 |
Case Report
A rare case of urinary bladder paraganglioma documented by 18F-FDG PET-CT: Clinical and imaging features
1 Department of Nuclear Medicine, Ghent University Hospital, Ghent, Belgium
2 Department of Radiology, Ghent University Hospital, Ghent, Belgium
Address correspondence to:
Azzam Abdalla Ibrahim
MD, Corneel Heymanslaan 10, 9000 Ghent,
Belgium
Message to Corresponding Author
Article ID: 101196Z01AI2021
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Ibrahim AA, Schandevyl SV, Smeets P, Goethals I. A rare case of urinary bladder paraganglioma documented by 18F-FDG PET-CT: Clinical and imaging features. Int J Case Rep Images 2021;12:101196Z01AI2021.ABSTRACT
Paragangliomas are extra-adrenal neural crest-derived neoplasms. Hybrid imaging allows for localization, preoperative planning and whole-body assessment. A rare case of urinary bladder paraganglioma is presented. In addition, in this case report, we highlight the selection of the appropriate radioactive tracer in the light of mutations.
Keywords: 18F-FDG PET-CT, Radionuclide imaging, Somatostatin receptor, Vesicular paraganglioma
Introduction
Catecholamines producing neuroendocrine tumors (NETs), pheochromocytomas, and paragangliomas (PPGLs) are rare and originate from adrenal medulla chromaffin cells (pheochromocytoma) or from neural crest-derived paraganglion cells situated in the region of the autonomic nervous system ganglia and accompanying nerves (paragangliomas).
The histology of paragangliomas is similar to that of pheochromocytomas, however, there is a higher tendency to metastasizing compared to pheochromocytoma. Increased levels of catecholamines in functional tumors account for the characteristic clinical manifestations, particularly elevated blood pressure, headache, palpitations, and diaphoresis.
The current WHO classification of endocrine tumors classifies paragangliomas in two categories: (1) head and neck paraganglioma and (2) sympathetic paraganglioma [1] (see also Table 1).
Paragangliomas occur in patients with a wide age range and there is a female predilection. One-third of paragangliomas are estimated to be hereditary with a higher prevalence of mutations in young patients. In general, PPGLs are divided into four molecularly defined subgroups: (1) the kinase signaling subtype, (2) the Wnt-altered subtype, (3) the cortical admixture subtype, and (4) the pseudohypoxia subtype. The pseudohypoxia subtype further comprises two main subgroups: the tricarboxylic acid cycle (TCA)-related PPGLs, in which mainly the succinate dehydrogenase subunits are involved/affected, and the von Hippel–Lindau (VHL)/endothelial PAS domain-containing protein 1 (EPAS-1)-related PPGLs [2].
Succinate dehydrogenase mutations (SDH) or (SDHx) account for 20% of all PPGLs. There are five subtypes: succinate dehydrogenase subunit A (SDHA), B (SDHB), C (SDHC), D (SDHD), and AF2 (SDHAF2), of these SDHD and SDHB are the most common (60% of the cases).
Succinate dehydrogenase subunit B (SDHB) mutations (10% of all PPGLs) are correlated with an increased malignant transformation (31–71%) and retroperitoneal localization [3]. Other solid tumors such as gastrointestinal stromal tumors, pituitary adenomas, and clear cell renal cell carcinomas have been associated with these familial PPGL syndromes [3].

Case Report
A 21-year-old man presented to the emergency room with increasing thunderclap headaches, palpitations, sweating, pallor, and anxiety after micturition. The symptoms were present for two months. Clinical examination was negative. The differential diagnosis may include (intermittent) cerebral/subarachnoid hemorrhage, due to primary or secondary hypertension, the latter related to the use of medications or illicit drugs that may increase catecholamine and metanephrine blood levels. Also psychiatric disorders such as alcohol withdrawal syndrome or anxiety disorders with panic attacks must be considered. However, when the above-mentioned typical symptoms occur during/shortly after micturition, the diagnosis of a urinary bladder paraganglioma is preferred. This was further investigated performing the following examinations:
Laboratory tests which showed a markedly increased urinary noradrenalin of 414 mcg/24 hours (normal range, 8–100 mcg/24 hours) and plasma normetanephrine of 5540 pmol/L (normal range, 48–495 pmol/L).
