed an empty rectum.
Blood tests revealed a slightly elevated C-reactive protein (CRP) (Table 1), but her complete blood count was normal. Abdominal ultrasound was limited by excessive bowel gas, hindering a clear visualization of the abdomen. An orthostatic abdominal plain film showed meteorism of both the large and small bowel, but there were no air-fluid levels (Figure 1). Following evaluation by the internist, the patient was admitted to the medical department for further investigation, as the cause of her symptom was determined to be non-urgent.
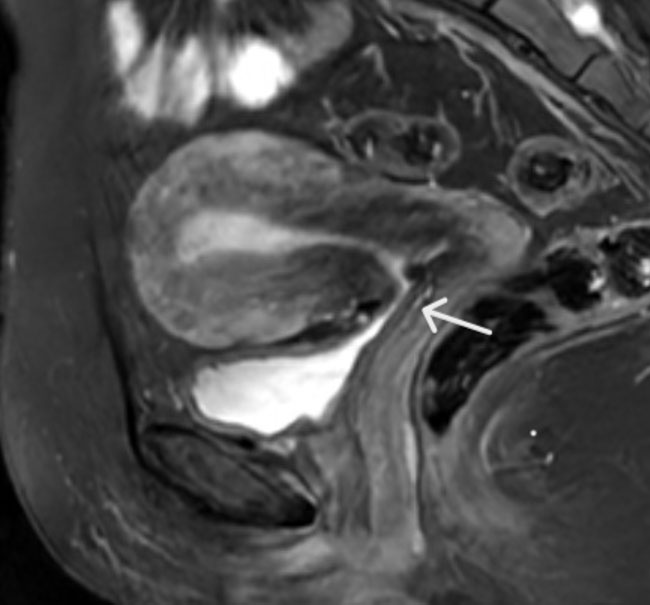
Although she was initially managed with bowel rest, fluid therapy, and intravenous administration of antiemetics, this only minimally improved the patient’s condition. Six hours later, the patient experienced multiple episodes of vomiting. On repeat abdominal examination, the abdomen remained soft, and there was still no guarding nor other signs of peritoneal irritation. She was awake, cooperative, and hemodynamically stable, and the rest of the physical examination was unremarkable. However, her CRP had risen further, but her white blood cell count remained within normal range (Table 1). An urgent computed tomography (CT) scan of the abdomen was conducted, which revealed a pathognomonic “whirl” pattern suggesting SBV (Figure 2). Following a surgical consultation, the decision was made to proceed with emergency laparoscopic exploration. Upon entering the abdomen, no free fluid was observed within the peritoneal cavity during the diagnostic panoramic view. Additionally, there was no malodor, and no adhesions were observed within the peritoneal cavity.
However, a clockwise twist in the ileum, approximately 2 m from the ileocecal valve, was identified associated with a twisted segment along the mesenteric axis. This finding confirmed the diagnosis of ileal volvulus. Additionally, the distal jejunum and proximal ileal loops showed mild distension. There was no evidence of obstructing bands or perforations.
The volvulus was successfully detorsed laparoscopically with minimal handling using an atraumatic grasper. Because there were no anatomical abnormalities, the detorsed segment of the ileum was not fixed in place. Although this segment initially appeared slightly discolored, it was deemed viable, and it gradually regained its normal color and shine. Also, normal peristaltic waves were observed to return. A thorough inspection confirmed that there were no other abnormalities, such as internal hernias or congenital anomalies.
Her inpatient stay was uncomplicated. She passed a bowel motion on the third postoperative day and was discharged from hospital on the same day. Before discharge, a stool sample was taken to rule out parasitic infections, which was returned as negative a few days later. At follow-up visits in the outpatient department one month and 12 months later, the patient was doing well with no history of relapse.



Discussion
Small bowel volvulus is less common in Western countries than in Asia, the Middle East, and Africa. The cause for these regional differences is still unknown, but people with low socioeconomic status, diabetic autonomic neuropathy, or parasitic infestation are at increased risk of SBV [6]. Sudden changes in dietary habits with consumption of food after long fasting are also known risk factors, as a sudden overloading of an empty bowel with a single voluminous meal may induce forceful bowel peristalsis, resulting in small bowel volvulus [4],[7]. In the absence of any other discernible pathology or etiology, our patient’s volvulus could be attributed to the ingestion of a substantial meal after a period of prolonged fasting.
The preoperative diagnosis of primary SBV is more difficult than secondary SBV. Several underlying causes, both congenital and acquired, can contribute to secondary small bowel volvulus. Congenital anomalies include malrotation, Meckel’s diverticulum, or an abnormally long mesentery, while acquired risk factors include post-surgical adhesions, bands, tumors, and internal hernias [8],[9].
