 |
Case Report
Multimodal imaging of psoriatic arthritis triggered by Chikungunya fever
1 PhD student in Medicine, Department of Radiology, Rio de Janeiro State University, Rio de Janeiro, RJ, Brazil
2 Adjunct Professor of Rheumatology, Department of Rheumatology, Federal University of the State of Rio de Janeiro, RJ, Brazil
3 Adjunct Professor of Pediatric Rheumatology, Department of Rheumatology, Rio de Janeiro State University, Rio de Janeiro, RJ, Brazil
4 Doctor resident in Rheumatology, Department of Rheumatology, Rio de Janeiro State University, Rio de Janeiro, RJ, Brazil
5 Associate Professor of Radiology, Department of Radiology, Rio de Janeiro State University, Rio de Janeiro, RJ, Brazil
Address correspondence to:
Caio Leal Leidersnaider
Rua Barão da Torre, 445/805, 22411-003 Rio de Janeiro, RJ,
Brazil
Message to Corresponding Author
Article ID: 101229Z01CL2021
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Leidersnaider CL, Vaz JLP, Sztajnbok FR, Gonçalves MT, Mogami R. Multimodal imaging of psoriatic arthritis triggered by Chikungunya fever. Int J Case Rep Images 2021;12:101229Z01CL2021.ABSTRACT
Chikungunya fever (CF), caused by the Chikungunya virus (CHIKV), is an arboviral disease transmitted by infected Aedes mosquitoes found worldwide. Although CF may trigger chronic arthritis, there are still few reports of patients who have progressed to psoriatic arthritis (PsA). We describe the clinical and ultrasound (US) and magnetic resonance imaging (MRI) findings of the wrist and hands of a 49-year-old man who had peripheral PsA triggered by CHIKV. He had scaly, itchy scalp lesions three months after the diagnosis of CF. The patient had classic synovitis and tenosynovitis secondary to CF. The persistence of inflammatory disease with signs of enthesitis and dactylitis on magnetic resonance imaging (MRI) and US, family history and appearance of skin lesions on the scalp strongly suggest post-CF PsA. Viral infections can be a triggering factor for several diseases with chronic arthritis, such as PsA. Imaging exams are essential methods for both diagnosis and the monitoring of treatment.
Keywords: Arthritis, Chikungunya fever, Magnetic resonance imaging, Psoriatic, Ultrasonography
Introduction
Chikungunya fever (CF) is a viral disease whose transmission occurs through vector females of Aedes aegypti and Aedes albopictus mosquitoes infected by the Chikungunya virus (CHIKV). There are reports of outbreaks in Europe, the Americas, Asia, Africa, and Oceania [1].
Approximately 60% of patients with CHIKV infection progress to chronic arthritis [2]. In these cases, joint limitations can persist for up to five years after infection [3] and are associated with permanent sequelae [4]. After an incubation period of three to seven days, patients may experience fever, skin rash, myalgia, and arthralgia. The disease becomes chronic when the arthralgias persist for more than three months. The literature shows that a small portion of patients with chronic CF and severe polyarticular forms develop rheumatoid arthritis (RA) [5] or other forms of arthritis, including psoriatic arthritis (PsA) [6].
Conventional radiology is still a first-line exam in the investigation of rheumatological diseases. However, the method is not as sensitive as MRI or US in showing early bone and soft tissue changes. Although US has limitations in bone evaluation, together with Doppler it can identify early signs of enthesitis or organ-enthesis involvement [7]. Conventional MRI, in turn, is useful for diagnosing bone complications such as marrow edema and erosions as well as soft tissue involvement [8].
The pattern of involvement of the hands and wrists by CF is very similar to that found in RA, and it is characterized by symmetrical and bilateral involvement of the metacarpophalangeal and proximal interphalangeal joints, tenosynovitis, subcutaneous edema, and bone changes, such as marrow edema and erosions [9].
