 |
Case Report
Resection of large proportion ameloblastoma with immediate reconstruction: A case report
1 DDS, MSc, Mato Grosso Cancer Hospital and University of Cuiabá, Cuiabá, MT, Brazil
2 DDS, Department of Oral Surgery Mato Grosso Cancer Hospital, Cuiabá, MT, Brazil
3 DDS, Mato Grosso Cancer Hospital, Cuiabá, MT, Brazil
4 DDS, MSc, PhD, Mato Grosso Cancer Hospital and University of Cuiabá, Cuiabá, MT, Brazil
Address correspondence to:
Luiz Evaristo Ricci Volpato
Universidade de Cuiabá, Av. Beira Rio, 3100 - Jardim Europa, Cuiabá, MT, CEP: 78065-443,
Brazil
Message to Corresponding Author
Article ID: 101240Z01ES2021
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
da Silva EJ, Godinho V, Magalhães LRM, Volpato LER. Resection of large proportion ameloblastoma with immediate reconstruction: A case report. Int J Case Rep Images 2021;12:101240Z01ES2021.ABSTRACT
Introduction: Ameloblastoma is a benign odontogenic tumor, locally aggressive and highly prone to recurrence. Due to its clinical behavior and high recurrence rate, it is recommended that the treatment of ameloblastoma be radical, which creates a defect in bone continuity, requiring reconstruction of the osteotomized segment.
Case Report: A 26-year-old patient diagnosed with a large proportion ameloblastoma of plexiform type in the left mandible, resulting in facial asymmetry and volumetric increase in the left middle and lower thirds of the face sought treatment at Mato Grosso Cancer Hospital. The treatment consisted of resection with immediate reconstruction, using pre-contoured reconstruction plate aided by prototyping and costochondral graft.
Conclusion: The graft associated with the reconstruction plate demonstrated good adaptation to the mandibular fossa and preservation of joint function, in addition to minimizing the possible mechanical failures expected from the fixation material. The use of the 3D model to aid in the previous conformation of the plate resulted in less surgical time, adequate adaptation of the material to the bone segment, and better facial symmetry.
Keywords: Ameloblastoma, Odontogenic tumors, Oral pathology, Oral surgery, Three-dimensional printing
Introduction
Ameloblastoma is a benign, intraosseous odontogenic tumor, of epithelial origin, locally aggressive, with progressive and expansive growth [1],[2], and high tendency to relapse. Its origin is related to the enamel organ, remains of the odontogenic epithelium and coating of odontogenic cysts [1].
Its recommended treatment is marginal or segmental mandibulectomy, with the need for margins of 1 to 1.5 cm [3] which commonly leads to continuity defect in the bones, requiring mandibular reconstruction usually performed with autogenous bone graft and titanium plates [4].
This work presents a case of extensive ameloblastoma resection in the mandible with immediate reconstruction using pre-contoured reconstruction plate aided by prototyping and costochondral graft.
Case Report
A 26-year-old male patient previously diagnosed with ameloblastoma sought treatment presenting a hardened swelling in the face with an evolution of 10 years. The diagnosis had been made previously in an anatomopathological analysis service, after incisional biopsy. According to the patient, in the episodes of pain, attempts were made to decompress the lesion through puncture, resulting in temporary relief. However, some of such attempts led to hemorrhage requiring hospitalization. Due to financial limitations, it took time for him to seek specialized care.
He presented facial asymmetry with volumetric increase in the middle and lower thirds of the left face, with a hardened consistency on palpation, painless and a normal colored surface. Intraorally, in the posterior region of the left mandible, there was bulging of cortical bone and nodular lesion, with an irregular, symptomatic, fixed surface, with sessile base and presence of purulent secretion. Poor oral hygiene and the left side maxillary molars occlusion on the tumor were also noted (Figure 1).
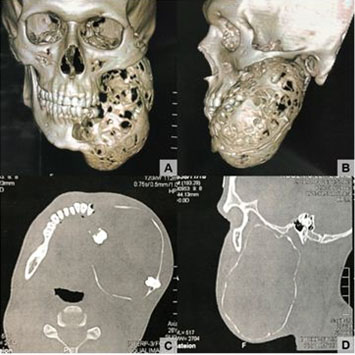
Computed tomography showed a hypodense, multilocular lesion, with bulging of cortical bone involving the left hemimandible, associated with teeth 37 and 38 (Figure 2).
