 |
Case Report
Bilateral carotid paraganglioma: A case report
1 Neurosurgery Clinic, Fann Teaching Hospital, Dakar, Senegal
2 Cardiology Department, Kamenge Teaching Hospital, Bujumbura, Burundi
3 Medical Imaging Department, Kamenge Teaching Hospital, Bujumbura, Burundi
4 Saint Joseph Cardiology Clinic, Burundian Society of Cardiology, Burundi
5 Neurology Department, Kamenge Teaching Hospital, Bujumbura, Burundi
Address correspondence to:
Jean Michel Nzisabira
Neurosurgery Department, Fann University Hospital, Dakar,
Senegal
Message to Corresponding Author
Article ID: 101268Z01JN2021
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Nzisabira JM, Ndirahisha E, Manirakiza S, Nzisabira LS, Barasukana P, Nzisabira L. Bilateral carotid paraganglioma: A case report. Int J Case Rep Images 2021;12:101268Z01JN2021.ABSTRACT
Introduction: Paragangliomas are rare tumors derived from the neural crest. The carotid location is the most common in the neck.
Case Report: We report the case of a 17-year-old Burundian girl who presented with a bilateral laterocervical mass syndrome evolving for several years. The interrogation reveals a case of laterocervical swellings of very slow evolution without any other clinical manifestation. The diagnosis was made by nuclear magnetic resonance imaging and angiography.
Conclusion: The young age of the patient, the bilateral location of the tumors in the carotid artery, and the family history suggest a hereditary etiology.
Keywords: Age, Bilaterality, Carotid location, Paraganglioma, SDH gene
Introduction
Paragangliomas are tumors of the autonomic nervous system that develop from the paraganglia. Paraganglia are cells derived from the neural crest. They are rare tumors. The incidence is estimated at 1/300,000 per year, paragangliomas and pheochromocytomas combined and whatever their location (Lefebvre 2014) [1]. Although the evolution of paragangliomas is very slow and uncertain, signs of severity can be present very early on. It is important to know how to look for them and to recognize them because their presence leads to specific diagnostic and therapeutic measures. Our aim is to look for these signs in this case and then compare them with those of the most recent publications.
Case Report
This case concerns a 17-year-old girl, student, without any particular history, referred to the medical imaging department for exploration of two laterocervical masses.
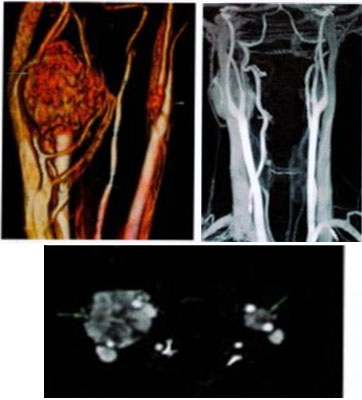
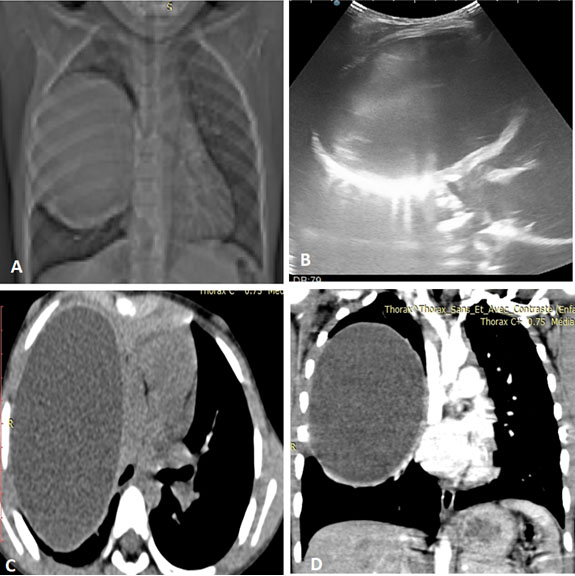
These masses became clinically apparent about three years before the radiological exploration. The family history revealed a cervical mass syndrome in a 27-year-old brother and hypertension in a 26-year-old sister. Examination revealed a hyperpigmented spot of several centimeters on the right forearm. Cervical magnetic resonance imaging showed two well-demarcated tissue masses located at the level of the two carotid bifurcations. The two masses measured respectively: 3.5 (L) × 2.7 (W) × 2.6 (AP) cm on the right and 1.5 (L) × 1.3 (W) × 1.2 (AP) cm on the left. In T1 sequence they appeared iso-signal and in T2 sequence they appeared hypersignal with intense enhancement. Punchy areas in hyposignal appear on T2 giving the “salt and pepper” appearance, suggestive of paraganglioma. Carotid angiography showed tissue masses with intense enhancement at the level of the carotid bifurcations and spreading the two carotids. The right tissue mass surrounded the internal carotid artery by more than 1800. On the left, the internal carotid artery was not surrounded.
