 |
Case Report
Hyperthrophy of the pituitary stem and insipid diabetes about a case
1 MD, Resident in Radiology, CHU Ibn Sina, Rabat, Morocco
2 MD, Radiology Resident, Ibn Sina University Hospital, Rabat, Morocco
3 MD, Endocrinology Resident, Ibn Sina University Hospital, Rabat, Morocco
4 MD, Specialist in Radiology, CHU Ibn Sina, Rabat, Morocco
5 Professor in Diagnostic and Interventional Imaging, Head of Central Radiology Department, Ibn Sina Rabat University Hospital, Rabat, Morocco
6 Professor in Diagnostic and Interventional Imaging, Department of Central Radiology, Ibn Sina Rabat University Hospital, Rabat, Morocco
Address correspondence to:
Rita Oze Koudouhonon
10 rue Oulad El Bouziri Mabella, Rabat door A4 on the 4th floor,
Morocco
Message to Corresponding Author
Article ID: 101280Z01RK2022
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Koudouhonon RO, Igombe SRA, Wilson B, Ahmed A, Elhosni KB, Nassar I, Billal NM. Hyperthrophy of the pituitary stem and insipid diabetes about a case. Int J Case Rep Images 2022;13:101280Z01RK2022.ABSTRACT
The involvement of the pituitary stem frequently encountered since the development of pituitary imaging is revealed by diabetes insipidus in the majority of cases. The pituitary stem can be the target of various pathologies, infectious, infiltrative, and tumor. In cases where the etiological investigation is negative, genetic abnormalities may be incriminated. Through our case we show the variability of conditions that can reach the pituitary stem as well as the role of imaging in the etiological investigation to arrive at hypotheses requiring confirmation at histology or close monitoring of lesions.
Keywords: Diabetes insipidus, MRI, Pituitary stem hyperthrophy
Introduction
The pituitary stem is a median organ normally measuring between 1 and 1.5 mm thick. It is said to be thickened when its diameter varies between 2.5 and 3 mm [1]. This anomaly, increasingly encountered on pituitary magnetic resonance imaging (MRI) since its development, is found in various pathologies including diabetes insipidus which is an inaugural sign, inflammatory, infectious, infiltrative, or tumor pathologies. The etiological diagnosis being uncertain, monitoring of lesions or histological evidence, is necessary to determine with certainty the cause [2],[3].
Case Report
We report the case of a 49-year-old patient. Mother of two children, widow without past history (ATCD), in whom the sudden installation of polyuria and polydipsia dating back about 26 months, required a consultation in endocrinology where she was hospitalized.
The clinical examination found an obese patient with a body mass index (BMI) of 41 kg/m2, normal cardiovascular examination with blood pressure (BP) at 130/80, heart rate (FC) at 108 bpm, and electrocardiogram (ECG) without particularity. She had a severe polyuro-polydipsic syndrome with urination greater than 8 liters (L) estimated at 10 L/day (d) and 6 nocturnal awakenings. During hospitalization, she benefited from a 6 hors water restriction test, with the realization of a urinary ionogram which made it possible to highlight a urinary osmolarity of less than 700 mosm/L. A therapeutic test (anti-diuretic hormone = DHA), Minirin 120 ug spray 1×/d for 72 hours improved her syndrome, with a regression of urination (3 L/d and a night awakening).
An etiological survey was carried out. The examination of the pituitary axes, including the determination of thyrotropic hormones (TRH=Thyrotripin-liberin=thyrotripin-releasing hormone, TSH = TSH=thyroid-stimulating hormone, T3, T4, and gonadotropic hormones (FSH=follicle-stimulating hormone, LH=luteinizing hormone was without abnormality.
Biologically, there was hypochromic microcytic anemia with a complete blood count (SN) a hemoglobin level of 5.9 g/100 mL per hematocrit at 23%, the mean blood cell volume (GMV) at 59.7 u3.
The positive inflammatory balance with a sedimentation rate (VS) accelerated to (1 hour = 58 mn; 2 hour = 100 mn), the reactive protein C (CRP) increased to 14.23 mg/L.
Biochemistry returned to normal blood sugar at 0.91, hemoglobin glycated (HbA1C) normal at 5.1, ferritin 6.18 ng/mL.
The search for Koch's bacillus (BK) in the sputum had returned to normal.
Cytobacteriological examination and urinary biochemistry were normal. Histological examination of the biopsy fragment of the salivary gland showed a discrete chronic non-specific sialadenitis without amyloid and granuloma deposition.
The radiological assessment on abdominal and transthoracic ultrasound found no abnormalities. X-ray of long bones was normal. The chest X-ray found an interstitial syndrome with mediastinal lymphadenopathy.