Small bowel volvulus is an uncommon cause of small intestinal obstruction and frequently goes undetected until surgical intervention. The symptoms of SBV can sometimes closely resemble those of other causes of intestinal obstruction. However, the most common presenting symptom is sudden onset of acute abdominal pain. In our case, the patient did not report any abdominal pain, which may have been due to: (i) a high pain threshold (some individuals have a naturally high tolerance for pain); (ii) partial luminal obstruction, allowing passage of some intestinal contents and leading to mild distension or stretching of the proximal intestine and less or no distension-associated pain; and (iii) absence of a vascular insult, i.e., the volvulus did not compromise the blood supply to the affected intestine to cause ischemia, necrosis, and consequent severe pain.
In most cases, abdominal X-rays and ultrasound scans fail to provide definitive diagnostic clues; therefore, CT scans are crucial for evaluating suspected cases of small bowel volvulus. On CT imaging, potential signs of SBV include rotation of the mesentery and its associated blood vessels, dilated gut loops, and the presence of bowel ischemia (pneumatosis intestinalis, free peritoneal fluid, and portal vein gas) [10],[11]. Nevertheless, the diagnostic accuracy of abdominal contrast CT scan for SBV varies depending on the stage of the disease, the quality of the imaging, the presence of other conditions that can cause intestinal obstruction, and the experience of the radiologist. However, CT is generally 45–75% accurate, and CT is considered to be the most accurate imaging modality for diagnosing SBV [5],[12],[13]. In our case, we established the diagnosis of SBV preoperatively using CT, which showed the classic CT finding of an SBV “whirl sign," where the twisted, edematous mesentery appears as a swirling pattern on the scan. However, it is important to note that the absence of this sign does not rule out SBV [14].
One of the most serious complications of SBV is bowel necrosis. Fo et al. [15] identified several risk factors for necrosis in SBV, including elevated neutrophils, a prolonged disease course (>24 hours), and the presence of bloody ascites but not the direction of rotation, presence of peritonitis, and bowel sound status. Bloody ascites can develop in SBV patients due to disturbances in venous reflux, and it strongly suggests the possibility of intestinal necrosis.
Prompt surgical intervention is crucial when SBV is suspected to prevent the development of small bowel necrosis. The specific surgical approach is tailored to the viability of the small bowel, the abdominal anatomy, and the presence of other concomitant diseases. Simple devolvulation is frequently performed when the small bowel is viable and there are no other diseases, and small bowel resection is performed when it becomes gangrenous.
While management of secondary SBV involves addressing the underlying etiology, management of primary SBV remains controversial. Some surgeons advocate simple devolvulation [9], while others strongly recommend additional intestinal fixation (enteropexy) and even argue that resection is essential to prevent future episodes [7],[16]. While Bouassida et al. [17] discussed different techniques used to avoid recurrence, there is currently no consensus on how to achieve this. The risk of recurrence with detorsion alone is reported to be 30%, while enteropexy carries a risk of fistula formation [18]. Plication of the mesentery results in an increased risk of vascular injury, and prophylactic surgical resection of the torsional segment increases postoperative morbidity and lengthens the hospital stay.
Therefore, every potential solution has its risks and benefits, and we opted for detorsion alone given the lack of any identifiable underlying anatomical abnormality or pathology. There is some evidence to support this approach. Li et al. [5] reported that, in the absence of anatomical abnormalities, simple devolvulation without fixation is unlikely to lead to a high rate of recurrence. When anatomical abnormalities are present, such as a long small bowel or mesentery, fixation, or resection of the intestine might be necessary, depending on the surgeon’s expertise and the patient’s condition.
There are only a few studies on the laparoscopic treatment of SBV. Kim et al. reported a case of primary SBV, which was reduced laparoscopically with subsequent intestinal resection [19]. In our case, we were able to reduce the torsional segment laparoscopically, and segmental resection and fixation were unnecessary as the bowel segment remained viable, regained its normal color, and no secondary cause was identified. Depending on the individual case, a laparoscopic approach may also benefit patients due to reduced pain, tissue damage, recovery time, and hospital stay associated with the laparoscopic approach [20],[21]. However, the laparoscopic approach requires a high level of surgical skill and experience, and it may not be feasible in cases of extensive bowel necrosis or perforation [5]. Therefore, the decision to use the laparoscopic approach should be made on a case-by-case basis, considering the patient’s condition and the surgeon’s expertise.
Conclusion
The absence of specific symptoms and signs in the early stage of SBV often leads to a missed diagnosis or misdiagnosis, resulting in serious complications. Due to its variable presentation and high mortality rate, a high level of suspicion is required to diagnose small bowel volvulus. To avoid adverse outcomes, urgent abdominal CT scan and early surgical intervention are essential. While the laparoscopic approach may be an option for many SBV cases, its effectiveness depends on various factors such as the severity of the volvulus, timing of intervention, and the surgeon’s experience.
