 |
Case Report
Glioblastoma multiforme mimicking frontotemporal dementia: A case report
1 Department of Medicine, Iguaçu University - UNIG - RJ, Brazil
2 Department of Neurology, Federal University of Rio de Janeiro - UFRJ - RJ, Brazil
3 Iguaçu University - UNIG - Department of Neurology of Hospital Geral de Nova Iguaçu - RJ, Brazil
Address correspondence to:
Antônio Marcos da Silva Catharino
Iguaçu University - UNIG - Department of Neurology of Hospital Geral de Nova Iguaçu - RJ,
Brazil
Message to Corresponding Author
Article ID: 101436Z01MO2024
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Orsini M, de Freitas MRG, Vieira PC, Reis CHM, Vieira G, da Silva Catharino AM. Glioblastoma multiforme mimicking frontotemporal dementia: A case report. Int J Case Rep Images 2024;15(1):12–16.ABSTRACT
Glioblastoma (GBM) is the most common and aggressive primary brain tumor in adults. In this case a 57-year-old male patient had cognitive decline, visual dysfunction, and memory loss. He is not able to interact during the medical consultation. The brain Magnetic Resonance Imaging (MRI) showed an infiltrative and expansive lesion compressing the third ventricle and extending to midbrain to the left. The anatomopathological report concluded the diagnosis of Grade IV glioblastoma and the patient will undergo to surgical intervention.
Keywords: Brain magnetic resonance imaging, Glioblastoma, Primary brain tumor
Introduction
Glioblastoma (GBM) is the most common and most lethal and aggressive primary brain tumor in adults [1],[2]; statistics in the United States and Germany has indicated that during childhood it is relatively rare and accounts for less than 3% of childhood brain tumors [3],[4]. The first case of GBM was reported in 1928, the treatment of this neoplasm showed significant improvement and the mean time between diagnosis and patient death increased from 6 to 15 months between 1940 and 2010 [5]. Classified as primary (GBM) arises without a known clinical precursor tumor or secondary derived from the evolution of high-grade malignancy from a previous glioma. Its histopathological features are commonly a grade IV astrocytic neoplastic process, with significant tumoral necrosis and microvascular proliferation [1],[2]. Surgery is the only curative strategy. The association of concomitant treatment with concurrent alkylating chemotherapy and radiotherapy improves survival of patients but is associated with toxicity. However, even with the use of these therapies, the prognosis of patients is restricted with an average survival of 15 months [1],[2].
Case Report
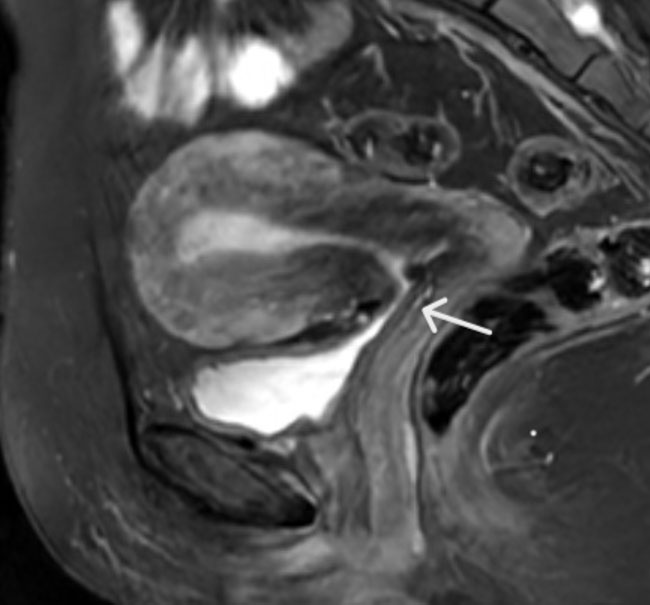
A 57-year-old male was presented with hypertension and dyslipidemia as co-morbidities. His wife reported that he has been presenting cognitive decline and social withdrawal for about seven months. In addition, there had been numerous episodes of executive processing errors, visuospatial dysfunction, and short- and long-term memory dysfunction. Aspects related to hygiene are neglected and sometimes not performed in private places. Vague staring, short answers, poor vocabulary, and, undoubtedly, decline in all aspects of basic and instrumental activities mark the vast cognitive dullness. The patient was not able to interact during the neurological examination, making him/her impaired. Laboratory test was normal. Brain Magnetic Resonance Imaging (MRI) showed an infiltrative lesion with an expansive effect, slightly hyperintense on T2 and FLAIR, hypointense on T1, without enhancement and absence of signs of restricted diffusion affecting the thalamus bilaterally (Figure 1), compressing the third ventricle and extending inferiorly to the midbrain to the left. Changes in the signal of the hippocampi (Figure 2) and tonsils by extension of the referred lesion, being larger on the right, were identified. It was noteworthy that headache, diplopia, convulsive crises, nausea and vomiting, paralysis or paresis of the limbs were not reported in the neurological examination or through verbalization of the wife. In contrast, changes in mood and personality, speech, and learning difficulties were identified. The anatomopathological report concluded the diagnosis of Grade IV glioblastoma. The patient was undergone to surgical intervention.


