 |
Clinical Image
Lung bronchogenic cyst in children
1 MD, Radiology Department, Ibn Sina Paediatric Teaching Hospital, Mohammed V University, Rabat, Morocco
2 MD, Professor, Radiology Department, Ibn Sina Paediatric Teaching Hospital, Mohammed V University, Rabat, Morocco
Address correspondence to:
Romeo Thierry Yehouenou Tessi
MD, Radiology Department, Ibn Sina Paediatric Teaching Hospital, Mohammed V University, BP 6527, Rabat,
Morocco
Message to Corresponding Author
Article ID: 101266Z01RT2021
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Yehouenou Tessi RT, El Haddad S, Oze KR, Allali N, Chat L. Lung bronchogenic cyst in children. Int J Case Rep Images 2021;12:101266Z01RT2021.ABSTRACT
No Abstract
Keywords: Bronchogenic, Child, CT scan, Cyst, Lung
Case Report
This is a case of a 5-year-old child with cough and fever who was treated for recurrent lung infections.
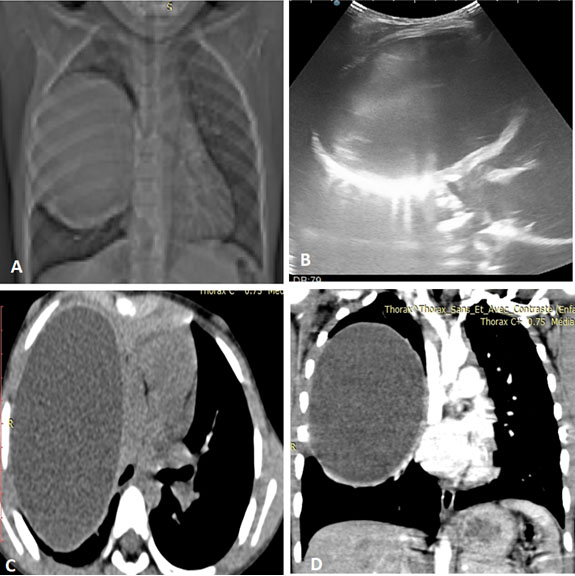
The symptoms had been evolving for about one year. A chest X-ray was performed to show a rounded opacity in the right lung with a watery tone (Figure 1A, topogram).
A thoracic computed tomography (CT) scan was ordered to better characterize this right pulmonary opacity. The thoracic CT scan showed a right intrapulmonary formation with a mass effect on the lower lobe of well-bounded, thin-walled, rounded cystic density, unenhanced after injection of iodinated contrast medium. It remains in intimate contact with the upper and middle lobar branches. It exerts a mass effect on the right lower lobe (Figure 1C, Figure 1D).
Additional thoracic ultrasound reveals a pure anechoic right lung formation, thin-walled with posterior reinforcement, not vascularized on color Doppler (Figure 1B).
In view of this picture, the diagnosis of bronchogenic cyst of intra-parenchymal location was evoked.
She underwent en bloc resection of the cystic lesion with histological confirmation of the diagnosis of bronchogenic cyst.
Discussion
Bronchogenic cyst is a rare benign congenital malformation of the tracheobronchial tree occurring during embryonic development [1].
It consists of a thin-walled cystic formation of bronchial type and variable content of variable topography often integral with the tracheobronchial axis:
- Mediastinal (75%)
- Intra-parenchymal lung (15–23%)
- Ectopic
According to Maier's classification, four mediastinal locations are distinguished: para-tracheal, carinal, hilar, paraesophageal [2].
The clinical signs of discovery vary. It can be asymptomatic, with recurrent lung infections, signs of compression (dyspnea, cough, stridor, dysphagia, and respiratory distress).
In children, infectious phenomena are in the foreground. Asymptomatic forms represent 20–30% [3].
The contribution of imaging is considerable, not only to approach the diagnosis but also to carry out a pre-therapeutic assessment.