A new incisional biopsy was performed in the lesion, which revealed a fragment of odontogenic lesion of epithelial origin, whose histopathological analysis consisted of plexiform and follicular parenchyma, composed of basaloid cells similar to ameloblasts. In the internal region of the lesion, a looser disposition was noted, mimicking the stellar reticulum. There was no sign of malignancy. From these findings, the diagnosis of ameloblastoma was confirmed (Figure 3).
Hemimandibulectomy with immediate reconstruction using a 2.4 mm mandibular reconstruction plate and a costochondral graft, removed from the rib, was proposed.
A 3D anatomical model generated from rapid prototyping was used for conformation prior to surgery to optimize the surgical time and improve the adaptation and fixation of the reconstruction plate (Figure 4). To reconstruct the side to be resected, the contralateral area was mirrored.
Under general anesthesia and nasotracheal intubation, lip switch with extended submandibular incision was performed for exposure and resection of the tumor. The occlusion was preserved using maxillomandibular block through locking screws and steel wire. This was followed by ostectomy in the anterior region of the mandible and resection of the tumor measuring 13 cm in its greater extension (Figure 5). The pre-conformed reconstruction plate was adapted and fixed to the mandibular remainder. The costochondral graft taken from a right rib was fixed to the plate with screws to mimic the mandibular condyle and maintain joint function (Figure 6). A vacuum suction drain was used in the immediate postoperative period to reduce the possibility of dead space formation. The patient was admitted to the intensive care unit for three days. During that time he was fed with pasty food by the oral route.
The control radiography showed good positioning of the plate and graft (Figure 7). The locking screws were maintained for elastic therapy.
After 14 days, the patient evolved with stable dental occlusion, limited mouth opening, hypomobility of the lower left lip and fistula with purulent drainage in the submental region. Irrigation was performed with 0.9% saline and culture and antibiogram tests were requested for appropriate antibiotic therapy. The patient used oral 500 mg ciprofloxaxin, 12/12 hours, for 10 days and underwent local care in the fistula region, progressing satisfactorily.
Considering the limitations of this type of reconstruction, the definitive rehabilitation planned would be through a customized temporomandibular joint prosthesis. About three and a half months after the operation, the patient informed that he would no longer attend the return visits, making the treatment unfeasible.






Discussion
A case of ameloblastoma of large proportions in a patient of atypical age group, who underwent resection with immediate reconstruction using a reconstruction plate and costochondral graft, with the aid of a 3D anatomical model was reported.
Ameloblastoma represents about 1% of all head and neck tumors and is the commonest odontogenic tumor. It is more frequent in men (1.2: 1) between 30 and 60 years of age, with a peak around the fifth decade of life, affecting in 80% of cases, the posterior mandible region [5]. In the case presented, the patient was a 26-year-old male and already with an important tumor dimension.
The recurrence rate of ameloblastoma varies according to the treatment modality: 8% after resection and 41% after enucleation and curettage. Considering the aggressive nature of the tumor and the possibility of malignization in recurrences, the treatment of choice is resection with a safety margin of 1 cm, generally requiring reconstruction [5],[6]. In this case the segmental resection of the mandible was performed with immediate reconstruction.
Titanium reconstruction plates are biocompatible, adaptable to bone surfaces, offer acceptable functional results and give stability to the mandibular segment, preventing its deviation when in function. Planning based on a 3D model includes advantages, such as a special understanding of bone morphology, accurate and previous conformation of the plate and an adequate measure of the graft to be removed, therefore, decreasing the time of surgery and, consequently, the time of exposure of the patient to general anesthesia [4],[7],[8]. In this case, the use of the pre-contoured reconstruction plate in 3D model allowed adequate adaptation and symmetry, a considerable reduction in the patient's exposure time to general anesthesia and a lower risk of infections due to prolonged wound exposure.
Since this reconstruction involved the ramus and condyle regions, it was decided to use costochondral grafts in order to maintain joint function [7],[9],[10]. As observed in the intraoperative and imaging exams, the graft was satisfactorily positioned in the mandibular fossa.
A vacuum suction drain was used to reduce the possibility of dead space formation. Suction drains are also used to reduce the formation of bruises, a factor that can predispose to infections. On the other hand, the drain can act as a source of contamination, in addition to preventing the natural tamponade that occurs when surgical wounds are only closed by sutures [11]. As noted, the use of the suction drain did not prevent the development of postoperative infection in the case.