Discussion
Glioblastoma is an anaplastic glioma with predominantly astrocytic differentiation, classified by the WHO as a Grade IV tumor and corresponds to the most common and aggressive type among malignant brain tumors [6],[7],[8],[9]. Glioblastoma is characterized by being undifferentiated, having rapid infiltrative growth and presenting necrosis and microvascular proliferation. The presence of necrosis histologically differentiates it from low-grade gliomas [6],[7],[8],[9],[10],[11]. According to the Central Brain Tumor Registry of the United States (CBTRUS) from 2010 to 2014 GBM represents 47.1% of malignancies and 14.9% of all central nervous system (CNS) tumors. Its incidence increases with age, affecting adults after the age of 50–55 years, with the average age of diagnosis at 64 years and with more than half of cases over 65 years [9],[12]. It has a peak incidence between 75 and 84 years, decreasing after this age. Between 0 and 19 years represent only 3% of all CNS tumors. It is 1.58 times more common in men than in women and 1.93 times more common in Caucasians than in Blacks [11].
The most commonly occurring malignant brain or other CNS tumor was glioblastoma (14.6% of all tumors), and the most common non-malignant tumor was meningioma (37.6% of all tumors). According to recent studies, glioblastoma is the most common CNS tumor in men, while meningioma is more common in women. In the years between 2012 and 2016, there were 79,718 deaths from malignant tumors and other CNS tumors and it was estimated that around 86,000 new cases of CNS tumors would be diagnosed in the United States in 2019 [13]. The patient reported here is 57 years old, the age group in which the GBM in general is more frequent, according to the medical literature.
The clinical presentation of patients varies according to the location of the lesion, characterized by cognitive symptoms, seizures, focal neurological deficits, motor deficits of homonymous hemianopsia. In cases where the tumor originates in non-eloquent areas, patients present with intracranial hypertension with headache, vomiting, and papilledema [14],[15],[16],[17]. The most common symptom is headache, present in 30–50% of cases [12]. When it affects the frontal lobe, it can cause personality change, which occurs in 20–40% of the patients. Rarely, it may mimic a stroke due to intratumoral hemorrhage [16]. In this case reported the patient had no focal signs, headache, diplopia, convulsive crises, nausea and vomiting, paralysis or paresis of the limbs were not reported in the neurological examination. Symptoms of malignant brain tumors include headache, seizures, neurocognitive impairment, and focal neurologic deficits, signs, and symptoms reported in numerous scientific articles [18],[19],[20].
The standard diagnostic test when GBM is suspected is MRI [18],[21]. It initially affects the periventricular and subcortical white matter and is in the supratentorial region in 95% of cases, with a higher incidence in the frontal lobe [12],[18] and presents a heterogeneous lesion with necrosis, hemorrhage, and peritumoral edema with consequent deviation of median line.
The definitive diagnosis is classically given by histopathological analysis, with visualization mainly of necrosis and microvascular proliferation [22]. The 2016 WHO Classification considers both histopathological and molecular characteristics in the diagnosis, thus GBM was divided, according to the presence or not of isocitrate dehydrogenase (IDH) mutations type 1 or type 2, into GBM IDH-wild, IDH-mutant, and Not Otherwise Specified (NOS) [6],[10].