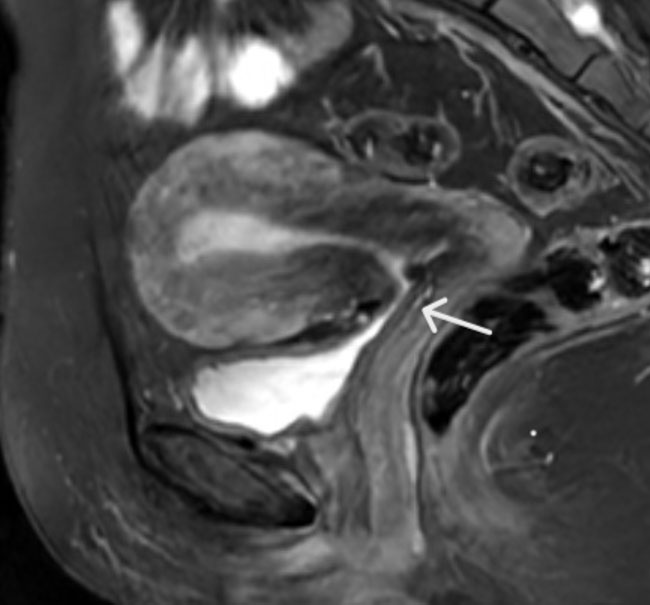
Even though the diagnosis of urinary bladder paraganglioma was highly probable, 123I-metaiodobenzylguanidine (MIBG) and 111In-pentetreotide scintigraphy (single-photon emission computerized tomography or SPECT) were negative/normal. Adrenal magnetic resonance imaging (MRI), to exclude a pheochromocytoma, was also negative. On the other hand, on ultrasound, cystoscopy, and 18F-fluorodeoxyglucose (FDG) positron emission tomography-computed tomography (PET-CT) scan a bladder mass was seen. On PET-CT scan, the mass (30 × 20 mm, Figure 1 and Figure 2) was intensely FDG–avid and located in the left upper wall of the bladder (Figures 1 and 2). On computed tomography (CT), the detrusor muscle appeared invaded by a heterogeneously contrast-enhancing soft-tissue mass, indicative of a richly vascularized tumor (Figure 2).
The mass was removed applying minimally invasive, robot-assisted laparoscopic surgery without opening of the bladder wall. Pathology confirmed complete resection of a vesicular paraganglioma with the typically light-microscopic appearance of a paraganglioma: a nesting pattern of epitheloid cells separated by discrete fibrovascular septa (Zellballen). Immunohistochemical staining for chromogranin, synaptophysin, neuron-specific enolase (NSE), and sustentacular cells (S-100) was positive. Additional molecular diagnostics revealed a SDHB mutation (autosomal dominant inheritance). Hence, genetic testing was recommended for (a) symptomatic first-degree relatives.
Follow-up 18F-FDG PET-CT at 1 year after surgery was unremarkable. Also, a repeat 3-year 68Ga-DOTA-NOC PET-CT was negative.


Discussion
Based on the clinical manifestations in our case, a functional PPGL is suspected. Particularly, a functional PPGL localized in the bladder wall is highly probable because the typical symptoms such as thunderclap headaches, hypertension, and palpitations occur only during/shortly after micturition. As such, the typical symptoms in our case are due to the release of massive catecholamines in the blood stream, which are caused by compression of the tumor by a contracting detrusor muscle during micturition [4].
Diagnosis is further confirmed by an elevated 24-hour normetanephrine level, ultrasound, and cystoscopy. It is noteworthy that the bladder is an unusual location (less than 1%) but due to the typical symptoms of a hypertensive crisis associated with micturition, the diagnosis is straightforward.
Imaging, and in particular hybrid PET-CT imaging, is performed to rule out multiple tumors and distant metastases [5].
On CT, paragangliomas are typically observed as heterogeneous soft tissue masses (attenuation greater than 10 Hounsfield units) with intense contrast enhancement, reflecting the high vascularization. An intermediate to high signal intensity is seen on T2-weighted MRI, with post-gadolinium enhancement on T1-weighted MRI [6],[7].
Radioisotope imaging is more sensitive for whole-body assessment/screening than anatomical imaging. It is specific for PPGL, may visualize these tumors in unusual locations, and can identify patients who may benefit from (radionuclide) therapy.
