 |
Case Report
Double aortic arch (DAA): An unusual cause of dysphagia
1 Radiology Department, International Institute of Oncology, Mohammed V University, Rabat, Morocco
Address correspondence to:
El Harras Yahya
Radiology Department, International Institute of Oncology, Mohammed V University, Rabat,
Morocco
Message to Corresponding Author
Article ID: 101205Z01EY2021
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Yahya EH, Kaoutar I, Hounayda J, Rachida L, Youssef O. Double aortic arch (DAA): An unusual cause of dysphagia. Int J Case Rep Images 2021;12:101205Z01EY2021.ABSTRACT
Introduction: Vascular rings, due to the double aortic arch, are a class of congenital anomalies, considered as an important cause of tracheoesophageal compression. These anomalies are usually symptomless and thus are diagnosed fortunately when imaging is being performed for other reasons.
Case Report: We report a clinical case of a patient with a history of dysphagia in his childhood, never labeled or treated.
Conclusion: Currently, advanced imaging, especially computed tomography (CT), is the diagnostic procedure of choice of the double aortic arch. It can be associated with other anatomical variants. Surgical repair leads to excellent long-term prognosis.
Keywords: Double aortic arch, Dysphagia, Vascular ring
Introduction
Aortic arch malformations are a large spectrum of variations and anomalies which originate from disordered embryogenesis of branchial arches. Clinically, these aberrations can be symptomless, and are usually diagnosed when imaging is being performed for some other reasons. However, it may present with severe respiratory or esophageal symptoms especially when associated with complete vascular rings [1].
Double aortic arch (DAA) is the most common type of vascular ring malformation, in which the trachea and esophagus are completely encircled by connected segments of the aortic arch and its branches. Wolman first reported the clinical syndrome of vascular compression produced by a DAA in 1939 [2],[3].
Case Report
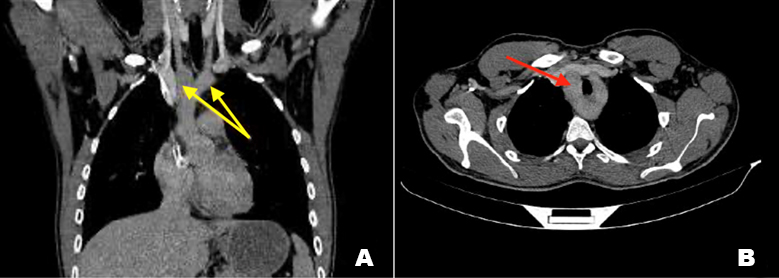
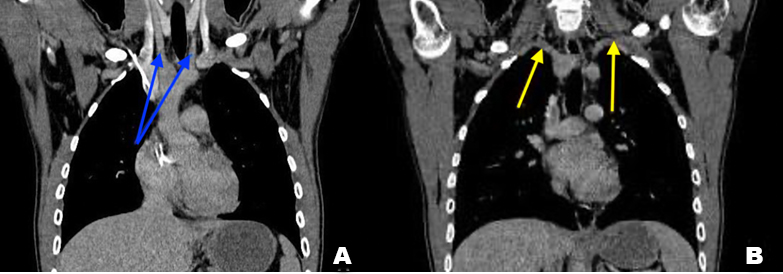
We report a case of a 27-year-old male patient, chronic smoker, presenting to our department for difficulties in swallowing evolving for several years never explored. Upper gastrointestinal (GI) endoscopy was normal. Contrast enhanced thoracic CT scan was realized showing a double aortic arch (DAA) with the ascending aorta seen splitting into the right arch and the left arch (Figure 1A). The double arch forms a vascular ring with compression of the proximal esophagus posteriorly as well as abutment and slight compression of the trachea (Figure 1B). The right and left arch have the same diameter, and each one gives rise to the ipsilateral subclavian and common carotid arteries (Figure 2). Then both arches unite posteriorly and form the descending aorta. Our scan showed no other cardiac anomaly.

Discussion
Aortic arch development is a complex process that occurs between weeks two and seven of gestational life. Six pairs of arches appear and disappear at different times, leaving remnants that form important vessels. In early weeks, the first two arches regress, leaving the maxillary, hyoid, and stapedial arteries. The third branch forms the common carotid arteries and a small portion of the internal carotid arteries, and the bilateral aortic arches emanate from the fourth pair of arches. In week five of gestation, the right-sided arch regresses and the left-sided arch remains, leaving a normal left-sided aortic arch [3]. The formation of a DAA originates from a failed regression of the right-sided arch with the persistence of the left-sided arch.
The aortic arches give rise to the ipsilateral subclavian and common carotid arteries (Figure 3), and the innominate artery is absent [4],[5].
In accordance with its anatomic characteristics, DAA has been divided into three types [6]: (1) large right posterior arch and small left anterior arch (right dominant aortic arch), accounting for 75%; (2) small right rear arch and large left front arch (left dominant aortic arch), accounting for approximately 20%; (3) and equal diameter DAA (balanced type aortic arch), accounting for 5%.
Clinical presentation depends largely on the existence of hemodynamic instability. Children with DAA tend to present earlier than those with the other vascular ring pathology. However, it may remain undiagnosed. Often, patients are identified as an incidental finding during routine imaging for other indications, and in some studies some patients are diagnosed after foreign body ingestion, and in an adult with aortic dissection [3].
Due to the anatomic nature of the lesion, DAA may manifest with symptoms of stridor, dyspnea, cough, and recurrent respiratory infections. In addition to airway symptoms, and related to esophageal compression, patients may experience swallowing difficulties, which manifests as vomiting and feeding intolerance. Life-threatening episodes of reflex apnea with cyanosis have being described [2].
