 |
Case Report
Giant myxoid liposarcoma of the gluteal region: Resection and buttock reconstruction
1 Chief Consultant and HOD, Department of Plastic Surgery, Vivekananda Polyclinic and Institute of Medical Sciences, Lucknow, Uttar Pradesh, India
2 Vivekananda Polyclinic and Institute of Medical Sciences, Lucknow, Uttar Pradesh, India
Address correspondence to:
Tarun Kumar
Vivekananda Polyclinic and Institute of Medical Sciences, Uttar Pradesh
India
Message to Corresponding Author
Article ID: 101413Z01AG2023
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Agarwal A, Kumar T. Giant myxoid liposarcoma of the gluteal region: Resection and buttock reconstruction. Int J Case Rep Images 2023;14(2):69–74.ABSTRACT
Introduction: Soft tissue sarcoma in adult is a rare disease and it needs an interdisciplinary team management. Liposarcoma has mesenchymal origin and arises in the fatty tissue. Multiple histologic subtypes of liposarcoma are recognized, including myxoid liposarcoma. In two-third of the cases, this tumor occurs in the muscle while often demonstrating a misleading benign appearance. Myxoid liposarcoma occurs predominantly in the deep soft tissues of the extremities and has the ability of metastasis to a wide range of soft tissue. Surgery is the main therapeutic modality in treatment of soft tissue sarcoma.
Case Report: Presenting an exceptional case of a 50-year-old woman with history of painless large swelling of size 28×21×13 cm in left gluteal region since one year with rapid progression over three months. It was diagnosed as low grade myxoid liposarcoma of the left buttock. This is the largest reported case of myxoid liposarcoma of extremities in Asia found in literature. The patient was treated with complete excision of tumor with gluteus maximum muscle. Gluteus minimus flap was elevated to cover the exposed sciatic nerve and buttock recontouring was done as single procedure for aesthetically favorable results followed by post-operative radiotherapy and necessary follow-ups.
Conclusion: Buttock contouring done post-resection as single procedure is more acceptable by the patient and has got superior aesthetic results.
Keywords: Buttock reconstruction, Myxoid liposarcoma, Radiotherapy
Introduction
Malignant sarcomas comprise approximately 1% of all soft-tissue tumors [1],[2]. Liposarcoma accounts for 16–18% of all soft tissue sarcomas [3] and is the most common sarcoma of the lower extremities. Myxoid liposarcoma is the second most common liposarcoma variant, characterized by lipomatous differentiation with a myxoid stroma and comprise of 30–40% of all liposarcomas [4],[5]. It presents as a large, slow-growing, painless mass, and needs thorough preoperative investigation including biopsy with metastatic workup [2]. Biopsy determines the variant of liposarcoma with grade of tumor which is pivotal for the line of treatment and also provides information about the percentage of round cells which tells about the degree of differentiation and affects the prognosis [6]. The treatment method for myxoid liposarcoma is confirming negative margins post-wide local excision followed by adjuvant radiotherapy or chemotherapy or both based on the risk of recurrence with metastatic disease [1].
The aim of this case report is to present our experience in the management of a giant myxoid liposarcoma of left gluteal region both functionally and aesthetically.
Case Report
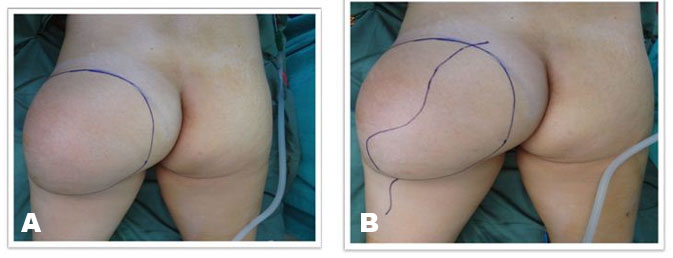
A 50-year-old woman presented with a painless, slowly growing swelling of the left gluteal region for one year with rapid increase in size in the past three months. There was no history of loss of weight, appetite, and fever with no significant past history. On local examination, the swelling was 28×21×13 cm, irregular in shape with smooth surface, non-tender, firm to hard in consistency, with reduced mobility with no fixity to skin (Figure 1). There were no signs of sciatic nerve compression with normal sensory motor examination of the ipsilateral limb. There was no evidence of inguinal lymphadenopathy.