On scintigraphy, metaiodobenzylguanidine (MIBG) which is radiolabelled with 123I or 131I acts as a norepinephrine analog which is internalized by the sympathetic paraganglioma cells. 123I MIBG scintigraphy is preferred over 131I MIBG scintigraphy because it provides a better image quality, has a lower radiation burden which allows higher permissible administered activity and as a result a higher count rate. Moreover, 123I is technically easier to perform with less time between injection and imaging, 24 hours for 123I MIBG compared with 48–72 h for 131I MIBG scintigraphy. Pentetreotide is a diethylenetriaminepentaacetic (DTPA) conjugate of octreotide and a long-acting somatostatin analogue (SSA). [111In] DTPA-pentetreotide specifically binds to the somatostatin receptors (SSTRs), particularly the subtypes 2 and 5, that are overexpressed on the cell membranes. Therefore, both tracers are suited for imaging PGGL. However, the sensitivity of 123I-MIBG or 111In-pentetreotide scintigraphy is lower than that of PET-(CT), mainly because of an inferior SPECT resolution compared to PET.
The choice of the most appropriate PET radiotracer for imaging PPGLs can be challenging.
18F-fluoro-l-dopa (FDOPA) (PET-CT) is taken up by the tumor cells of PPGLs. In the cell, 18F-FDOPA is decarboxylated, converted into [18F] fluorodopamine ([18F] FDA) by L-aromatic amino acid decarboxylase (AADC) and stored in the neurosecretory vesicles of the catecholamine-producing cells [7]. This means that there is selective tracer accumulation in the tumor cells, which enhances the contrast between a low background and the tumor. Moreover, the resolution of PET is superior to that of SPECT and the high three-dimensional acquisition yield renders excellent quality PET whole-body images that significantly improve image interpretation in comparison with SPECT. It is also worth mentioning that certain medications do not need to be discontinued which is the case for 123/131I MIBG imaging. All of the above make 18F-FDOPA PET-CT the first choice for imaging pheochromocytomas and head and neck paragangliomas with a sensitivity of >90% for head and neck PPGL and almost 100% for pheochromocytoma, the latter due to the limited uptake of the tracer by normal adrenal glands [7],[8].
However, sensitivity in retroperitoneal paragangliomas may be decreased by the physiological uptake in the pancreas [9]. Furthermore 18F-FDOPA PET-CT sensitivity in PPGLs related to SDHx mutations is lower than in non-SDHx mutated PPGLs [7],[9],[10],[11].
The PET tracer 68Ga-DOTA, which targets the SSTR2 that is most commonly overexpressed in PPGLs, may also be used. This PET tracer is also internalized into the cells. Recent studies show that 68Ga-DOTA is likely superior to other radiopharmaceuticals for patients with extra-adrenal PPGLs [7],[12]. Recently published data in patients with extra-adrenal PPGLs, 68Ga-DOTA PET-CT showed better patient-based and lesion-based detection rates than did 18F-FDOPA PET-CT (98% vs. 95% and 99% vs. 68%, respectively) [7]. Furthermore, 68Ga-DOTA PET-CT may allow optimization of targeted radionuclide therapy with 177Lu-DOTA-TATE.
As is the case for 18F-FDOPA, availability and cost of 68Ga-DOTA are often an issue. Moreover, in the United States, these tracers can only be used in the context of clinical trials [7],[12].
Contrarily, the wide availability and relatively low cost of 18F-FDG makes it a reasonable first choice, especially in SDHx mutated paragangliomas. The better 18F-FDG avidity in SDHx is explained by the accumulation of succinate due to blockade of the Krebs cycle, which results in what is called “pseudohypoxia.” This phenomenon results in a higher glucose uptake and consumption due to increased glycolysis despite normal oxygen supply [13]. The sensitivity is particularly high for PPGLs associated with SDHB mutations (sensitivity per lesion of 83% for SDHB-positive tumors vs. 62% for SDHB-negative tumors), compared to 18F-FDOPA (sensitivity of 93% for SDHB negative vs. 20% for SDHB positive) [7],[9],[14].
Upon presentation of our patient at our hospital, 68Ga-DOTA and 18F-FDOPA PET were not available, which explains why, after a negative 123I-MIBG scintigraphy, 18F-FDG PET-CT was performed.