The CT scan is the gold standard, confirming the fluid nature of the mass, its density, its topography and its relationships. The density of the cyst ranges from 0 to 20 Hounsfield units (HU), but can reach 120 HU due to its high protein content. It is well delineated, often unilocular but may have a multi-location. There is no contrast enhancement. The wall may be thick and calcified [4].
It appears on CT as a cystic mass of homogeneous fluid density, a well-limited cystic mass of homogeneous or high fluid density (mucoid content) with a thin wall that is sometimes calcified without contrast.
Anatomically, an intra-pulmonary bronchogenic cyst is unilocular and filled with mucus [1]. It can sometimes be complicated by superinfection.
The differential diagnosis is made with other bronchopulmonary malformations, namely [3]:
- Adenomatoid cystic pulmonary malformation: 25% of bronchopulmonary masses, the most frequently diagnosed in antenatal period. It is due to adenomatoid proliferation of the terminal bronchioles by arrest of maturation of the bronchial tree, in the bronchioles at the glandular stage without formation of alveolar tissue. It affects males +++, is often unilateral and unilobar, in the lower lobe +++. It is usually asymptomatic. It presents a risk of superinfection or even malignant degeneration.
Computed tomography scan confirms the diagnosis in the form of a cystic mass connected to a bronchus +/−aerated content, aeric cysts connected to the bronchus, well demarcated from the rest, pulmonary hyperclarity with mediastinal discharge, sometimes hydroaeric levels.
- Giant lobar emphysema: This corresponds to alveolar distension localized to a lobe of the lung in relation to bronchial obstruction on expiration. Computed tomography scan confirms the diagnosis and specifies the topography.
The affected lobe appears hyperenlightened and hypovascularized. Treatment is surgical, consisting of a lobectomy.
- Hydatid cyst: The individualization of a wall-delimiting cyst may wrongly make the diagnosis of hydatid cyst, as well as in mixed forms with hydroaerobic content, the differential diagnosis is with complicated hydatid cysts.
Treatment is essentially surgical. Care must be taken not to open the cyst. It concerns both symptomatic and asymptomatic cysts, given the frequency of complications. Total monobloc excision is the treatment of choice. It can be performed by conventional (thoracotomy) or video thoracoscopy.
Conclusion
Bronchogenic cyst is a rare benign congenital malformation of the tracheobronchial tree, affecting mainly children. It occurs mainly in the mediastinum and accounts for 60% of mediastinal cysts and 6–15% of mediastinal masses. There are no specific clinical signs of mediastinal bronchogenic cyst. The symptomatology is due to the occurrence of complications dominated by compression and infection. Imaging (computed tomography (CT) and magnetic resonance imaging (MRI)) can suggest it, but only histological analysis confirms the diagnosis. Surgical resection is recommended for all bronchogenic cysts as the evolution is unpredictable.
REFERENCES
1.
Le HM, Validire P, Mayeur D, Seguin-Givelet A, Gossot D. Intrapulmonary bronchogenic cysts. [Article in French]. Rev Mal Respir 2016:33(7):622–5. [CrossRef]
[Pubmed]

2.
Maier LC. Bronchiogenic cysts of the mediastinum. Ann Surg 1948;127(3):476–502. [CrossRef]
[Pubmed]
3.
Bousetta K, Aloui-Kasbi N, Fitouri Z, et al. Malformations pulmonaires congénitales. Apport de l'imagerie. Journal de Pédiatrie et de Puériculture 2004:17(7):370–9. [CrossRef]
4.
Hantous-Zannad S, Charrada L, Mestiri I, et al. Radiological and clinical aspects of bronchogenic lung cysts: 4 case reports. [Article in French]. Rev Pneumol Clin 2000;56(4):249–54.
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Romeo Thierry Yehouenou Tessi - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Siham El Haddad - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Koudouhonon Rita Oze - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Nazik Allali - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Latifa Chat - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2021 Romeo Thierry Yehouenou Tessi et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}