The IDH-wild GBM is the most common (90%), corresponds more frequently to the primary GBM, predominates over 55 years, has a median survival with a maximum treatment of 15 months. While the IDH-mutant GBM is less common (10%), corresponds more to secondary GBM, affects younger patients, and has a better prognosis—survival with maximum treatment of 31 months [12],[22].
Despite intensive treatment and new findings, the prognosis is poor, with a median survival of 13.4–19.9 months and a 5-year survival of 5.5% and a disease-free survival of 7–8 months [22],[23]. In the absence of treatment, the median survival is 3 months, evidencing the aggressiveness of the disease [12],[24].
The standard treatment for GBM is surgical resection with adjuvant chemoradiotherapy. Surgery plays a central role in the management of GBM with diagnostic objectives, symptomatic relief, increased survival, and decreased need for corticosteroids [25],[26],[27]. Total resection should be sought—however, location in eloquent areas or infiltration in the corpus callosum may allow only partial resection, and in 20–30% of cases GBM are unresectable [28].
Chemotherapy alkylating and radiotherapy association with the surgical treatment improves survival of patients but is associated with toxicity. However, even with the use of these therapies, the prognosis of patients is restricted with an average survival of 15 months [1],[2].
Conclusion
The case reported here was consistent with reports published in the literature regarding clinical presentation, imaging patterns, and histopathology.
REFERENCES
1.
Zhao YH, Wang ZF, Pan ZY, et al. A meta-analysis of survival outcomes following reoperation in recurrent glioblastoma: Time to consider the timing of reoperation. Front Neurol 2019;10:286. [CrossRef]
[Pubmed]

2.
Brown TJ, Brennan MC, Li M, et al. Association of the extent of resection with survival in glioblastoma: A systematic review and meta-analysis. JAMA Oncol 2016;2(11):1460–9. [CrossRef]
[Pubmed]
3.
Kaatsch P, Rickert CH, Kühl J, Schüz J, Michaelis J. Population-based epidemiologic data on brain tumors in German children. Cancer 2001;92(12):3155–64. [CrossRef]
[Pubmed]
4.
Ostrom QT, Gittleman H, Farah P, et al. CBTRUS statistical report: Primary brain and central nervous system tumors diagnosed in the United States in 2006–2010. Neuro Oncol 2013;15(Suppl 2):ii1–56. [CrossRef]
[Pubmed]
5.
Wick W, Osswald M, Wick A, Winkler F. Treatment of glioblastoma in adults. Ther Adv Neurol Disord 2018;11:1756286418790452. [CrossRef]
[Pubmed]
6.
Louis DN, Perry A, Reifenberger G, et al. The 2016 World Health Organization classification of tumors of the central nervous system: A summary. Acta Neuropathol 2016;131(6):803–20. [CrossRef]
[Pubmed]
7.
Czarnywojtek A, Borowska M, Dyrka K, et al. Glioblastoma multiforme: The latest diagnostics and treatment techniques. Pharmacology 2023;108(5):423–31. [CrossRef]
[Pubmed]
8.
Makowska M, Smolarz B, Romanowicz H. microRNAs (miRNAs) in glioblastoma multiforme (GBM)-recent literature review. Int J Mol Sci 2023;24(4):3521. [CrossRef]
[Pubmed]
9.
Vaz-Salgado MA, Villamayor M, Albarrán V, et al. Recurrent glioblastoma: A review of the treatment options. Cancers (Basel) 2023;15(17):4279. [CrossRef]
[Pubmed]
10.
Louis DN, Perry A, Wesseling P, et al. The 2021 WHO classification of tumors of the central nervous system: A summary. Neuro Oncol 2021;23(8):1231–51. [CrossRef]
[Pubmed]
11.
Ostrom QT, Gittleman H, Liao P, et al. CBTRUS Statistical Report: Primary brain and other central nervous system tumors diagnosed in the United States in 2010–2014. Neuro Oncol 2017;19(suppl_5):v1–88. [CrossRef]
[Pubmed]
12.
