 |
Case Report
Pediatric hereditary angioedema protocol for multiple extraction of teeth: A case report
1 King’s College Hospital NHS Foundation Trust, Denmark Hill, London, SE5 9RS, England
Address correspondence to:
Nermin Hayek
Dental Core Trainee, Oral and Maxillofacial Surgery, King’s College Hospital, King’s College Hospital, Denmark Hill, London, SE5 9RS,
England
Message to Corresponding Author
Article ID: 101238Z01NH2021
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Hayek N, Storey B, Davies R, Chellappah A, Hussain K. Pediatric hereditary angioedema protocol for multiple extraction of teeth: A case report. Int J Case Rep Images 2021;12:101238Z01NH2021.ABSTRACT
Introduction: Hereditary angioedema is a rare condition that can cause severe oropharyngeal and laryngo-tracheal swelling. Dental and maxillofacial surgeons should be aware that the swelling can be stimulated by the trauma of simple oral and dental extractions resulting in life-threatening airway compromise; especially in a pediatric population.
Case Report: We discuss a case of a 6-year-old male child with brittle hereditary angioedema who required the extraction of multiple carious deciduous teeth.
Conclusion: We describe our management from initial assessment to discharge; utilizing a patient-centered, multidisciplinary, evidence-based approach to successfully manage this child in order to provide a useful resource to inform safe clinical practice when encountering children with this rare condition.
Keywords: Angioedema, Dental, Extraction, Hereditary, Pediatric
Introduction
Hereditary angioedema (HAE) is a rare condition characterized by sudden and recurrent cutaneous or sub-mucosal swelling, secondary to transient increases in bradykinin-mediated vascular permeability. In the most common sub-type, the underlying pathophysiology centers on a deficiency or dysfunction of the functional C1 esterase inhibitor (C1-INH)—a protease regulator in the complement, plasma contact, fibrinolytic and coagulation pathways. It is a relatively uncommon condition affecting approximately 1 in 50,000 people with both male and females affected equally, it is inherited in an autosomal dominant pattern, and the most prevalent sub-type (HAE with reduced C1-INH) accounts for 85% of cases [1]. The condition is clinically characterized by potentially life-threatening recurrent episodes of swelling usually affecting the limbs, face, gastrointestinal tract, and airway [2]. There are numerous triggers for these episodes but of particular note to the dentist, surgeon, and anesthetist is that of stress, infection, and minor surgical trauma. Although C1 esterase inhibitor, due to its involvement in the fibrinolytic pathway and coagulation cascade, theoretically increases the risk of bleeding, it has not been shown to be significant in vivo. Given a small but extremely unfortunate handful of cases existing in the literature of death secondary to asphyxiation following tooth extraction, we present a case of successfully and uneventfully managing the extraction of seven deciduous teeth under general anesthetic in a 6-year-old child with brittle HAE [3].
Case Report
A 6-year-old boy presented to his local dentist Maidstone, UK, with extensive carious lesions involving seven of his deciduous teeth. His past medical history included HAE with reduced CI-INH Type 1, asthma, and eczema. He was under a pediatric immunology consultant but his HAE had remained unpredictable and difficult to manage. His triggers were mainly secondary to trauma, sometimes infection and other times spontaneous and he was suffering from attacks up to twice weekly requiring assessment in his local emergency department in Maidstone. Clinically, it manifested as oral and limb swelling, as well as abdominal discomfort and gastrointestinal disturbance.
