 |
Case Report
A case report of osteochondroma of radial neck in a young adult
1 Professor, Department of Orthopaedics, JJM Medical College, Davangere, Karnataka, India
2 Junior Resident, Department of Orthopaedics, JJM Medical College, Davangere, Karnataka, India
Address correspondence to:
Navya Raj
Junior Resident, Department of Orthopaedics, JJM Medical College, Davangere, Karnataka,
India
Message to Corresponding Author
Article ID: 101395Z01SG2023
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Gupta SKG, Raj N. A case report of osteochondroma of radial neck in a young adult. Int J Case Rep Images 2023;14(1):119–122.ABSTRACT
Introduction: Osteochondroma, often referred to as exostosis, is the most common benign tumor characterized by a bony protuberance surrounded by cartilaginous surface, most commonly in proximal tibia, distal femur, proximal humerus. Our case was presented in a very unusual site, i.e., Radial neck.
Case Report: A case report of unusual manifestation of a solitary osteochondroma, i.e., exostosis, a common benign tumor but in a rare site, i.e., in the radial neck. We report this case due to its unusual site of presentation. The lesion for surgically managed.
Conclusion: Osteochondroma involving rare location such as radial neck can be challenging to diagnose for clinicians but with thorough examination and radiological studies the swelling was recognizable as osteochondroma and the patient was treated accordingly.
Keywords: Osteochondroma, Radial head, Rare, Solitary, Young
Introduction
Osteochondroma or solitary exostosis is a cartilage capped exophytic lesion that grows on the external surface of the bone containing a marrow cavity continuous with that of the parent bone. These lesions are sometimes referred to as osteocartilaginous exostosis. The term exostosis is a general term and is used to refer to any outgrowth of a bone from the cortical surface. Osteochondroma is the most common primary bone tumor comprising more than one-third of all benign bone tumors [1]. Osteochondroma accounts for 35–46% of all benign bone neoplasms. The incidence of osteochondroma under the age of 30 is higher in men compared to women [2]. Osteochondromas are usually thought to be benign bone tumors although they are more correctly thought of as developmental anomalies [3]. They usually affect bones that develop by enchondral ossification and rarely originate from bones that develop by intramembranous ossification such as the scapula, pubic rami, clavicle, and ribs [4]. The tumor grows in a direction away from the growing end of bone (possibly due to attached tendons or muscles pulling it away) with the cartilage cap pointing away from the physeal plate. When the normal growth stops (i.e., longitudinal growth), then the exostosis growth also stops. These lesions occur most frequently in long bones next to the metaphysis [5]. The most common sites are around the knees (distal femur and proximal tibia) followed by the proximal humerus. These tumors can also develop in unusual sites. Clinically, osteochondromas can be asymptomatic and found incidentally [6]. When an exophytic bone lesion contains a cartilaginous cap >1 cm in height or if there is associated pain, it is thought to be a higher risk for the lesion representing a chondrosarcoma [7]. Symptoms are usually related to the size and location of the osteochondroma.
Radiologically, osteochondromas are seen as sessile or pedunculated lesions that flare out from the bone surface with cortical continuity of their stalk [5]. Symptomatic osteochondromas can be treated with extraperiosteal excision. The neoplastic cartilage cap should be removed completely to avoid recurrence. The recurrence rate is lower in older patients who have a “burned out” cartilage cap than in younger patients with an active cartilage cap. Patients with multiple osteochondromas are usually kept under surveillance. Risk factors for malignant transformation are multiple exostosis, sessile osteochondroma, proximally located osteochondroma (pelvis, scapula, and proximal humerus). These cases are kept under surveillance [8].
Case Report
We presented with an unusual manifestation of osteochondroma. A 26-year-old male patient who was referred to our hospital due to swelling and pain of the right elbow joint. His swelling started three years back, initially the size was like a peanut that slowly progressed to the present size of a lemon. Initially swelling was not associated with pain, but he developed pain six months back which was insidious in onset. Otherwise patient history is not significant.
Local examination
On inspection: A solitary bony irregular mass of about 3×3 cm located on the lateral aspect of the upper forearm, with no skin changes (Figure 1).
On palpation: It was a non-tender, bony hard, moving with the rotation of the forearm which indicated it being arising from radius, non-reducible, non-compressible, and fixed to the underlying bone.
Movements: Terminal flexion of right elbow joint was restricted, rotation of right forearm was painful but not restricted.
Peripheral nerve examination: No posterior interosseous nerve involvement found.
At the end of the examination, we found the following conditions as our differential diagnosis:
- Dislocation of radial head
- Old malunited fracture of lateral condyle humerus
- Osteochondroma of radial neck
- Myositis ossificans
Radiographic study
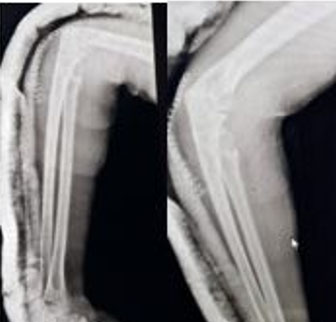
On anteroposterior and lateral view X-ray, there was a large bony excrescence originating from the radial neck and was extended toward the elbow joint. The lesion appeared to be mostly hyperdense, containing hypodense. No signs of fracture or dislocation could be seen (Figure 2).
