 |
Case Report
Rarer adverse effect of clozapine
1 Resident, Department of General Medicine, Dr. Ram Manohar Lohia Hospital, New Delhi, India
2 Professor, Department of General Medicine, Dr. Ram Manohar Lohia Hospital, New Delhi, India
Address correspondence to:
MB Indu
Resident, Department of General Medicine, Dr. Ram Manohar Lohia Hospital, New Delhi,
India
Message to Corresponding Author
Article ID: 101315Z01MI2022
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Indu MB, Saini R, Sharma B. Rarer adverse effect of clozapine. Int J Case Rep Images 2022;13(1):24–27.ABSTRACT
Introduction: Clozapine is an atypical anti-psychotic drug widely used in the treatment of schizophrenia. It reduces suicidal ideations in schizophrenics and hence the mortality. Agranulocytosis is one among the most known serious complication of this drug. However, it can also cause life-threatening complications like necrotizing enterocolitis.
Case Report: We report a case of a 31-year-old male with past history of schizophrenia and seizure disorder on 300 mg clozapine and phenytoin 300 mg daily for 10 years. He was admitted for the evaluation of altered sensorium. Blood routine investigations and radioimaging were normal. Electroencephalogram (EEG) showed non-convulsive status epilepticus which was managed with anti-epileptic drugs. His sensorium did not improve. He started to develop fever and loose stools, later developed abdominal distension and pain. On evaluation it was found to have ischemic colitis with secondary bacterial peritonitis. Clozapine was stopped, managed conservatively. The patient recovered completely.
Conclusion: Clozapine can cause seizures. The anti-cholinergic effect of this drug can induce focal intestinal necrosis, which when unrecognized progress to transmural ischemia and perforation. Such cases need surgical intervention and is associated with high mortality. A high index of suspicion for early diagnosis, prompt correction of risk factors and early intervention prevents mortality.
Keywords: Clozapine, Ischemic colitis, Non-convulsive seizures
Introduction
Clozapine is the first atypical anti-psychotic drug and the only one approved by the Food and Drug Administration (FDA) for suicidal tendencies in schizophrenia. Ever since its discovery, it was widely used due to lower risks of extra pyramidal side effects and reduced suicidal tendencies. Alarming cases of agranulocytosis were widely documented with its use and hence this drug is reserved for drug resistant schizophrenia. The more common side effects are weight gain, hyperglycemia, tachycardia, seizures, neuroleptic malignant syndrome, etc. [1]. It can also cause life-threatening complications like agranulocytosis, cardiomyopathies, and gastrointestinal complications [2]. A high index of suspicion is the key to identify such complications.
Case Report
A 31-year-old male with previous history of schizophrenia and seizure disorder (on Clozapine 300 mg and Phenytoin 300 mg daily) presented with altered sensorium to an outside hospital and was managed as a case of encephalitis with acyclovir and ceftriaxone for 10 days. The patient did not improve despite treatment and hence was referred to our hospital. On examination at presentation to our hospital, his vitals were stable. Glasgow coma score (GCS)was E2V2M4. There were no signs of meningeal irritation and focal neurological deficits. Blood routine investigations, cerebrospinal fluid (CSF) studies, and imaging studies were normal. Herpes Simplex virus (HSV) and Japanese Encephalitis (JE) serologies were negative.
During the hospital stay, there were occasions of aggressive behavior from him which were managed with physical constrainment and anti-psychotics like haloperidol. Electroencephalogram (EEG) showed generalized epileptiform discharges predominantly in the frontocentral leads (Clozapine is known to cause non-convulsive status epilepticus, the mechanism which is not known. Treatment includes addition of anti-epileptic like sodium valproate and in refractory cases, clozapine is withdrawn and a second anti-psychotic is added). Considering a possibility of catatonic schizophrenia, clozapine was continued and sodium valproate was added. But, his sensorium continued to be the same.
On day 3, he started to have fever and loose stools. Blood routine investigations were normal. Total leukocyte count was 11,000/mm3. Serum procalcitonin, stool for Clostridium difficile toxin were negative. Blood culture was sterile.
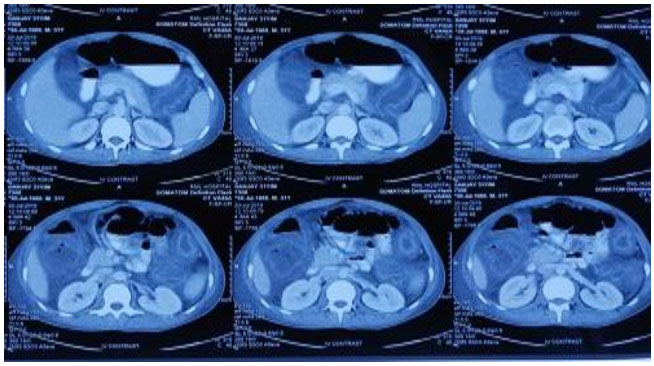
Two days later, he developed abdominal distension and on examination had guarding. Bowel sounds were sluggish. Repeat hemogram showed total leucocyte count of 30,000/mm3 with 88% polymorphonuclear cells. X-ray abdomen had no multiple air fluid levels (Figure 1 and Figure 2). Ultrasonography (USG) abdomen showed ascites and dilated bowel loops with loss of gut signature. Ascitic fluid showed more than 1000 cells/mm3 with 95% polymorphonuclear cells, sugar 119 mg, protein 2.81 g/dL, lactate dehydrogenase (LDH) 633 mg/dL, and serum ascites albumin gradient (SAAG) 0.46 suggestive of secondary bacterial peritonitis. Ascitic fluid culture was sent. Contrast-enhanced computed tomography (CECT) abdomen showed large bowel edema with small bowel dilatation suggestive of diffuse ischemic colitis (Figure 3).