Thakkar JP, Dolecek TA, Horbinski C, et al. Epidemiologic and molecular prognostic review of glioblastoma. Cancer Epidemiol Biomarkers Prev 2014;23(10):1985–96. [CrossRef]
[Pubmed]
13.
Ostrom QT, Cioffi G, Gittleman H, et al. CBTRUS statistical report: Primary brain and other central nervous system tumors diagnosed in the United States in 2012–2016. Neuro Oncol 2019;21(Suppl 5):v1–00. [CrossRef]
[Pubmed]
14.
Mesquita Filho PM, Espanhol RA, Azambuja ND, Varela DL, Rodriguez R. Multicentric giant cell glioblastoma: Case report and revision of the literature. Neurosurg Q 2016;26(1):64–8.
15.
Naydenov E, Bussarsky V, Nachev S, Hadjidekova S, Toncheva D. Long-term survival of a patient with giant cell glioblastoma: Case report and review of the literature. Case Rep Oncol 2009;2(2):103–10. [CrossRef]
[Pubmed]
16.
Montazer F, Torabizadeh Z, Sheidaie S. Giant cell glioblastoma multiforme: A case report. Int J Curr Res 2014;6(11):10182–4.
17.
Margetts JC, Kalyan-Raman UP. Giant-celled glioblastoma of brain. A clinico-pathological and radiological study of ten cases (including immunohistochemistry and ultrastructure). Cancer 1989;63(3):524–31. [CrossRef]
[Pubmed]
18.
Hanif F, Muzaffar K, Perveen K, Malhi SM, Simjee ShU. Glioblastoma multiforme: A review of its epidemiology and pathogenesis through clinical presentation and treatment. Asian Pac J Cancer Prev 2017;18(1):3–9. [CrossRef]
[Pubmed]
19.
Heemann GC, Heemann ACC. Newly diagnoses glioblastoma multiforme: Diagnosis and initial surgical treatment. Acta Medica 2018;39(2).
20.
Schaff LR, Mellinghoff IK. Glioblastoma and other primary brain malignancies in adults: A review. JAMA 2023;329(7):574–87. [CrossRef]
[Pubmed]
21.
Chawla S, Boal DKB, Dillon PW, Grenko RT. Best cases from the AFIP: Splenic Torsion. RadioGraphics 2003;23(2):305–8. [CrossRef]
22.
Nørøxe DS, Poulsen HS, Lassen U. Hallmarks of glioblastoma: A systematic review. ESMO Open 2017;1(6):e000144. [CrossRef]
[Pubmed]
23.
Hung AL, Garzon-Muvdi T, Lim M. Biomarkers and immunotherapeutic targets in glioblastoma. World Neurosurg 2017;102:494–506. [CrossRef]
[Pubmed]
24.
Miranda A, Blanco-Prieto M, Sousa J, Pais A, Vitorino C. Breaching barriers in glioblastoma. Part I: Molecular pathways and novel treatment approaches. Int J Pharm 2017;531(1):372–88. [CrossRef]
[Pubmed]
25.
Li YM, Suki D, Hess K, Sawaya R. The influence of maximum safe resection of glioblastoma on survival in 1229 patients: Can we do better than gross-total resection? J Neurosurg 2016;124(4):977–88. [CrossRef]
[Pubmed]
26.
Bower M, Waxman J. Central nervous system cancers. Lect Notes Oncol 2016;2011:96–7.
27.
Weller M, van den Bent M, Hopkins K, et al. EANO guideline for the diagnosis and treatment of anaplastic gliomas and glioblastoma. Lancet Oncol 2014;15(9):e395–403. [CrossRef]
[Pubmed]
28.
Preusser M, de Ribaupierre S, Wöhrer A, et al. Current concepts and management of glioblastoma. Ann Neurol 2011;70(1):9–21. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Marco Orsini - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Marcos RG de Freitas - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Paulo Cezar Vieira - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Carlos Henrique Melo Reis - Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Gabriela Vieira - Conception of the work, Design of the work, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Antônio Marcos da Silva Catharino - Conception of the work, Design of the work, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2024 Marco Orsini et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}