 |
Case Report
A giant solitary fibrous tumor of the mesentery: Case report
1 Department of General Surgery, CHEDV – São Sebastião Hospital, Santa Maria da Feira, Portugal
Address correspondence to:
Lúcia Carvalho
5 Doutor Cândido Pinho Street, 4520-211, Santa Maria da Feira,
Portugal
Message to Corresponding Author
Article ID: 101210Z01LC2021
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Carvalho L, Matos L, Pereira AM, Almeida RF, Lima AT, Nora M. A giant solitary fibrous tumor of the mesentery: Case report. Int J Case Rep Images 2021;12:101210Z01LC2021.ABSTRACT
Introduction: Solitary fibrous tumor is a rare neoplasm of mesenchymal origin that typically arises from pleura. Mesentery origin is an extremely rare presentation. Although benign in most cases, surgery with en bloc resection of the tumor is the treatment modality due to the possibility of malignancy and allows a final histopathological and immunohistochemical diagnosis.
Case Report: We report a case of a giant solitary fibrous tumor of the mesentery of the small intestine in a 74-year-old patient who was referred to our hospital for an intermittent and vague abdominal pain. Physical examination revealed a dolorous and immobile mass palpable on right lower quadrant which was initially thought to be a gastrointestinal stromal tumor (GIST). The mass was successfully resected and the diagnosis of a solitary fibrous tumor was confirmed on immunohistochemical analysis. The patient was discharged 4 days after surgery and had an uneventful clinical course throughout the 12-month postoperative follow-up.
Conclusion: We present an uncommon localization of a solitary fibrous tumor, arising from the small bowel mesentery and with a large dimension. Since solitary fibrous tumor may show aggressive behavior with frequent local recurrence, careful long-term follow-up has been recommended for the rare cases of extrapleural solitary fibrous tumor.
Keywords: Abdominal mass, Mesenchymal tumor, Small bowel mesentery, Solitary fibrous tumor
Introduction
Solitary fibrous tumor (SFT) is a rare neoplasm of mesenchymal origin that can occur in any part of the body [1]. It mainly arises from the thoracic cavity (pleura and lung) although other extra-thoracic locations such as orbit, thyroid, breast and central nervous system have been reported [2]. These ubiquitous mesenchymal tumors were first described in 1931 by Klemperer and Rabin as a distinct mesothelial tumor characterized by high fibrosis and hypervascularity [3].
Solitary fibrous tumors are usually localized benign tumors that remain asymptomatic until local compression on adjacent organs appears, hampering the diagnosis [4].
Preoperative computed tomography (CT) and magnetic resonance imaging (MRI) are the imaging techniques of choice to identify and characterize the tumor, although immunohistopathology and immunohistochemical analysis are needed to definitive diagnosis.
Solitary fibrous tumor is a well-circumscribed and frequently encapsulated mass but with malignant features such as invasion of surrounding tissues and may occur in exceptional cases. Considering the possibility of malignancy, complete surgical resection with negative margins is recommended. Long-term surveillance after surgery is required once recurrence may occur 20 years after primary treatment [4].
Although SFTs are well described, involvement of the mesentery is seldom reported in the literature [5]. The authors present a case of a giant solitary fibrous tumor of the mesentery in a 74-year-old man.
Case Report
A 74-year-old man with no remarkable medical history was referred to our hospital due to an abdominal mass detected during investigation of an intermittent abdominal pain. He denied any recent weight loss, nausea, anorexia, vomiting and diarrhea.
On clinical examination, there was a palpable, dolorous and immobile mass on right upper quadrant. Routine blood analyses were normal.