Magnetic resonance imaging (MRI) of the gluteal region showed a well-defined lobulated lesion, measuring approximately 20×15.5×8.5 cm noted in left gluteal region, epicentered in gluteus maximus muscle, abutting quadratus femoris, and obturator internus muscles with preserved fat planes. Anteriorly the mass was seen indenting onto the sciatic nerve. No obvious involvement of underlying bone or overlying subcutaneous plane was seen (Figure 2A and Figure 2B).
Fine Needle Aspiration Cytology (FNAC) of the mass gave the impression of low grade mesenchymal tumor of myxoid variant. Biopsy was done and diagnosed to be low grade myxoid liposarcoma. Metastatic workup was done with high-resolution computed tomography (HRCT) thorax, ultrasonography (USG) whole abdomen, and CT abdomen to look for metastasis in lungs and liver but were found to be normal.
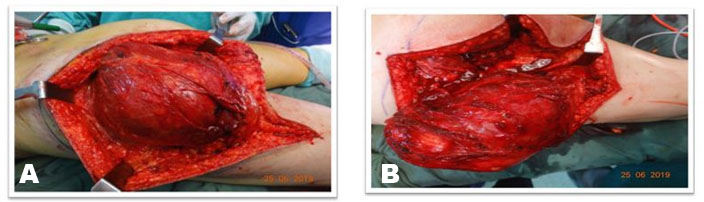
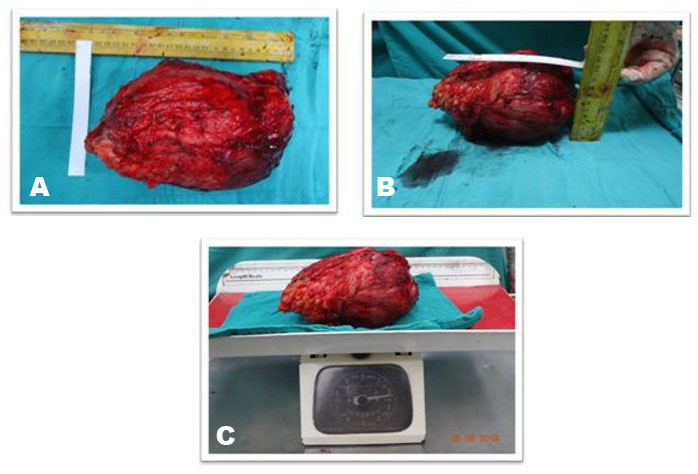
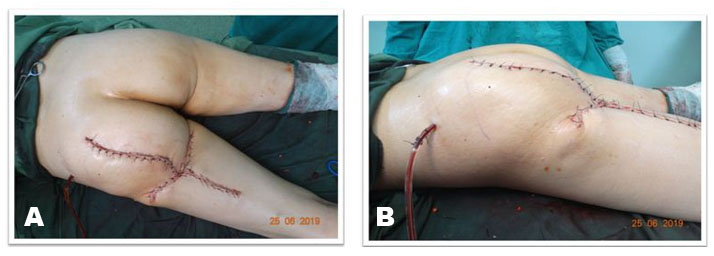
Surgical excision was planned after routine investigations. The patient was put in prone position under regional anesthesia. The skin was incised with S-shaped incision centered over the gluteal region extending 4 cm below the gluteal crease over the left thigh (Figure 3A and Figure 3B). The subcutaneous tissues were thinned out and fat was found atrophied. The fascia covering the gluteus maximus muscle was incised superiorly and the tumor was seen arising from the gluteus maximus muscle (Figure 4). At inferior margin of gluteus maximus muscle near the gluteal crease, the tumor was seen extending inferiorly into the subcutaneous fat. The sciatic nerve was identified and looped inferiorly in the thigh and was then traced superiorly. Dissection was done in the plane between the tumor and the sciatic nerve above the gluteal crease. The tumor was found indenting the nerve but the fat planes between tumor and the nerve were preserved. Complete excision of the tumor was done including the gluteus maximus muscle (Figure 5A). The exposed sciatic nerve was covered with gluteus minimus muscle to protect the irritation of nerve from surrounding structures (Figure 5B). The tumor measured 23×19×10 cm in dimensions and weighed 2.2 kg (Figure 6A, Figure 6B, Figure 6C).