Computed tomography of right elbow
Lesion arising from the anterior cortex of the neck of the radius, measuring about 4.2×3.7 cm, which was projecting toward the anterolateral aspect of the elbow But not involving with humero-radial, humero-ulnar, and proximal radio-ulnar articulation (Figure 3).
MRI was not done due to unavailability of MRI facility in our center
Nerve conduction study showed
Axonopathy of right radial nerve was with reduced conduction velocity.
Management
After doing thorough preoperative evaluation, the patient was taken up for surgery under Brachial block, extraperiosteal excision was done using Kocher’s approach. Intraoperative and postoperative period was uneventful. Confirmatory Postoperative Radiograph was taken (Figure 4).



Discussion
Clinical features of osteochondroma include a nontender, painless, slowly growing mass. It usually occurs in the age group of 10–20 years with no known sex predilection.
In our case presentation, the patient was “older” and symptomatic. The clinical presentation of this case of osteochondroma is rather unusual as the diagnosis was made based on the presenting complaint being swelling associated with "pain." Most common sites are knee, shoulder, elbow, wrist, scapula, ankle, ilium, lateral and medial ends of clavicle [1]. Whereas in this case the site is “Radial Neck” which is a very rare site for osteochondroma. There have been only 4 cases of osteochondroma of radial neck which have been published so far, one of which was associated with dislocation of the radial head [5].
Radiographic findings include cartilage capped bone outgrowth arising from the external surface of a long tubular bone that may be pedunculated or sessile. There can be two types of osteochondroma: One being sessile type with a broad-based attachment to the cortex and pedunculated type, with a long and thin stalk with bulbous tip. Multiple lesions are called as diaphyseal achalasia [9]. Cartilage cap can also be calcified. We should always look for stippled calcification as it is highly associated with malignant transformation.
In general, lesions point away from the nearby joint and toward the diaphysis. In our case, the lesion is sessile type, growing away from the elbow joint.
On computed tomography (CT) scan, as a characteristic finding, the cortical and medullary portions of the lesion are continuous with those of the host bone. Complications associated with osteochondroma are:
- Mechanical block to the movements of the joint
- Neurovascular compression—compression to nerve leading to neuropathy, axonopathy, and compression to vessels leading to pseudoaneurysm
- Growth disturbance leading to angular deformity and cosmetic deformity
- Fracture of the pedunculated stalk
- Bursitis
- Malignancy, most common malignancy is chondrosarcoma and rarely osteosarcoma. The frequency of malignant degeneration is approximately 1% for solitary type and 5–25% for hereditary multiple exostoses.
Conclusion
Osteochondromas are very commonly presenting benign tumors, but in common sites. We report this case due to its unusual site of presentation. These tumors are usually asymptomatic, whereas our case presented with pain and restriction of terminal range of flexion at elbow. Age of presentation is also more than the usual age of presentation. So we would like to conclude the study stating that osteochondromas though are uncommon in a lot of sites, but can still manifest in any site.
REFERENCES
1.
Casstevens C, Hubbard J, Abrams R. Impinging exostoses of the proximal radius: A report of two cases with distinct clinical features. JSES Reviews, Reports, and Techniques 2021;1(2):141–44.

2.
Shahid O, Shahid M, Shaik L, Masud M, Ranjha S. Rare case of osteochondroma on the dorsal aspect of the scapula. Cureus 2021;13(8):e17051. [CrossRef]
[Pubmed]
3.
Javdan M, Hekmatnia A, Ghazavi A, et al. A case report of osteochondroma with unusual clinical and imaging presentation. Adv Biomed Res 2015;4:2. [CrossRef]
[Pubmed]
4.
Heck KR Jr. Benign bone tumours and neoplastic conditions simulating bone tumours. In: Canale ST, Beaty JH, editors. Campbell's Operative Orthopaedics. 11ed. Philadelphia, PA: Mobsy Elsevier; 2007. p. 858–61.
5.
Oljaca A, Hirzberger D, Bergovec M, et al. Osteochondroma of the scapula associated with a subclavian artery pseudoaneurysm: Case report. SAGE Open Med Case Rep 2019;10;7:2050313X18823089. [CrossRef]
[Pubmed]
6.
Ratra R, Peshin C. Rare presentation of benign osteochondroma: A case report. J Orthop Case Rep 2020;9(6):82–5. [CrossRef]
[Pubmed]
7.
Salgia A, Biswas SK, Agarwal T, Sanghi S. A rare case presentaion of osteochondroma of scapula. Med J DY Patil Univ 2013;6(3):338–41. [CrossRef]
8.
Berber O, Dawson-Bowling S, Jalgaonkar A, et al. Bizarre parosteal osteochondromatous proliferation of bone: Clinical management of a series of 22 cases. J Bone Joint Surg Br 2011;93(8):1118–21. [CrossRef]
[Pubmed]
9.
Tepelenis K, Papathanakos G, Kitsouli A, et al. Osteochondromas: An updated review of epidemiology, pathogenesis, clinical presentation, radiological features and treatment Options. In Vivo 2021;35(2):681–91. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
SK Venkatesh Gupta - Conception of the work, Design of the work, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Navya Raj - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2023 SK Venkatesh Gupta et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}