Surgery consultation done, advised for conservative management. Literature review showed cases of clozapine induced necrotizing colitis.
Clozapine was stopped. Stool for occult blood was negative. The patient was kept nil per orally, antibiotics upgraded and other supportive care was given. He improved, fever, loose stools, abdominal pain, and distension subsided and gained consciousness. Repeat hemogram on day 7 was normal. He was then discharged.


Discussion
Clozapine acts as an antagonist to dopamine, serotonin, and muscarinic receptors [3]. Clozapine-induced gastrointestinal effects are believed to be due to its anti-cholinergic effects [4]. Intestinal necrosis is a partial or total necrosis of small or large bowel with mucosal starting point and consecutively transmural progression. The current pathophysiology of necrotizing enterocolitis is attributed to the following mechanisms:
- Small intestinal obstruction and increased intraluminal pressure can reduce intestinal perfusion by compressing the mucosal vessels. This leads to bowel ischemia. The risk of colonic perforation is high if the bowel diameter exceeds 12 cm and this increases mortality to 50% [5].
- Hypomotility and fecal stasis leading to luminal bacterial translocation that triggers an inflammatory response.
Aspiration of fecal vomitus can also prove fatal. The dose and duration of treatment with clozapine-induced necrotizing enterocolitis varied between 400 to 750 mg/day and 36 days to 23 years respectively [6].
Concurrent administration of other medication with anticholinergic effects can exacerbate this. The other risk factors for gastrointestinal complications associated with clozapine include HIV coinfection, obesity, other gastrointestinal infections and metabolic disorders (hypokalemia). Our patient had received haloperidol injections during his hospital stay. The additive anti-cholinergic effect of the anti-psychotics has caused the imbalance in autonomic regulation and led to bowel ischemia. The altered sensitivity to pain in schizophrenic patient can also be responsible for the delay in diagnosis and treatment, further contributing to the mortality.
Patients with bowel necrosis were at higher mortality than those with ischemic colitis [7]. Initial clinical features (within first 24 hours of onset) may be non-specific—abdominal pain, vomiting, and diarrhea. Some had constipation. This if neglected can lead to perforation peritonitis, frank bowel necrosis leading to septic shock [8].
Laparotomy in most of the reported cases showed grossly dilated bowel and at autopsy revealed intestinal necrosis [6]. Cases of ischemic colitis if recognized early can be managed conservatively but laparotomy and bowel resection is required in bowel necrosis [8].
Conclusion
Clozapine reduces mortality by reduction in suicidal tendencies in schizophrenia. But, it can also cause life-threatening adverse effects. A high index of clinical suspicion to recognize such events at the earliest is the key to reduce mortality associated with these. Regular follow-up, frequent blood investigations, and adequate addressal of complaints help in these.
REFERENCES
1.
Iqbal E, Govind R, Romero A, et al. The side effect profile of Clozapine in real world data of three large mental health hospitals. PLoS One 2020;15(12):e0243437. [CrossRef]
[Pubmed]

2.
Yu SC, Chen HK, Lee SM. Rapid development of fatal bowel infarction within 1 week after clozapine treatment: A case report. Gen Hosp Psychiatry 2013;35(6):679.e5–6. [CrossRef]
[Pubmed]
3.
Ijaz S, Bolea B, Davies S, et al. Antipsychotic polypharmacy and metabolic syndrome in schizophrenia: A review of systemic reviews. BMC Psychiatry 2018:18(1):275. [CrossRef]
[Pubmed]
4.
Palmer SE, McLean RM, Ellis PM, Harrison- Woolrych M. Life-threatening clozapine-induced gastrointestinal hypomotility: An analysis of 102 cases. J Clin Psychiatry 2008;69(5):759–68. [CrossRef]
[Pubmed]
5.
Guégan H, Carles J, Loze S, Janvier G, Junès F, Videau J. Acute necrotising enterocolitis in adults. Analysis of a homogeneous series of 12 cases. Review of the literature. [Article in French]. J Chir (Paris) 1992;129(4):191–7.
[Pubmed]
6.
Razak NA, Mohd Nor F, Shafie MS, Hwang IS. Clozapine induced fatal bowel ischemia – A neglected side effect? MJP Online Early 2017.
7.
Peyrière H, Roux C, Ferard C, et al. Antipsychotics-induced ischemic colitis and gastrointestinal necrosis: A review of the French pharmacovigilance database. Pharmacoepidemiol Drug Saf 2009;18(10):948–55. [CrossRef]
[Pubmed]
8.
Palladino E, Ormando V, Fusco L. Clozapine induced ischemic colitis and gastrointestinal necrosis requiring surgical treatment: A mini review. imedPub Journals 2016;4(1):41.
SUPPORTING INFORMATION
Author Contributions
MB Indu - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Rohit Saini - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Brijesh Sharma - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2022 MB Indu et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}