Discussion
This is the first case reported in Burundi. The first serious element is the rarity of the disease. We found very few published cases in Africa. The only publications we could find were from Morocco (Soumia 2021) [2], South Africa (Cassandra Bruce-Brand 2021) [3], and Egypt (Zainine Rim Besbes 2015) [4]. The early age of onset of the disease was the second most important factor in our patient's case. In a review published in 2017, Lenders states that young age and tumor size, the third sign of severity, predispose to a high risk of metastasis and recurrence [5]. The dimensions of the patient's two cervical masses are very large compared to the size of a normal carotid corpuscle, which varies between 3 and 5 mm (Figure 1 and Figure 2). Karren (2020) estimates the potential for carotid paragangliomas to progress to malignancy to be around 10% [6]. Bilaterality is the fourth sign of severity. The fifth element we encounter in the girl is the family history. One of the brothers has a cervical mass of the same topography, painless, asymptomatic, and evolving for several years. This mass would have appeared even before that of his sister. An older sister has episodes of hypertension although she is currently only 26 years old.
The family history, the young age of the patient, the bilaterality, and the location are elements that plead in favor of a hereditary etiology (Garcia-Carbonero 2021) [7],[8]. It is currently recognized that paragangliomas/phaeochromocytomas of genetic origin account for 30–33% of cases of carotid paragangliomas, which may be bilateral in 5% of cases and multiple in 80% of cases. Familial cases are due to mutations in the subunits of the succinate dehydrogenases gene: SDHB, SDHC, and SDHD (Amr Gad 2014) [9]. The transmission is autosomal dominant, i.e., there is a 50% chance that a child will inherit the mutation from a parent. People carrying a maternal gene mutation are in the vast majority of cases healthy, whereas those who inherit the paternal gene mutation are usually ill. The penetrance of the gene transmission depends on the gene, age, and tumor location. Genetic diagnosis is very important for the screening and follow-up of patients and their relatives. Indeed, it is now recognized that the presence of a constitutional mutation in the SDHB gene of a paraganglioma carrier is an important risk factor for malignancy (38%) and poor prognosis (Amr Gad 2014) [9]. These mutated SDHB tumors are mainly located in the thoraco-abdomino-pelvic region. They can take the familial or multiple forms, but they are less frequent (22% for familial forms vs. 21% for multiple forms), in contrast to mutated SDHD paragangliomas, where familial expression of the disease and multiple forms are more frequent, respectively 59% and 67% (Guo 2015) [10].

Conclusion
The patient needs to complete her work-up as far as possible with genetic, biochemical, immunohistochemical, and imaging tests to ensure optimal management.
REFERENCES
1.
Lefebvre M, Foulkes WD. Pheochromocytome and paraganglioma syndrome: Genetics and management update. Curr Oncol 2014;21(1):e8–17. [CrossRef]
[Pubmed]

2.
Berrad S, Erraichi H, Oualla K, et al. Paraglanglioma of the carotid glomus. Am J Biomed Sci & Res 2021;12(4):AJBSR.MS.001771. [CrossRef]
3.
Bruce-Brand C, van Wyk AC. Prevalence of succinate dehydrogenase deficiency in paragangliomas and phaeochromocytomas at a tertiary hospital in Cape Town: A retrospective review. Journal of Endocrinology, Metabolism and Diabetes of South Africa 2021;26(1):9–15. [CrossRef]
4.
Rim Z, Rim B, Houda C, Souheil J, Najeh B, Ghazi B. Paraganglioma of the carotid body: Report of 26 patients and review of literature. Egyptian Journal of Ear, Nose, Throat and Allied Sciences 2015;16(1):19–23. [CrossRef]
5.
Lenders JWM, Eisenhofer G. Update on modern management of pheochromocytoma and paraganglioma. Endocrinol Metab (Seoul) 2017;32(2):152–61. [CrossRef]
[Pubmed]
6.
Antonio K, Valdez MMN, Marcado-Asis L, Taïeb D, Pacak K. Pheochromocytoma/paraganglioma: Recent updates in genetics, biochemistry, immunohistochemistry, metabolomics, imaging and therapeutic options. Gland Surg 2020;9(1):105–23. [CrossRef]
[Pubmed]
7.
Garcia-Carbonero R, Matute Teresa F, Mercader-Cidoncha E, et al. Multidisciplinary practice guidelines for the diagnosis, genetic counseling and treatment of pheochromocytomas and paragangliomas. Clin Transl Oncol 2021;23(10):1995–2019. [CrossRef]
[Pubmed]
8.
Lenders JWN, Duh Y, Eisenhofer G, et al. Pheochromocytoma and paraganglioma: An endocrine society clinical practice guideline. J Clin Endocrinol Metab 2014;99(6):1915–42. [CrossRef]
[Pubmed]
9.
Gad A, Sayed A, Elwan H, et al. Carotid body tumors: A review of 25 years. Experience in diagnosis and management of 57 tumors. Ann Vasc Dis 2014;7(3):292–9. [CrossRef]
[Pubmed]
10.
Zhenying G, Lloyd RV. Pheochromocytomas and paraganglioma: An update on recent molecular genetic advances and criteria for malignancy. Adv Anat Pathol 2015;22(5):283–93. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Jean Michel Nzisabira - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Eugène Ndirahisha - Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Sébastien Manirakiza - Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Linda Samantha Nzisabira - Acquisition of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Patrice Barasukana - Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Léopold Nzisabira - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2021 Jean Michel Nzisabira et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}