Although there have been several reports of developing RA, to our knowledge, there are few descriptions of post-CF PsA. Mathew et al. [5] investigated 1396 individuals with CF and concluded that only 2.5% of patients developed PsA. Thus, our report is valuable due to the scarcity of cases, and it features an imaging presentation typical of peripheral spondyloarthropathy secondary to arbovirus infection.
Case Report
A 49-year-old man had a fever (101.30°F/38.5°C) for approximately ten days and exhibited persistent signs of polymyalgia and polyarthralgia. He used dipyrone and oral hydration to reduce the fever, and his musculoskeletal symptoms partially improved. Serologies for CHIKV were positive for IgM (51; normal value: 9). Subsequently, a skin rash appeared, and polyarthralgia associated with edema of the hands, wrists (Figure 1), elbows, knees, and feet worsened. Two months later, he was evaluated in an outpatient rheumatology clinic at a university hospital in Rio de Janeiro, Brazil. He continued to experience polyarthralgia and edema in the metacarpophalangeal and interphalangeal joints, especially of the left hand. Erythematous scaling and itchy skin lesions were also noted in the anterior medial region of the scalp on physical examination. At the time, the patient was not taking any known medication that could precipitate psoriasis. He also denied any preceding emotional stress (at least two months prior to the appearance of the skin lesion). The patient had never had any episode of psoriatic skin lesions. The patient was hypertensive, using enalapril 20 mg/day, and was an abstainer, nonsmoker, and physically active. He denied allergies and blood transfusions and had an up-to-date vaccination schedule. His father had PsA. One maternal aunt had multiple sclerosis, and another had ankylosing spondylitis.
The rheumatologists prescribed meloxicam 15 mg/day and prednisone 20 mg/day after discussing the case. The patient returned the following month with little clinical improvement, and methotrexate 15 mg and folic acid 5 mg were started after verification of the laboratory tests.
After starting the medication, he was followed up on an outpatient basis and remained asymptomatic. However, the patient stopped medication on his own, and after two years and four months he returned to the outpatient clinic with symptom recrudescence. After that, the joint pain returned, but the psoriatic skin lesions did not. He was re-evaluated with US and MRI.
Written consent was obtained from the patient to be evaluated at the rheumatology outpatient clinic and the radiology department of a university hospital in the city of Rio de Janeiro, Brazil.
There were no changes in the patient’s complete blood count: C-reactive protein 13 mg/L (normal index: up to 3 mg/L), fibrinogen 340 mg/dL (normal index: 200–400 mg/dL), and normal levels of transaminases and electrolytes (sodium and potassium). The nonreactive immunological tests included the following: antinuclear factor (ANA), antibodies against citrullinated peptides (ACPA), rheumatoid factor (RF), and cytoplasmic antineutrophil antibodies (ANCA). Serological tests for HIV and hepatitis B and C were nonreactive; CHIKV IgM and IgG were reactive; and HLA-B27 was negative.
The equipment used was a Toshiba US, model Aplio XG, with a 7–18 MHz multifrequency probe, in B mode and with power Doppler (pulse repetition frequency 750 Hz, low wall filter and gain adjusted just below the appearance of the artifacts).
The MRI scans were performed in a Siemens model Avanto, 1.5 T high-field scanner. The image acquisition protocol had the following sequences: protonic density (PD) with fat saturation in the axial, sagittal, and coronal planes and T1 pre- and post-contrast fat saturation in the axial plane.