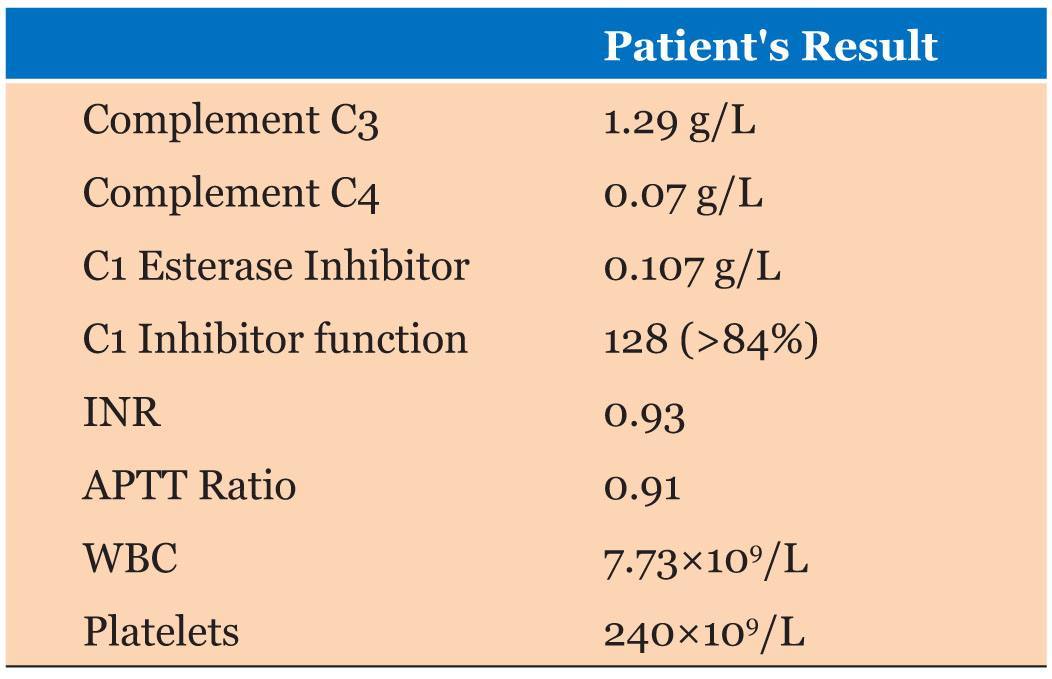
With regard to his HAE he was not taking any regular prophylactic medication, but was prescribed Icatibant and C1 esterase inhibitor concentrate (Berinert) for use during acute attacks. He also used a regular inhaled-corticosteroid and short-acting beta-agonist for his asthma. Of note, his father suffered from the same condition, which made the home management and administration of medication somewhat more manageable. Table 1 presents the patient’s pre-operative bloods.
Exodontia of deciduous teeth under local anesthetic (with or without inhaled sedation) in the pediatric population is frequently and routinely performed in primary care or the clinic setting, or secondary care with general anesthesia. However, given the unpredictable nature of this child’s HAE, and the potential for life-threatening airway compromise, it was decided that it would be more appropriate for the case to be managed in a tertiary hospital. It was felt that to safely deliver the care to this patient, provision of general anesthetic with a definitive airway, pre-operative consultation with tertiary specialists, capacity for a peri-operative surgical airway if required and post-operative level 2 or 3 care should all be available.
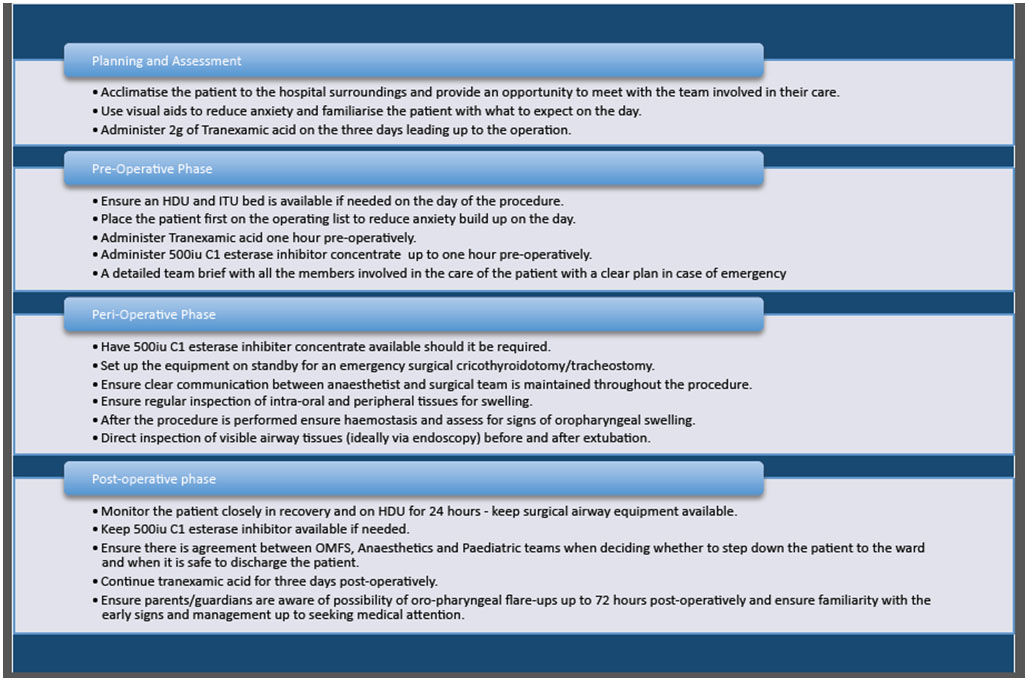
Extractions of his carious deciduous teeth under general anesthetic was thus subsequently planned and a full pre-operative assessment was jointly undertaken with input from oral and maxillofacial surgeons (OMFS), anesthetists, pediatricians, immunologists in King’s College Hospital, London, UK. A personalized plan was created and was carried out as detailed below. A summary is described in Figure 1.