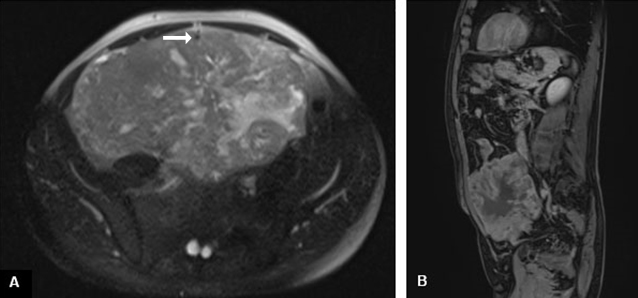
The abdominal ultrasound revealed the presence of a large pelvic lesion. Further evaluation with abdominopelvic CT showed a large solid heterogeneous mass measuring 17×11×5 cm and centered in mesentery, in an infra-umbilical localization (Figure 1). Magnetic resonance imaging supported the CT scan in regard to the location as well as the contrast enhancement (Figure 2), suggesting malignancy in both images. The appearance and the contrast enhancement pattern were suggestive of a gastrointestinal stromal tumor (GIST) or a mesenchymal tumor. No metastasis in the adjacent organs or peritoneal cavity was observed.
The patient was proposed to surgical exploration and tumor resection. A midline laparotomy exposed a large rounded and well-demarcated mass arising from the mesentery root but without involving it, measuring 20 × 25 cm (Figure 3). En bloc resection was performed without compromising small bowel vascular supply.
The histopathological analysis of the mass revealed spindle-shaped cells with slightly nuclear atypia. Areas of necrosis were found in <5% of the tumor. There were 2 mitoses per 300 HPF and a Ki-67 index of 15%. Immunohistochemical analysis revealed positivity for bcl-2, CD99, B-catenin, vimentin and with focal positivity for CD34. There was consistent negative staining for CD117, S100 protein, smooth muscle actin, desmin, c-kit and DOG-1. Surgical margins were clear.
The patient had an uneventful postoperative course and was discharged on the 4th postoperative day. So far, 12 months of follow-up with abdominopelvic CT showed no evidence of recurrence.


Discussion
Solitary fibrous tumors are rare mesenchymal neoplasms that most frequently arise from the pleura. Lung, mediastinum, pericardium, nose, paranasal sinuses and central nervous system are less frequent locations [6]. Mesentery is an extremely rare presentation of this tumor.
Scarce literature about mesenteric SFTs reports a slightly male predominance and middle age presentation.
Clinical manifestations are variable and depend on the size and location of the tumor. Solitary fibrous tumors are painless, slow growing, unless other organs compression or incidental diagnosis is made for other reasons. The etiology of this lesion remains unclear [2].
The resemblance with other benign and malign tumors (desmoids, inflammatory pseudotumors, leiomyomas, gastrointestinal stromal tumors, soft tissue sarcomas, lymphomas, and metastasis) with different treatment options and prognosis make the decision to operate difficult with no reliable preoperative diagnostic exam available. Although it is difficult to make a definitive diagnosis of an SFT before surgery, CT or MRI may help to identify the tumor by analyzing its morphology, density, composition and enhancement pattern. Imagiologic features as the presence of rounded necrotic areas, calcifications, and enhancement pattern in the arterial, portal venous, and delayed phases of CT scan suggest SFT in contrast with other neoplasms arising from the mesentery.
Considering the inability to exclude malignancy, the presence of a solid mass lesion of the mesentery that is not thought to be a reactive lymph node or lymphoma is an indication for surgical removal. Prolonged observation and repetitive studies with biopsy are discouraged except in selected circumstances, particularly when lymphoma is suspected.
Due to the rarity of SFTs in this particular in these locations, guidelines for treatment remain unclear. In general, effective medical treatment for neoplastic mesenteric masses is not available. Surgical resection is the most effective treatment for SFTs and allows a final histopathological and immunohistochemical diagnosis. Surgical complete resection is considered when clear margins are obtained and that may involve en bloc resection of other involved structures. In this case, the lesion was completely removed with negative margins with no need of resection of adjacent organs. Definitive diagnosis was made by immunohistochemical analysis.