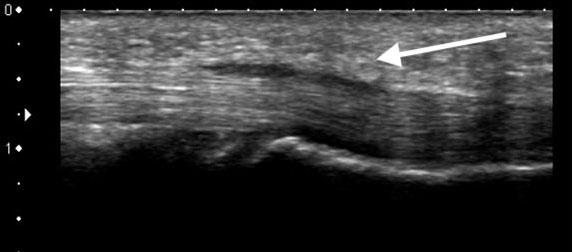
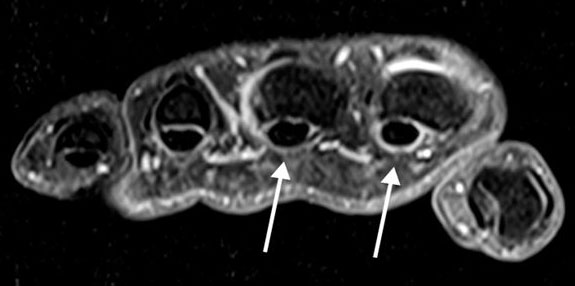
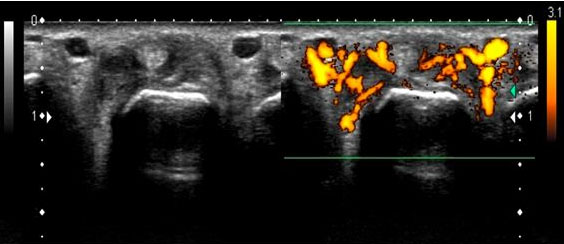
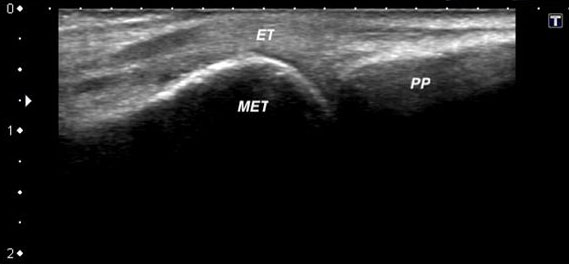
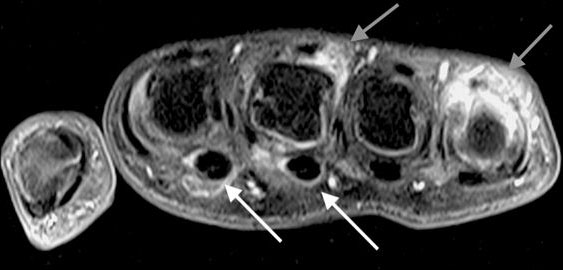
The US and MRI scans showed signs of arthritis in the wrist and metacarpophalangeal joints of both hands. There was also tenosynovitis of all extensor compartments, digital flexor tenosynovitis (Figure 2 and Figure 3), and signs of classical enthesitis due to thickening of the digital extensor entheses and functional enthesitis (Figure 4, Figure 5, Figure 6) due to peritendinous extensor thickenings. Vascular hyperflow was observed by power Doppler (Figure 4) at several sites of inflammation, paramagnetic contrast enhancement of the distended sheaths, and functional enthesitis sites. Focal bone edema was identified as an indirect sign of enthesitis at the base of the left third metacarpal associated with signs of inflammation of the extensor carpi radialis brevis.

Discussion
The authors present an unusual complication of CF suggested by clinical and imaging findings. US and MRI were also essential during the treatment follow-up.
According to the Classification Criteria for Psoriatic Arthritis (CASPAR) [10], to confirm the diagnosis of PsA, it is necessary to have an inflammatory joint disease and at least a three-point score in the other categories. The patient had a five-point score due to scalp psoriasis (two points), family history (one point), negative RF (one point), and dactylitis (one point). As reported in other literature cases, these signs and symptoms appeared immediately after CF infection, and the disease regressed with methotrexate therapy [5].
The patient’s age and gender profiles disagree with the literature, which describes a predominance in women over 45 years old who are at risk for musculoskeletal complications in CF [11]. Among the usual manifestations of CF, the presentation of only fever, polymyalgia, polyarthralgia, and skin rash and the high levels of C-reactive protein are in accordance with the literature [12].