Planning and assessment phase
The planning for the case began 6–8 weeks prior to surgery. To reduce stress (a known trigger) the patient was acclimatized to the hospital surroundings with multiple pre-operative appointments, providing the opportunity to meet and build rapport with all team members who would be actively involved in planning and delivering of his care; this included oral and maxillofacial surgery, anesthetics, pediatrics, and immunology & allergy. As part of the pediatrician aesthetic workup, the video “A Little Deep Sleep” was provided for the child to watch at home prior to his operation date, which aimed to put him at ease and reduce anxiety. After advice from our hematology colleagues, it was recommended that the child take 2 g of oral tranexamic acid each morning for the three pre-operative days to reduce the risk of post-operative hemorrhage.
Pre-operative phase
The patient was admitted the night before into a pediatric bed and was cannulated and pre-operative bloods taken. The post-operative high dependency unit bed was confirmed and a level 3 intensive therapy unit bed was also provisionally confirmed in case the child remained intubated or underwent a surgical airway and required a further period of ventilation. The patient was placed first on the operating list to diminish anxiety and provide ample time should any complications arise. The pre-planned dose of tranexamic acid was given, and 1 hour prior to intubation, 500 IU of C1 esterase inhibitor concentrate (Berinert) was given on the ward by the pediatric immunology specialist nurse known and familiar to the patient. A very detailed and clear briefing was undertaken with anesthetic, surgical, and theatre staff including our management plan in the event of acute swelling.
Intra-operative
The patient was planned to be anaesthetized and intubated in theatre, accompanied by his father and the immunology & allergy nurse specialist, and staff members and unnecessary sound was kept to a minimum to reduce anxiety. A further 500 IU C1 esterase inhibitor concentrate (Berinert) was available in the operating theatre in case of requirement during intubation or peri-operatively. The equipment for a surgical cricothyroidotomy and tracheostomy was set up with an appropriate size tracheostomy tube, with the oral and maxillofacial surgery consultant and specialist registrar scrubbed ready. The patient was anesthetized via an intravenous infusion and atraumatically intubated under direct vision with an endotracheal tube using a Glidescope. Clear communication between anesthetic and surgical team was maintained throughout to ensure swift surgical intervention if required. Once a safe definitive airway was confirmed, assessment for oropharyngeal swelling was undertaken and a throat pack was gently placed. It was decided that to reduce unnecessary trauma, local anesthetic would not be used. The surgery then proceeded without complication and all seven deciduous teeth were extracted. The extractions were performed as atraumatically as possible and suturing of the sockets (with 4-0 vicrylrapide), although undertaken where required, was minimized. During the case regular inspections of the intra-oral tissues, as well as the rest of the body were undertaken to assess for swelling that might otherwise go unnoticed. Damp gauze was then placed under gentle compression over the sockets for 10 minutes to ensure hemostasis. Post-procedure, the throat pack was removed and the anesthetic team thoroughly assessed the airway via the Glidescope. A joint consultant decision was made that there were no signs of swelling in the mouth, oropharynx, or visible larynx and the patient was extubated in theatre. The separate trolley with the equipment for a surgical airway was kept available and the surgeons remained scrubbed until the patient was transported to recovery.
Post-operative
The patient was monitored closely in recovery and then on high dependency unit (HDU) for 24 hours. A further 500 IU C1 esterase inhibitor concentrate (Berinert) was made available in case of any signs of swelling. At 24 hours a joint pediatric, anesthetic, and OMFS consultant decision was made that the child could be stepped down to the ward and would be appropriate to be discharged later that day. A discussion was had regarding the latency period in which a flare up may occur and whether the child should stay for 36 hours. Given his father has the same condition, and is used to identifying the early signs, giving the rescue medications and frequently attending the local emergency departments, it was felt that this social situation facilitated safe discharge at approximately 30 hours. The tranexamic acid was continued for three days post-operatively. We were pleased to hear that the child recovered well with no post-operative complications.