The role of other treatment modalities in the management of SFTs such as radiotherapy and chemotherapy is controversial, with ambiguous results. Effective radiotherapy with palliative intention in cases not suitable for surgery, as well as an adjuvant therapy has been reported in literature [4]. Antiangiogenic therapy is also evolving for unresectable cases so far with promising results [7].
Up to 20% of SFTs are malignant [8]. The malignant variant is characterized by large a mass (>50 mm in diameter) and histologic features such as hypercellularity, necrosis, cellular atypia, and a high mitotic index (>4 mitoses per 10 HPF) [2].
In this case, histological analysis revealed hypercellularity, cellular atypia with no hemorrhagic areas and tumoral necrosis in less than 5% of the mass. Mitotic index was 2 mitoses per 300 HPF. Based on these findings, this tumor was considered benign in nature.
Solitary fibrous tumor’s prognosis is unknown; however, recurrence rate and distant metastases are up to 50%, occurring many years later [9]. Hematogenic spread to lungs, liver, and bone result the most common sites of metastasis [10].
Long-term surveillance, with CT scans every six months for the first two years and then annually is recommended, especially in high mitotic index and large tumors [2]. Follow-up of 12 months after surgery showed no evidence of recurrence or distant metastasis is this case.
Conclusion
We report a case of a rare mesenteric SFT, probably one of the largest reported in the literature. Despite resemblance with other solid tumors, CT scan and MRI are the best available exams to guide toward a differential diagnosis. Recommended treatment is complete surgical resection with clear margins and long-term follow-up is mandatory due to high risk of recurrence and distant metastasis.
REFERENCES
1.
Zhang GJ, Li RT, Zhou Y, et al. Solitary fibrous tumor of small bowel mesentery with postoperative bowel obstruction: A case report and review of literature. Int J Clin Exp Pathol 2015;8(9):11691–7.
[Pubmed]

2.
Nishida K, Ubukata H, Konishi S, et al. A giant solitary fibrous tumor of the mesentery: A case report and literature review. World J Surg Oncol 2015;13:17. [CrossRef]
[Pubmed]
3.
You X, Sun X, Yang C, Fang Y. CT diagnosis and differentiation of benign and malignant varieties of solitary fibrous tumor of the pleura. Medicine (Baltimore) 2017;96(49):e9058. [CrossRef]
[Pubmed]
4.
Liu JN, Liu Z, Ji PY, Zhang H, Guo SL. Solitary fibrous tumor of the mesentery: A case report and review of the literature. J Int Med Res 2020;48(10): 300060520950111. [CrossRef]
[Pubmed]
5.
Urabe M, Yamagata Y, Aikou S, et al. Solitary fibrous tumor of the greater omentum, mimicking gastrointestinal stromal tumor of the small intestine: A case report. Int Surg 2015;100(5):836–40. [CrossRef]
[Pubmed]
6.
Gold JS, Antonescu CR, Hajdu C, et al. Clinicopathologic correlates of solitary fibrous tumors. Cancer 2002;94(4):1057–68. [CrossRef]
[Pubmed]
7.
Vella S, Cannataci C, Cortis K. Solitary fibrous tumour of the mesentery: A case report. BJR Case Rep 2017;4(1):20170057. [CrossRef]
[Pubmed]
8.
Gengler C, Guillou L. Solitary fibrous tumour and haemangiopericytoma: Evolution of a concept. Histopathology 2006;48(1):63–74. [CrossRef]
[Pubmed]
9.
Park MS, Araujo DM. New insights into the hemangiopericytoma/solitary fibrous tumor spectrum of tumors. Curr Opin Oncol 2009;21(4):327–31. [CrossRef]
[Pubmed]
10.
Bouhabel S, Leblanc G, Ferreira J, Leclerc YE, Dubé P, Sidéris L. Solitary fibrous tumor arising in the mesentery: A case report. World J Surg Oncol 2011;9:140. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Lúcia Carvalho - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Leonor Matos - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Ana Marta Pereira - Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Rui Ferreira Almeida - Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Artur Trovão Lima - Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Mário Nora - Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2021 Lúcia Carvalho et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}