The US and MRI scans showed several signs of involvement, with characteristics of spondyloarthropathy: dactylitis due to flexor tenosynovitis, classic enthesitis in distal extensor insertions, functional enthesitis due to peritendinous extensor thickening adjacent to the metacarpophalangeal and interphalangeal joints, and metacarpal marrow edema adjacent to the insertion of an extensor tendon.
After the 2015–2016 CF outbreak in Rio de Janeiro, Brazil, our group [9],[13] reported wrist/hand and ankle ultrasound changes. The authors highlighted bilateral synovitis and tenosynovitis as relevant findings for the diagnosis of musculoskeletal complications. However, in this case report, the existence of several signs of very intense enthesitis and flexor tenosynovitis in the imaging exams raised the suspicion of some other disease associated with CF.
There are two types of entheses according to function and location: fibrous and fibrocartilage. The most common fibrocartilage is found in the apophyses and epiphyses of long bones, short bones of the hands and feet, and several ligaments in the spine. Fibrous entheses are found in the metaphyses and diaphyses of long bones. Fibrocartilaginous entheses are those affected in spondyloarthropathies and altered in the US and MRI exams of the reported case [14], [15].
Functional enthesis is another essential concept to understanding our imaging findings. In specific locations where the tendon deflects or rubs against a bone surface, there are sesamoid (tendinous) and periosteal fibrocartilages. This patient had intense digital peritendinous extensor inflammatory thickenings, which are explained by these functional enthesis impairments [16],[17].
Dactylitis is one of the main features of psoriatic arthritis and is present in 40% of cases. The main finding is digital flexor tenosynovitis, that is, distention of the fibrous sheaths, which also existed in the reported case [18].
Clinical recognition of early-stage PsA is challenging when the disease affects only the peripheral joints. Despite the efficiency of CASPAR in identifying patients with less than one year of symptom onset (early psoriatic arthritis) [19], peripheral PsA remains a challenge for rheumatologists [20]. In our case, imaging helped detect the entheseal manifestations of the disease, suggesting alternative diagnoses in CF patients.
Conclusion
With the resurgence of CF epidemics worldwide, managing chronic arthritis has become an enormous challenge for rheumatologists. It is essential to follow these chronic cases and to identify the progression to other forms of arthritis, such as PsA. Imaging exams have become indispensable for the diagnosis and management of these complications.
REFERENCES
1.
Weaver SC, Lecuit M. Chikungunya virus and the global spread of a mosquito-borne disease. N Engl J Med 2015;372(13):1231–9. [CrossRef]
[Pubmed]

2.
Essackjee K, Goorah S, Ramchurn SK, Cheeneebash J, Walker-Bone K. Prevalence of and risk factors for chronic arthralgia and rheumatoid-like polyarthritis more than 2 years after infection with Chikungunya virus. Postgrad Med J 2013;89(1054):440–7. [CrossRef]
[Pubmed]
3.
Schilte C, Staikowsky F, Couderc T, et al. Chikungunya virus-associated long-term arthralgia: A 36-month prospective longitudinal study. PLoS Negl Trop Dis 2013;7(3):e2137. [CrossRef]
[Pubmed]
4.
Bouquillard E, Fianu A, Bangil M, et al. Rheumatic manifestations associated with Chikungunya virus infection: A study of 307 patients with 32-month follow-up (RHUMATOCHIK study). Joint Bone Spine 2018;85(2):207–10. [CrossRef]
[Pubmed]
5.
Mathew AJ, Goyal V, George E, et al. Rheumatic-musculoskeletal pain and disorders in a naïve group of individuals 15 months following a Chikungunya viral epidemic in south India: A population based observational study. Int J Clin Pract 2011;65(12):1306–12. [CrossRef]
[Pubmed]
6.
Chen LH, Sehra ST. Chikungunya virus infection-associated psoriatic arthritis? Mayo Clin Proc 2019;94(7):1384–6. [CrossRef]
[Pubmed]
7.