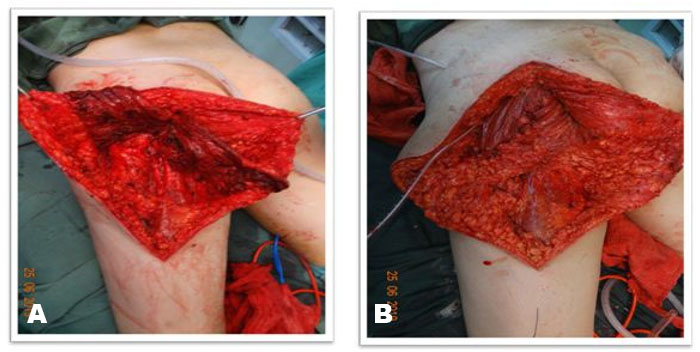
After excision, examination of bilateral gluteal for symmetry was started. Left gluteal region lacked enough support and bulk and had flattened appearance, so gluteal contouring was planned. The growing tumor had worked as a tissue expander resulting in excess skin in both horizontal and vertical directions. To achieve better gluteal symmetry, the medial skin flap was de-epithelized for 12 cm along the whole length. The adipofascial flap was then advanced and sutured on the undersurface of the lateral flap and the floor of defect to provide bulk in the region (Figure 7A and Figure 7B). To avoid dog-ear formation due to excess tissue in transverse plane, a limited skin excision was done at the level of gluteal crease. This resulted in symmetry of buttock region with better buttock contour and buttock crease formation giving an aesthetically pleasing result (Figure 8A and Figure 8B). Closure was done in layers over a suction drain placed below the de-epithelized flap which was removed on fifth postoperative day. It was followed by an uneventful wound healing with a superior aesthetic and satisfactory functional results.
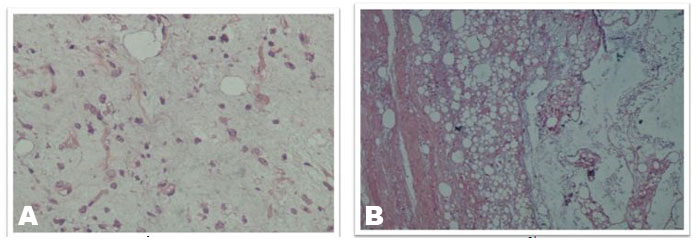
On histopathological examination, the mass was confirmed to be myxoid liposarcoma of the gluteal region. Small to large nodules composed of proliferated small bland non-lipoblast like primitive round to oval mesenchymal cells dispersed in abundant loose myxoid stroma along with several thin arborizing capillaries were seen. There were areas of abundant interstitial edema with clearing suggesting lymphangiectasia and focal areas of condensation of small round cells at periphery. Mitotic activity was sparse. The skeletal muscle tissue was largely preserved and some focal interstitial hemorrhage. The resected margins were free of tumor (Figure 9A and Figure 9B).
According to the French Fédération Nationale des Centres de Lutte Contre le Cancer (FNCLCC), it was a Grade 1 Myxoid liposarcoma (low grade). After discussion with the oncosurgery team, adjuvant radiation therapy was recommended for the patient. The patient underwent adjuvant radiotherapy (66 Gy), six weeks after surgery in the form of external beam radiation therapy (EBRT).
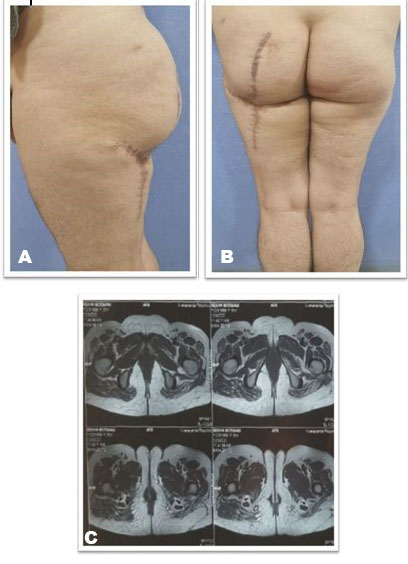
Magnetic resonance imaging scan of left gluteal and thigh region after one year of follow-up did not show any evidence of recurrence (Figure 10C) and the patient was put on six month follow-up for next five years and annually for next five years. Follow-up result after one year shows good buttock contour and symmetry with no functional deficit at the hip joint (Figure 10A and Figure 10B).