Physical examination may often be entirely normal. Sometimes it can include evidence of poor growth and feed intolerance, non-positional stridor, respiratory distress, and features of a lower respiratory infection such as bronchial breath sounds and crackle [7].
Imaging remains the mainstay of investigation
Echocardiography is a readily available non-invasive technique that has proven useful in investigation of the heart. It may reliably image the aortic arch and its branches [8]. In addition, it can identify other intra-cardiac anomalies that may also be present. Electrocardiographic studies are normal unless intra-cardiac structural anomalies are co-existent. Chest X-ray can reveal loss of aortic knob, lateral/posterior indentation of the trachea [3]. Esophagography or barium swallow used to be the gold standard for diagnosis. It shows esophagus left- and right-sided indentations from the vascular compression [9].
However, advanced imaging using computed tomography (CT) or magnetic resonance imaging (MRI) has become the diagnostic procedure of choice. Computed tomography angiography with three-dimensional reconstruction is an excellent non-invasive imaging technique that is used to diagnose and characterize vascular rings. Using this technique, the exact anatomy of the aortic arch malformation and its relationship with adjacent structures can be precisely defined, which can assist the cardiovascular surgeon in planning surgical management. It points the exact locations and extent of airway and esophageal obstructions, and can provide a comprehensive picture of arterial branching patterns [10].
So due to the increasing speed of CT scans (10 to 20 seconds vs. 30 to 45 minutes required for a sedated MRI), the fact that CT scans are relatively insensitive to motion and metal and also the reconfiguration of the CT scan as a three-dimensional image, CT is largely preferred over MRI for the diagnosis of DAA [7].
Bronchoscopy usually occurs pre-operatively to evaluate airway anatomy. It also helps to exclude other causes of airway obstruction, to confirm and to grade the severity of airway compression [11].
Surgical repair is the only treatment allowing to eliminate tracheoesophageal compression [12].
Therefore, in addition of being indicated for patients with symptoms of tracheal and/or esophageal compression, it can remain as a supplementary procedure in patients undergoing repair of other cardiothoracic abnormalities [3].
The principle of surgery is the division of the lesser arch, so it can relieve the vascular compression on the trachea and/or esophagus [2].
Long-term prognosis for patients with repaired double aortic arch is excellent, and the most common adverse outcomes are persistent respiratory symptoms [4].
Conclusion
Double aortic arch (DAA) is the most common type of vascular ring malformation, a class of congenital anomalies of the aortic arch system. There has been no predilection in sex documented in patients with double aortic arch. Due to limited data, no racial predilection is apparent. Double aortic arch may be clinically silent or manifest with symptoms due to the compression on trachea and/or esophagus. Computed tomography scanning is currently the diagnostic procedure of choice for vascular ring evaluation. Surgical repair remains the mainstay of treatment that is indicated for patients with symptoms.
REFERENCES
1.
Priya S, Thomas R, Nagpal P, Sharma A, Steigner M. Congenital anomalies of the aortic arch. Cardiovasc Diagn Ther 2018;8(Suppl 1):S26–44. [CrossRef]
[Pubmed]

2.
Alsenaidi K, Gurofsky R, Karamlou T, Williams WG, McCrindle BW. Management and outcomes of double aortic arch in 81 patients. Pediatrics 2006;118(5):e1336–41. [CrossRef]
[Pubmed]
3.
Tarmahomed A, Umapathi KK. Double Aortic Arch. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2020.
[Pubmed]
4.
Elumalai G, Senguttuvan E. Double aortic arch: Embryological basis and its surgical implications. Elixir Embryology 2016;100:38706–17.
5.
Wafy S. 'Vascular ring', the hidden congenital anomaly having symptoms that may mimic asthma: A case report. Egypt J Bronchol 2016;10:69–72. [CrossRef]
6.
Zhu X, Wu C, He Y, et al. 3D-Imaging evaluation of double aortic arch with MSCTA: A case report and mini-review. J Xray Sci Technol 2018;26(1):103–9. [CrossRef]
[Pubmed]
7.
Backer CL, Mavroudis C, Rigsby CK, Holinger LD. Trends in vascular ring surgery. J Thorac Cardiovasc Surg 2005;129(6):1339–47. [CrossRef]
[Pubmed]
8.
Hartenberg MA, Salzberg AM, Krummel TM, Bush JJ. Double aortic arch associated with esophageal atresia and tracheoesophageal fistula. J Pediatr Surg 1989;24(5):488–90. [CrossRef]
[Pubmed]
9.
Sahni D, Franklin WH. Vascular Ring Double Aortic Arch. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2020.
[Pubmed]
10.
Yang X, Ye J, Gao Z. Double aortic arch presenting with a foreign object in the oesophagus: A case report and imaging diagnosis. Cardiol Young 2017;27(8):1651–3. [CrossRef]
[Pubmed]
11.
Mokoka MC, Ullah K, Curran DR, O'Connor TM. Rare causes of persistent wheeze that mimic poorly controlled asthma. BMJ Case Rep 2013;2013: bcr2013201100. [CrossRef]
[Pubmed]
12.
Lemouakni S, Hassani A, Elyajouri H, et al. Double aortic arch: About two cases. [Article in French]. Pan Afr Med J 2017;27:273. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
El Harras Yahya - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Imrani Kaoutar - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Jerguigue Hounayda - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Latib Rachida - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Omor Youssef - Conception of the work, Design of the work, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2021 El Harras Yahya et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}