Restoration of masticatory, speech and respiratory functions is the main objective of mandibular reconstruction, followed by preservation of dental occlusion and temporomandibular joint, possibility of dental rehabilitation and satisfactory aesthetic results, considering that facial deformities can induce great social impact and psychological repercussions [7]. Maintenance of occlusal function was observed, with joint movements and mandibular perimeter preserved, favoring facial symmetry.
The majority of ameloblastomas relapses in a period of 5–6 years, however, recurrence was observed in a period of up to 20 years, justifying prolonged preservation. Radical resection is the only independent predictive factor for reducing the chance of recurrence [12]. The patient's nonattendance at postoperative consultations was a limiting factor for the follow-up and assessment of success of this case. Although the treatment was performed by a modality with low potential for recurrence, the possibility is not ruled out.
Conclusion
Reconstruction using a fixation system and costochondral graft minimized the possible mechanical failures expected from the plate and made it possible to adapt the graft to the mandibular fossa, preserving joint function. The prototyping aid for pre-contouring the plaque enriched the treatment, favoring better facial symmetry, adequate adaptation to bone segment, and decreased transoperative time. The importance of diagnosis and treatment in the initial stages of the injury is emphasized, in order to result in less surgical morbidity and possible functional and aesthetic deficiencies.
REFERENCES
1.
Effiom OA, Ogundana OM, Akinshipo AO, Akintoye SO. Ameloblastoma: Current etiopathological concepts and management. Oral Dis 2018;24(3):307–16. [CrossRef]
[Pubmed]

2.
da Silva YS, Tartaroti NA, Sendyk DI, Deboni MCZ, Naclério-Homem MDG. Is conservative surgery a better choice for the solid/multicystic ameloblastoma than radical surgery regarding recurrence? A systematic review. Oral Maxillofac Surg 2018;22(4):349–56. [CrossRef]
[Pubmed]
3.
Neagu D, Escuder-de la Torre O, Vázquez-Mahía I, et al. Surgical management of ameloblastoma. Review of literature. J Clin Exp Dent 2019;11(1):e70–5. [CrossRef]
[Pubmed]
4.
Cohen A, Laviv A, Berman P, Nashef R, Abu-Tair J. Mandibular reconstruction using stereolithographic 3-dimensional printing modeling technology. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009;108(5):661–6. [CrossRef]
[Pubmed]
5.
Kreppel M, Zöller J. Ameloblastoma-clinical, radiological, and therapeutic findings. Oral Dis 2018;24(1–2):63–6. [CrossRef]
[Pubmed]
6.
Hendra FN, Natsir Kalla DS, Van Cann EM, de Vet HCW, Helder MN, Forouzanfar T. Radical vs conservative treatment of intraosseous ameloblastoma: Systematic review and meta-analysis. Oral Dis 2019;25(7):1683–96. [CrossRef]
[Pubmed]
7.
Paré A, Bossard A, Laure B, Weiss P, Gauthier O, Corre P. Reconstruction of segmental mandibular defects: Current procedures and perspectives. Laryngoscope Investig Otolaryngol 2019;4(6):587–96. [CrossRef]
[Pubmed]
8.
Chutchurru MS, Brusca MI, Palavecino R. Ameloblastoma: Reconstruction using titanium plates adapted using stereolithographic models. Ann Maxillofac Surg 2018;8(2):337–41. [CrossRef]
[Pubmed]
9.
Lee WY, Park YW, Kim SG. Comparison of costochondral graft and customized total joint reconstruction for treatments of temporomandibular joint replacement. Maxillofac Plast Reconstr Surg 2014;36(4):135–9. [CrossRef]
[Pubmed]
10.
Mercuri LG. Costochondral graft versus total alloplastic joint for temporomandibular joint reconstruction. Oral Maxillofac Surg Clin North Am 2018;30(3):335–42. [CrossRef]
[Pubmed]
11.
de Andrade MAP, de Oliveira Campos TV, Silva BFA, et al. Six month follow-up of patients submitted to total knee arthroplasty with and without placement of suction drainage devices. Rev Bras Ortop 2015;45(6):549–53. [CrossRef]
[Pubmed]
12.
Au SW, Li KY, Choi WS, Su YX. Risk factors for recurrence of ameloblastoma: A long-term follow-up retrospective study. Int J Oral Maxillofac Surg 2019;48(10):1300–6. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Everton José da Silva - Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Géssica Vasconcelos Godinho - Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Luís Ricardo Machado Magalhães - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Luiz Evaristo Ricci Volpato - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2021 Everton José da Silva et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}