Discussion
Liposarcoma is a mesenchymal malignant tumor arising from adipose tissue which most commonly originates under the superficial fascia [1]. The World Health Organization [7] classified liposarcomas into three different subtypes according to the molecular and clinicopathological differences
- Well-differentiated/de-differentiated liposarcoma
- Pleomorphic liposarcoma
- Myxoid/round-cell liposarcoma
Myxoid variant is one of the major subtypes of liposarcoma and occurs mainly in the lower extremities, followed by the retroperitoneum and trunk. Approximately 10% of patients with myxoid liposarcoma experience metastasis [8]. A direct correlation between the percentage of round cells in histopathological examination and distant metastasis has been documented. Myxoid variant with more than 10% round cells has increased rate of distant metastasis attributing to high grade liposarcoma [9]. The common sites of metastases are thorax, retroperitoneum, and abdominal cavity [8]. Computed tomography chest and abdomen with pelvis is recommended for adequate staging and surveillance of myxoid liposarcoma [10].
Management of myxoid liposarcomas (MLs) depends on the staging and grade of tumor. Treatment includes surgery, radiation therapy—neoadjuvant or adjuvant or both and systemic chemotherapy—neoadjuvant or adjuvant or both. Surgery is the mainstay treatment of MLs, and the standard procedure is wide local excision with negative resection margins of = 10 mm of adjacent tissue [11]. Patients with subcutaneous and intramuscular sarcomas treated with wide excision alone shows a local recurrence rate of 5–10% [5]. Myxoid liposarcoma is highly radiosensitive, therefore, adjuvant radiation therapy is commonly utilized to control local spread, especially in patients with high grade, deep lesions of > 5 cm. Neoadjuvant radiotherapy can also be given in patients with myxoid liposarcoma (LPS) but surgical resection of tumor after it becomes difficult due to post-radiotherapy scarring of soft tissues, resulting in functionally inferior results. Radiotherapy acts by decreasing myxoid stroma produced by tumor cells, vascular damage, and adipocyte maturation [12]. Neoadjuvant or adjuvant chemotherapy is also a treatment option for patients with ML. Neoadjuvant chemotherapy with anthracycline and ifosfamide in patients with large, high grade tumors and in histological types like synovial sarcoma and myxoid liposarcoma has been found responsive [5]. Adjuvant chemotherapy is given in patients with high risk of recurrence and metastatic disease [13].
Yoshihiro Nishida et al. reported a case series of 53 patients of myxoid liposarcoma of extremities and trunk wall with overall survival of 90% at five years and 83% at 10 years after complete surgical excision with marginal clearance. All patients were analyzed with respect to disease-free survival, which was 77% at both 5 and 10 years [14]. The index case of low-grade tumor reported here was managed with complete surgical excision of tumor along with buttock recontouring in a single stage followed by postoperative radiotherapy. With R0 resection of tumor and no secondary metastasis, adjuvant chemotherapy was not given.
Buttock contouring can also be planned as a secondary procedure six months to one year after the initial surgery. The results would have been inferior to that achieved in the first stage as the excess expanded skin utilized as an adipofascial flap would not be available. Tissue expansion involves a combination of mechanical creep and biological creep. A constant force applied to stretch the skin, to continuously extend it is mechanical creep. The skin and other underlying tissues enlarges after applying a constant force is biological creep. In tissue expansion, the tissue is stretched without affecting the quality of the original tissue [15]. Similar phenomenon of tissue expansion was noticed due to rapidly growing tumor in buttock and was utilized for buttock recontouring after tumor excision.