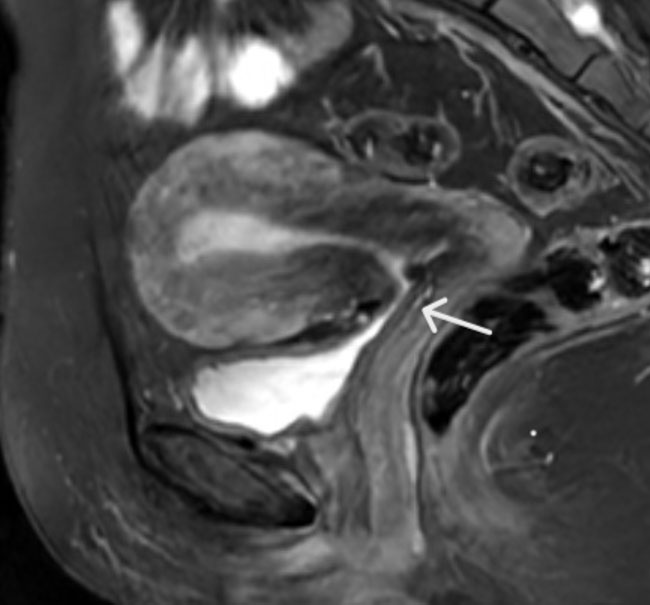
A pituitary magnetic resonance imaging (MRI) performed found a thickened pituitary rod measuring 3 mm without interruption syndrome (Figure 1).

Discussion
Imaging is essential in the etiological assessment of a large pituitary stem discovered during diabetes insipidus. Various pathologies among other inflammatory, infectious, infiltrative, or tumorous can be discussed in adults with a higher frequency for inflammatory or granulomatous diseases.
Sarcoidosis in the first line was evoked in our patient, in front of inflammatory biological signs, and pulmonary involvement with mediastinal lymphadenopathy. The absence of epithelioid granuloma in salivary gland biopsy (BGSA) on histological examination, allowed us to eliminate it.
Erdheim-Chester disease and hystiocytosis were also evoked in front of pulmonary signs, but eliminated in front of the absence of bone lesions on X-ray of long bones. A tuberculous origin has been evoked in front of the pulmonary signs, but refuted with the absence of BK in the sputum.
Faced with the absence of bundles of arguments eliminating the aforementioned etiologies, the diagnosis adopted in our patient is lymphocytic pituitary gland (HL) [1].
Lymphocytic pituitary gland (HL) is an autoimmune endocrinopathy of relatively recent individualization, since its first description nearly 40 years ago. It is an essentially female autoimmune pathology that most often reveals itself during pregnancy and the immediate postpartum. It can also occur years later. According to the literature, this still poorly known pathogenesis is related to lymphocytic infiltration of the pituitary gland. Hormonal deficiencies are common (65%), including ACTH (adrenocorticotrophic hormone) deficiency. In common practice, the determination of anterior pituitary antibodies is not useful for diagnosis, given their low sensitivities, since in 25% of cases associated with other autoimmune diseases [1],[4].
Anyway, the difficulty in asserting with certainty this etiology without histological proof (biopsy-neurosurgical excision), due to the slow evolution of certain pathologies delaying their clinical manifestation [1],[4].
The patient was finally put on replacement therapy, in order to lower the polyuro-polydipsic syndrome and limit nocturnal awakenings; Minirin 60 ug in spray 2×/d. This made it possible to improve her quality of life with the regression of his symptomatology. However, regular monitoring of lesions by pituitary MRI is required.
Conclusion
The discovery of a large pituitary stem on pituitary MRI, in the context of diabetes insipidus, raises a wide diagnostic range that must be guided by clinical and biological data.
REFERENCES
1.
Chanson P. Pathology of the pituitary stalk and diabetes insipidis. [Article in French]. Ann Endocrinol (Paris) 2005;66(1):50–4. [CrossRef]
[Pubmed]

2.
Trabelsi L, Mnif M, Rekik N, et al. MRI pituitary stalk abnormalities: Etiology aspects in 11 patients. [Article in French]. Ann Endocrinol (Paris) 2006;67(6):604–12. [CrossRef]
[Pubmed]
3.
Mnif F, Graja S, Rekik N, et al. Épaississement de la tige pituitaire: Aspects étiologiques et évolutifs à propos de 14 cas. Annales d'Endocrinologie 2012;73(4):297. [CrossRef]
4.
Salenave S, Chanson P, Young J. Hypophysite lymphocytaire. EMC - Endocrinologie - Nutrition 2007;4(2):1–7. [CrossRef]
SUPPORTING INFORMATION
Author Contributions
Rita Oze Koudouhonon - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Suzanne Rita Aubin Igombe - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Bizimana Wilson - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Aicha Ahmed - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Khadija Ben Elhosni - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Ittimade Nassar - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Nabil Moatassim Billal - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2022 Rita Oze Koudouhonon et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}