REFERENCES
1.
Brinda MAA, Manjunath S, Balasubramanya KS, Nanjaiah B. An unusual case of small bowel volvulus. J Clin Diagn Res 2015;9(11):PD08–10. [CrossRef]
[Pubmed]

2.
Tamura J, Kuniyoshi N, Maruwaka S, et al. “Whirl sign” of primary small bowel volvulus. West J Emerg Med 2014;15(4):359–60. [CrossRef]
[Pubmed]
3.
Gürleyik E, Gürleyik G. Small bowel volvulus: A common cause of mechanical intestinal obstruction in our region. Eur J Surg 1998;164(1):51–5. [CrossRef]
[Pubmed]
4.
Roggo A, Ottinger LW. Acute small bowel volvulus in adults. A sporadic form of strangulating intestinal obstruction. Ann Surg 1992;216(2):135–41. [CrossRef]
[Pubmed]
5.
Li X, Zhang J, Li B, et al. Diagnosis, treatment and prognosis of small bowel volvulus in adults: A monocentric summary of a rare small intestinal obstruction. PLoS One 2017;12(4):e0175866. [CrossRef]
[Pubmed]
6.
Patial T, Chaddha S, Rathore N, Thakur V. Small bowel volvulus: A case report. Cureus 2017;9(5):e1281. [CrossRef]
[Pubmed]
7.
Duke JH Jr, Yar MS. Primary small bowel volvulus: Cause and management. Arch Surg 1977;112(6):685–8. [CrossRef]
[Pubmed]
8.
Vaez-Zadeh K, Dutz W, Nowrooz-Zadeh M. Volvulus of the small intestine in adults: A study of predisposing factors. Ann Surg 1969;169(2):265–71. [CrossRef]
[Pubmed]
9.
Papadimitriou G, Marinis A, Papakonstantinou A. Primary midgut volvulus in adults: Report of two cases and review of the literature. J Gastrointest Surg 2011;15(10):1889–92. [CrossRef]
[Pubmed]
10.
Iwuagwu O, Deans GT. Small bowel volvulus: A review. J R Coll Surg Edinb 1999;44(3):150–5.
[Pubmed]
11.
Fisher JK. Computed tomographic diagnosis of volvulus in intestinal malrotation. Radiology 1981;140(1):145–6. [CrossRef]
[Pubmed]
12.
Ruiz-Tovar J, Morales V, Sanjuanbenito A, Lobo E, Martinez-Molina E. Volvulus of the small bowel in adults. Am Surg 2009;75(12):1179–82.
[Pubmed]
13.
Huang JC, Shin JS, Huang YT, et al. Small bowel volvulus among adults. J Gastroenterol Hepatol 2005;20(12):1906–12. [CrossRef]
[Pubmed]
14.
Berrocal T, Lamas M, Gutieérrez J, Torres I, Prieto C, del Hoyo ML. Congenital anomalies of the small intestine, colon, and rectum. Radiographics 1999;19(5):1219–36. [CrossRef]
[Pubmed]
15.
Fo Y, Kang X, Tang Y, Zhao L. Analysis of clinical diagnosis and treatment of intestinal volvulus. BMC Gastroenterol 2023;23(1):93. [CrossRef]
[Pubmed]
16.
Birnbaum DJ, Grègoire E, Campan P, Hardwigsen J, Le Treut YP. Primary small bowel volvulus in adult. J Emerg Med 2013;44(4):e329–30. [CrossRef]
[Pubmed]
17.
Bouassida M, Beji H, Chtourou MF, Ben Othmane N, Hamzaoui L, Touinsi H. Primary small bowel volvulus: A case report and literature review. Ann Med Surg (Lond) 2022;80:104250. [CrossRef]
[Pubmed]
18.
Tam A, Phong J, Yong C. Primary small bowel volvulus: Surgical treatment dilemma. ANZ J Surg 2019;89(11):1521–3. [CrossRef]
[Pubmed]
19.
Kim KH, Kim MC, Kim SH, Park KJ, Jung GJ. Laparoscopic management of a primary small bowel volvulus: A case report. Surg Laparosc Endosc Percutan Tech 2007;17(4):335–8. [CrossRef]
[Pubmed]
20.
Agrawal S, Yadav AR, Nepal B, Upadhyay PK. Primary ileal volvulus: A rare twist in an elderly patient—case report. BMC Surg 2020;20(1):237 [CrossRef]
[Pubmed]
21.
Otani K, Ishihara S, Nozawa H, et al. A retrospective study of laparoscopic surgery for small bowel obstruction. Ann Med Surg (Lond) 2017;16:34–9. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Acknowledgments
We are thankful to the patient for allowing us to report her medical report as a case report.
Author ContributionsGhassan Almaimani - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthor declares no conflict of interest.
Copyright© 2024 Ghassan Almaimani. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}