Buttock reconstruction is commonly done with tumescent liposculpture [16] or with a muscle flap cover [9]. Buttock reconstruction with tridimensional combined gluteoplasty can correct asymmetry and/or contour deformities. The combination of liposuction, intramuscular buttock implant placement, and fat transfer to the lateral third of the gluteus, corresponding to the hip and above the placed implant, is a procedure that can be performed as both primary and secondary procedure. This technique is especially indicated in patients with a limited amount of fat insufficient to achieve complete augmentation of gluteal region. Ideal patients for this procedure are the patients with significant deficits in projection and volume of lateral third of gluteus and/or hip, those with a limited amount of fat tissue available for transfer, those who underwent revision surgery, those with large defect after resection of tumor say liposarcoma, and those who desires larger average volume and projection [17].
Buttock reconstruction with only fat grafting procedure has risk of fatal fat embolization and needs large volumes of fat graft harvesting. Introduction of composite buttock augmentation has minimized the above complication and difficulty by using intramuscular implant placement, progressive instrument dissection, and targeted subcutaneous fat grafting giving good aesthetic results and also the problem of inadequate central mound projection can be corrected in single session rather than multiple rounds of fat transplantation [18].
Buttock reconstruction with fasciocutaneous local flaps is also a reliable technique. Gluteal fold fasciocutaneous V-Y advancement flap is a better method for buttock reconstruction having minimal donor site scar and acceptable degree of flap advancement and also creates a prominent gluteal crease.
Gluteus maximus perforator based island flap can be used as a fasciocutaneous or musculocutaneous flap depending on the need of thickness required. Similarly, infragluteal perforator flap is a versatile and reliable flap for buttock reconstruction with minimal donor site morbidity and good flap mobility [19].
As a secondary procedure, the patient may need to go through multiple fat grafting sittings for buttock contouring and such an amount of fat graft harvesting would have been very difficult as the patient was quite thin. Harvest and inset of a muscle flap would have been difficult due to post-radiotherapy scarring of adjacent muscles, vessels, and other soft tissues causing difficulty in dissection of the loco-regional muscle flaps and anastomosis of distant free flaps.
The largest liposarcoma of extremities reported in literature so far was from the European subcontinent of size 27×25 cm of right thigh which was well differentiated variant of liposarcoma. It was treated with en bloc excision of tumor [20].
The presented case is the largest liposarcoma of myxoid variety of extremities reported in Asia and the third largest liposarcoma of extremities reported in the world found in literature [10],[20].
This case report highlights the merit of complete excision of tumor with adjuvant radiotherapy and advantage of buttock contouring being done as single procedure utilizing the expanded skin over gluteal region showing excellent results aesthetically and functionally.
Conclusion
Present case signifies the importance of early surgical intervention for good functional results and utilization of expanded tissue as a result of rapidly growing tumor as adipofascial flap to recontour the buttock after complete surgical resection which also aided in adjuvant radiotherapy and also procured better aesthetic result. Here a line of management for a rapidly growing myxoid liposarcoma of extremities is specified in which after complete investigations and thorough metastatic workup, an early complete surgical excision of tumor should be performed with appropriate and aesthetically superior reconstruction option, with a systematic histopathological examination followed by adjuvant radiotherapy with or without chemotherapy. The patient undergoes regular follow-ups both clinically and radiologically to monitor the recurrence of tumor.
REFERENCES
1.
Blum A, Henrot P, Sirveaux F, et al. Diagnostic des lipomes des parties molles et des liposarcomes chez l'adulte. In: Laredo JD, editor. Conduite à tenir devant une image osseuse ou des parties molles d'allure tumorale Monographie du GETROA. Paris: Sauramps Medical; 2004, Vol. 31, p. 401–16.

2.
Dujardin F, Debled M, Guillemet C, et al. Diagnosis and treatment of soft-tissue tumors. [Article in French]. Rev Chir Orthop Reparatrice Appar Mot 2006;92(7):637–50. [CrossRef]
[Pubmed]
3.
Munk PL, Lee MJ, Janzen DL, et al. Lipoma and liposarcoma: Evaluation using CT and MR imaging. AJR Am J Roentgenol 1997;169(2):589–94. [CrossRef]
[Pubmed]
4.
Dei Tos AP. Lipomatous tumours. Curr Diag Pat 2001;7(1):8–16. [CrossRef]
5.