Conclusion
68Ga-DOTA-SST analogue PET-CT and 18F-FDOPA PET-CT are considered the first choice for imaging patients with suspected paraganglioma. However, availability and cost can be problematic. 18F-FDG PET-CT is a reasonable alternative because it is widely available and relatively less costly. In addition, 18F-FDG is an appropriate PET tracer for SDHx-mutated PPGLs.
REFERENCES
1.
Lloyd RV, Osamura RY, Kloppel G, Rosai J. WHO Classification of Tumours of Endocrine Organs. Lyon: IARC Press; 2017.

2.
Fishbein L, Leshchiner I, Walter V, et al. Comprehensive molecular characterization of pheochromocytoma and paraganglioma. Cancer Cell 2017;31(2):181–93. [CrossRef]
[Pubmed]
3.
Cascón A, Remacha L, Calsina B, Robledo M. Pheochromocytomas and paragangliomas: Bypassing cellular respiration. Cancers 2019;11(5):683. [CrossRef]
[Pubmed]
4.
Beilan JA, Lawton A, Hajdenberg J, Rosser CJ. Pheochromocytoma of the urinary bladder: A systematic review of the contemporary literature. BMC Urol 2013;13:22. [CrossRef]
[Pubmed]
5.
Antonio K, Valdez MMN, Mercado-Asis L, Taïeb D, Pacak K. Pheochromocytoma/paraganglioma: Recent updates in genetics, biochemistry, immunohistochemistry, metabolomics, imaging and therapeutic options. Gland Surg 2020;9(1):105–23. [CrossRef]
[Pubmed]
6.
Canu L, Van Hemert JAW, Kerstens MN, et al. CT Characteristics of pheochromocytoma: Relevance for the evaluation of adrenal incidentaloma. J Clin Endocrinol Metab 2019;104(2):312–8. [CrossRef]
[Pubmed]
7.
Taïeb D, Hicks RJ, Hindié E, et al. European Association of Nuclear Medicine Practice Guideline/Society of Nuclear Medicine and Molecular Imaging Procedure Standard 2019 for radionuclide imaging of phaeochromocytoma and paraganglioma. Eur J Nucl Med Mol Imaging 2019;46(10):2112–37. [CrossRef]
[Pubmed]
8.
Taïeb D, Jha A, Guerin C, et al. 18F-FDOPA PET/CT imaging of MAX-related pheochromocytoma. J Clin Endocrinol Metab. 2018;103(4):1574–82. [CrossRef]
[Pubmed]
9.
Treglia G, Cocciolillo F, de Waure C, et al. Diagnostic performance of 18F-dihydroxyphenylalanine positron emission tomography in patients with paraganglioma: A meta-analysis. Eur J Nucl Med Mol Imaging 2012;39(7):1144–53. [CrossRef]
[Pubmed]
10.
Taïeb D, Sebag F, Barlier A, et al. 18F-FDG avidity of pheochromocytomas and paragangliomas: A new molecular imaging signature? J Nucl Med 2009;50(5):711–7. [CrossRef]
[Pubmed]
11.
Timmers HJLM, Kozupa A, Chen CC, et al. Superiority of fluorodeoxyglucose positron emission tomography to other functional imaging techniques in the evaluation of metastatic SDHB-associated pheochromocytoma and paraganglioma. J Clin Orthod 2007; 16. [CrossRef]
[Pubmed]
12.
Lenders JWM, Duh QY, Eisenhofer G, et al. Pheochromocytoma and paraganglioma: An endocrine society clinical practice guideline. J Clin Endocrinol Metab 2014;99(6):1915–42. [CrossRef]
[Pubmed]
13.
Taïeb D, Pacak K. New insights into the nuclear imaging phenotypes of cluster 1 pheochromocytoma and paraganglioma. Trends Endocrinol Metab. 2017;28(11):807–17. [CrossRef]
[Pubmed]
14.
Timmers HJLM, Chen CC, Carrasquillo JA, et al. Staging and functional characterization of pheochromocytoma and paraganglioma by 18F-fluorodeoxyglucose (18F-FDG) positron emission tomography. J Natl Cancer Inst 2012;104(9):700–8. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Azzam Abdalla Ibrahim - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Steven Van Schandevyl - Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Peter Smeets - Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Ingeborg Goethals - Conception of the work, Design of the work, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2021 Azzam Abdalla Ibrahim et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}