Discussion
Although HAE is a rare condition, its relevance in dentistry remains of great importance due to its potentially lethal consequences. The literature has reported several deaths following extractions in both adults and children with HEA, specifically a delayed onset of laryngeal asphyxiation up to two days post-operatively [3],[4],[5],[6]. This clearly highlights the need for strategic planning using a multidisciplinary approach that follows guidance from the literature. Bork et al. (2003) report that facial swelling and/or laryngeal edema appeared in 21.5% of tooth extractions without prophylaxis of C1-INH concentrate compared to 12.5% of cases in those receiving prophylactic C1-INH [5]. This must, therefore, support the decision to administer pre-operative prophylactic C1 esterase inhibitor concentrate in HAE patients. Clinicians should also have an open discussion with the patient and, in cases of children, their parents, of the very realistic possibility of a flare of symptoms up to 72 hours post-operatively [7]. Our recommendation is that inpatient monitoring in such patients should be strongly considered ideally with level 2 care. Anxiety is known to trigger HAE, therefore the psychological and holistic wellbeing of patients must be put on equal footing as his or her physical health during the work-up for any intervention or treatment. The case highlighted to us the paramount importance of communication and multi-disciplinary working throughout the planning, pre-, peri, and post-operative aspects of care in complex cases like this.
When considering the high risks involved with invasive procedures in children with HAE, particularly in those where the risks are significantly higher, prevention may be better than cure. In a general dental setting, preventative measures must be implemented in patients with high risk conditions; the “Delivering Better Oral Health Toolkit” provides evidence-based guidelines in this regard [8],[9],[10]. Clinicians should also ensure a strong rapport is built with our more vulnerable patients to optimize mental wellbeing when visiting their dental practitioner. Finally, a thorough medical history must be elicited from each patient at every visit to gather all relevant information for treatment planning which includes family history to elicit hereditary conditions.
Conclusion
Hereditary angioedema is a potentially fatal condition if not managed appropriately. Minor dental surgery, infection, and the associated anxiety can trigger an attack and result in life-threatening airway compromise. Management of these patients is complex and we feel best undertaken in a controlled secondary care environment. Despite the low prevalence, perhaps an evidence-informed pathway is a future area for development. However, what we hope we have shown is that with thorough and focused forward planning, holistic care, multi-disciplinary input, pre-emptive treatment, clear communication, and effective teamwork, a routine case of pediatric exodontia can remain exactly that.
REFERENCES
1.
Busse PJ, Christiansen SC. Hereditary angioedema. N Engl J Med 2020;382(12):1136–48. [CrossRef]
[Pubmed]

2.
Ghazi A, Grant JA. Hereditary angioedema: Epidemiology, management, and role of icatibant. Biologics 2013;7:103–13. [CrossRef]
[Pubmed]
3.
Bracho FA. Hereditary angioedema. Curr Opin Hematol 2005;12(6):493–8. [CrossRef]
[Pubmed]
4.
Schürmann D, Herzog E, Raquet E, et al. C1-esterase inhibitor treatment: Preclinical safety aspects on the potential prothrombotic risk. Thromb Haemost 2014;112(5):960–71. [CrossRef]
[Pubmed]
5.
Forrest A, Milne N, Soon A. Hereditary angioedema: Death after a dental extraction. Aust Dent J 2017;62(1):107–10. [CrossRef]
[Pubmed]
6.
Rosa A, Miranda M, Franco R, Guarino MG, Barlattani A Jr, Bollero P. Experimental protocol of dental procedures in patients with hereditary angioedema: The role of anxiety and the use of nitrogen oxide. Oral Implantol (Rome) 2016;9(2):49–53. [CrossRef]
[Pubmed]
7.
Bork K, Barnstedt SE. Laryngeal edema and death from asphyxiation after tooth extraction in four patients with hereditary angioedema. J Am Dent Assoc 2003;134(8):1088–94. [CrossRef]
[Pubmed]
8.
Davies GM, Davies RM. Delivering better oral health – an evidence-based toolkit for prevention: A review. Dent Update 2008;35(7):460–2. [CrossRef]
[Pubmed]
9.
Hosokawa R, Tsukamoto M, Nagano S, Yokoyama T. Anesthetic management of a patient with hereditary angioedema for oral surgery. Anesth Prog 2019;66(1):30–2. [CrossRef]
[Pubmed]
10.
Rice S, Cochrane TJ, Millwaters M, Ali NT. Emergency management of upper airway angio-oedema after routine dental extraction in a patient with C1 esterase deficiency. Br J Oral Maxillofac Surg 2008;46(5):394–6. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Nermin Hayek - Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Bradley Storey - Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Rhodri Davies - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Anthony Chellappah - Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Karim Hussain - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2021 Nermin Hayek et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}