Fletcher CDM, Unni KK, Mertens F. World Health Organization Classification of Tumours. Pathology And Genetics of Tumours of Soft Tissue and Bone. Lyon: IARC Press; 2002, Vol. 1, p. 1–46.
6.
King DM, Hackbarth DA, Kilian CM, Carrera GF. Soft-tissue sarcoma metastases identified on abdomen and pelvis CT imaging. Clin Orthop Relat Res 2009;467(11):2838–44. [CrossRef]
[Pubmed]
7.
Weiss SW, Rao VK. Well-differentiated liposarcoma (atypical lipoma) of deep soft tissue of the extremities, retroperitoneum, and miscellaneous sites. A follow-up study of 92 cases with analysis of the incidence of “dedifferentiation”. Am J Surg Pathol 1992;16(11):1051–8. [CrossRef]
[Pubmed]
8.
Moreau LC, Turcotte R, Ferguson P, et al. Myxoid\round cell liposarcoma (MRCLS) revisited: An analysis of 418 primarily managed cases. Ann Surg Oncol 2012;19(4):1081–8. [CrossRef]
[Pubmed]
9.
Tremp M, di Summa PG, Oranges CM, Schaefer DJ, Kalbermatten DF. Reconstruction of gluteal deformities: A systematic review and experience of four cases. J Plast Surg Hand Surg 2017;51(5):313–22. [CrossRef]
[Pubmed]
10.
Willburger JCF, Kettelhack C, Fuchs B, Schaefer DJ, Osinga R. Giant myxoid liposarcoma of the gluteal region: Case report of patient caused delay of surgical treatment and review of the literature. J Surg Case Rep 2018;2018(10):rjy265. [CrossRef]
[Pubmed]
11.
Schenone AD, Luo J, Montgomery L, Morgensztern D, Adkins DR, Van Tine BA. Risk-stratified patients with resectable soft tissue sarcoma benefit from epirubicin-based adjuvant chemotherapy. Cancer Med 2014;3(3):603–12. [CrossRef]
[Pubmed]
12.
Salduz A, Alpan B, Valiyev N, et al. Neoadjuvant radiotherapy for myxoid liposarcomas: Oncologic outcomes and histopathologic correlations. Acta Orthop Traumatol Turc 2017;51(5):355–61. [CrossRef]
[Pubmed]
13.
Eilber FC, Eilber FR, Eckardt J, et al. The impact of chemotherapy on the survival of patients with highgrade primary extremity liposarcoma. Ann Surg 2004;240(4):686–95. [CrossRef]
[Pubmed]
14.
Nishida Y, Tsukushi S, Nakashima H, Ishiguro N. Clinicopathologic prognostic factors of pure myxoid liposarcoma of the extremities and trunk wall. Clin Orthop Relat Res 2010;468(11):3041–6. [CrossRef]
[Pubmed]
15.
Ramanathan M, Kumar S, Shetkar G. Tissue expanders in facial reconstructive surgery. International Journal of Oral & Maxillofacial Surgery 2007;36(11):1058.
16.
Avendaño-Valenzuela G, Guerrerosantos J. Contouring the gluteal region with tumescent liposculpture. Aesthet Surg J 2011;31(2):200–13. [CrossRef]
[Pubmed]
17.
Cárdenas-Camarena L, Trujillo-Méndez R, Díaz-Barriga JC. Tridimensional combined gluteoplasty: Liposuction, buttock implants, and fat transfer. Plast Reconstr Surg 2020;146(1):53–63. [CrossRef]
[Pubmed]
18.
Aslani A, Del Vecchio DA. Composite buttock augmentation: The next frontier in gluteal aesthetic surgery. Plast Reconstr Surg 2019;144(6):1312–21. [CrossRef]
[Pubmed]
19.
Kim JT, Kim YH, Naidu S. Perfecting the design of the gluteus maximus perforator-based island flap for coverage of buttock defects. Plast Reconstr Surg 2010;125(6):1744–51. [CrossRef]
[Pubmed]
20.
Costea R, Vasiliu E, Zarnescu NO, Hasouna M, Neagu S. Large thigh liposarcoma–Diagnostic and therapeutic features. J Med Life 2011;4(2):184–8.
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Amit Agarwal - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Tarun Kumar - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2023 Amit Agarwal et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}