Möller I, Loza E, Uson J, et al. Recommendations for the use of ultrasound and magnetic resonance in patients with rheumatoid arthritis. Reumatol Clin 2018;14(1):9–19. [CrossRef]
[Pubmed]
8.
Sudoł-Szopińska I, Jans L, Teh J. Rheumatoid arthritis: What do MRI and ultrasound show. J Ultrason 2017;17(68):5–16. [CrossRef]
[Pubmed]
9.
Mogami R, Pereira Vaz JL, de Fátima Barcelos Chagas Y, et al. Ultrasonography of hands and wrists in the diagnosis of complications of Chikungunya fever. J Ultrasound Med 2018;37(2):511–20. [CrossRef]
[Pubmed]
10.
Taylor W, Gladman D, Helliwell P, et al. Classification criteria for psoriatic arthritis: Development of new criteria from a large international study. Arthritis Rheum 2006;54(8):2665–73. [CrossRef]
[Pubmed]
11.
Sissoko D, Malvy D, Ezzedine K, et al. Post-epidemic Chikungunya disease on Reunion Island: Course of rheumatic manifestations and associated factors over a 15-month period. PLoS Negl Trop Dis 2009;3(3):e389. [CrossRef]
[Pubmed]
12.
Miner JJ, Aw-Yeang HX, Fox JM, et al. Chikungunya viral arthritis in the United States: A mimic of seronegative rheumatoid arthritis. Arthritis Rheumatol 2015;67(5):1214–20. [CrossRef]
[Pubmed]
13.
Mogami R, de Almeida Vieira A, Junqueira Filho EA, Lopes AJ. Chikungunya fever outbreak in Rio de Janeiro, Brazil: Ultrasonographic aspects of musculoskeletal complications. J Clin Ultrasound 2017;45(1):43-4. [CrossRef]
[Pubmed]
14.
Kaeley GS, Eder L, Aydin SZ, Gutierrez M, Bakewell C. Enthesitis: A hallmark of psoriatic arthritis. Semin Arthritis Rheum 2018;48(1):35–43. [CrossRef]
[Pubmed]
15.
Watad A, Eshed I, McGonagle D. Lessons learned from imaging on enthesitis in psoriatic arthritis. Isr Med Assoc J 2017;19(11):708–11.
[Pubmed]
16.
McGonagle D, Lories RJU, Tan AL, Benjamin M. The concept of a “synovio-entheseal complex” and its implications for understanding joint inflammation and damage in psoriatic arthritis and beyond. Arthritis Rheum 2007;56(8):2482–91. [CrossRef]
[Pubmed]
17.
Shaw HM, Benjamin M. Structure-function relationships of entheses in relation to mechanical load and exercise. Scand J Med Sci Sports 2007;17:303–15. [CrossRef]
[Pubmed]
18.
Tan AL, Fukuba E, Halliday NA, Tanner SF, Emery P, McGonagle D. High-resolution MRI assessment of dactylitis in psoriatic arthritis shows flexor tendon pulley and sheath-related enthesitis. Ann Rheum Dis 2015;74(1):185–9. [CrossRef]
[Pubmed]
19.
Coates LC, Conaghan PG, Emery P, et al. Sensitivity and specificity of the classification of psoriatic arthritis criteria in early psoriatic arthritis. Arthritis Rheum 2012;64(10):3150–5. [CrossRef]
[Pubmed]
20.
Furlan A, Stramare R. The thickening of flexor tendons pulleys: A useful ultrasonographical sign in the diagnosis of psoriatic arthritis. J Ultrasound 2018;21(4):309–14. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Caio Leal Leidersnaider - Conception of the work, Design of the work, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
João Luiz Pereira Vaz - Acquisition of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Flávio Roberto Sztajnbok - Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Marcelo Torres Gonçalves - Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Roberto Mogami - Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2021 Caio Leal Leidersnaider et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}